@DrTeslaFSD Finished ~350 miles today (1 SC stop) with the family in the Juniper and similarly used FSD the entire time. It makes the drive much more pleasant. I couldn’t imagine going back to manually driving.
@TheShreddington@ironnfox Roadtrips work when there’s a nearby charger at your destination. If nothing nearby there’s more thought that goes into keeping it charged than ICE car.
My wife finds the sunlight coming through glass roof too much.
It’s absolutely phenomenal.
