Your research belongs at EACVI 2026. 📢
The Call for Science is still open — and this year brings expanded opportunities to showcase your work in front of the global cardiovascular imaging community.
🗓️ Key deadlines:
→ Abstract submission: 21 May 2026
→ Clinical Case submission: 2 June 2026
→ Late-Breaking Science: 29 September 2026
EACVI 2026 takes place 3–5 December in Milan, uniting EuroEcho, EuroCMR and ICNC-CT in one landmark multimodality congress.
Submit today → https://t.co/M2vCqCniui
#EACVI26 #CardiovascularImaging #CallForAbstracts #Cardiology
🚨 Out now in Clinical Cardiology! Our new review maps the incredible 10-year rise of Cardiac MRI in ESC guidelines.
🧲🫀 Once an adjunctive test, CMR is now a foundational, Class I/IIa test for cardiomyopathies, MINOCA, & more! 📈 https://t.co/3IYChpA3G0 #CardioTwitter#CMR
🚨Funded PhD at @uniofeastanglia on stroke risk in AF: why do some have stroke but others do not? Combines imaging, physiology & platelet biology for personalised prevention. ⏰Deadline 31 Mar 2026. Home fees + stipend. Intl applicants pay fee difference. https://t.co/DoG3tFfDso
🫀 Standard echo & 2DPC CMR can underestimate aortic regurgitation in patients with heart rate variability. Our new case report demonstrates how 4D-flow CMR reclassified AR severity from mild-mod to mod-severe (RF 38%), guiding timely intervention! 📊 Read the full case below 👇
The nature is smart
Blood doesn’t crash into the LV, it glides.
The anterior mitral leaflet quietly shapes inflow into a smooth arc, guiding it straight toward the LVOT.
Less turbulence. Less wasted energy. Elegant design.🍷🍷
❤️ 🧲Where you measure matters: 4D flow CMR quantification of mitral regurgitation is most reliable near the vena contracta—standardization is key.
pdf 👉 https://t.co/W8jQRVZUj8
Dr. Jeesoo Lee explains below 👇
#WhyCMR
The Right Heart is NOT just a passive conduit. 🌊🫀
Our latest review in #EHJIMP describes how 4D Flow CMR reveals what standard imaging misses: RA vortex formation conserves energy, while PH destroys efficient flow (↓Direct Flow, ↑Residual Volume).
https://t.co/BTaEpOtps0
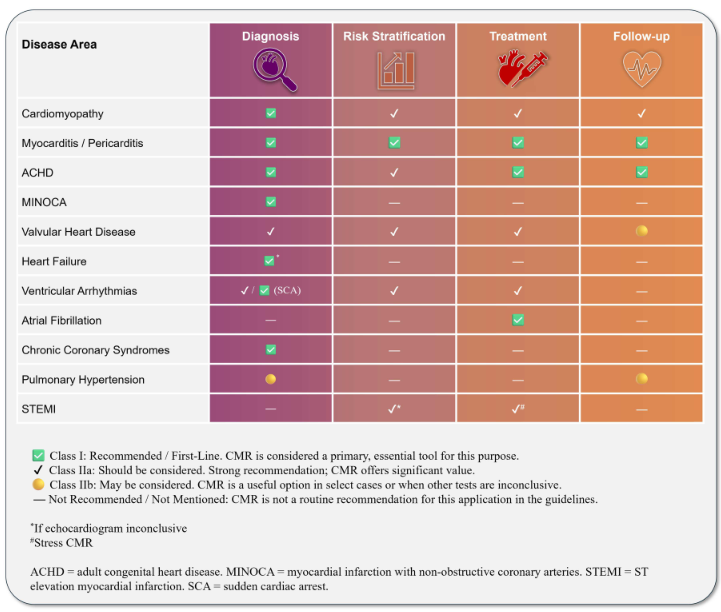
#EHJCVI 🧲 Is CMR redefining timing in chronic aortic regurgitation? A meta-analysis (~2,000 pts) shows CMR-derived AR fraction >33% is linked to ~4× higher risk, even in asymptomatic patients. CMR sharpens risk stratification beyond echo 👉 https://t.co/PB41reus88
Is 33% the new magic number in AR? 🤔🫀
Our #EHJCI meta-analysis (n=1,996) shows a CMR Regurgitant Fraction >33% predicts a 4-fold risk of adverse outcomes & surgery (HR 4.12).
Time to rethink intervention thresholds? 📉🧲https://t.co/0ki4J8gMTe #CMR@HEARTinMagnet
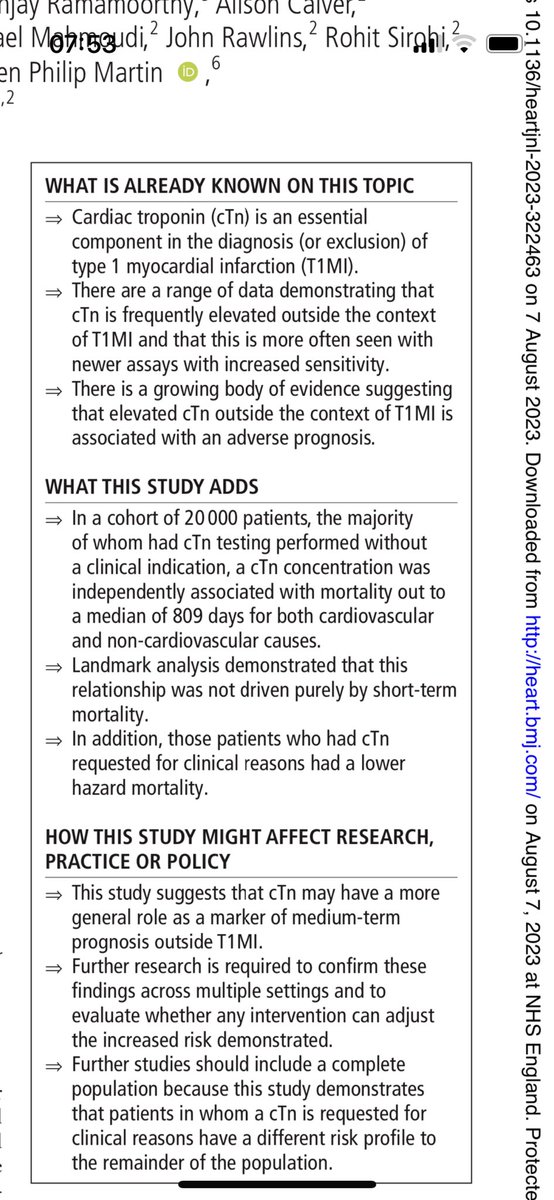
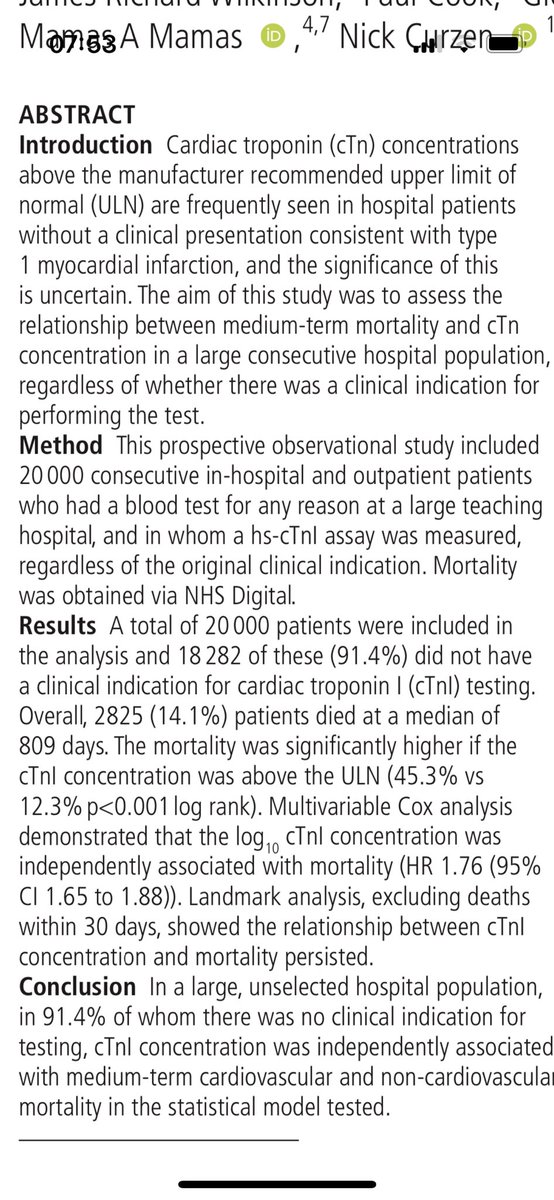
If you take a random troponin in 20k consecutive patients having a blood test for any reason (in 91% there was no clinical indication for hsTrop) then the result is associated with medium term mortality- both CV & nonCV… fascinating? @mmamas1973 @JonathanWHinton
It's the plaque rupture that causes the heart attack.
But you need plaque in the first place to rupture, and typically plenty of it.
The onset of plaque can be delayed to much later in life with aggressive risk factor control.
Thanks to @cardiologyoncal
Great day presenting at #ESCCongress 2022, detailing cardiac complications of Lemierre's and the importance of multimodality imaging and utilising the MDT. @escardio@DrChrisMcAloon
📷: @jgraby
At #ESCCongress 2022? Fancy hearing about an interesting cardiac manifestation of Lemierre's syndrome? Join me in Clinical Case Corner tomorrow at 13.25! @escardio@DrChrisMcAloon
Last shift at the BRI ✅ (for now...?)
Last shift as an SHO ✅
Onwards and upwards, @gloshospitals here we come. Definitely looking forward to a new challenge! #IMT3#IMT3isthenewST3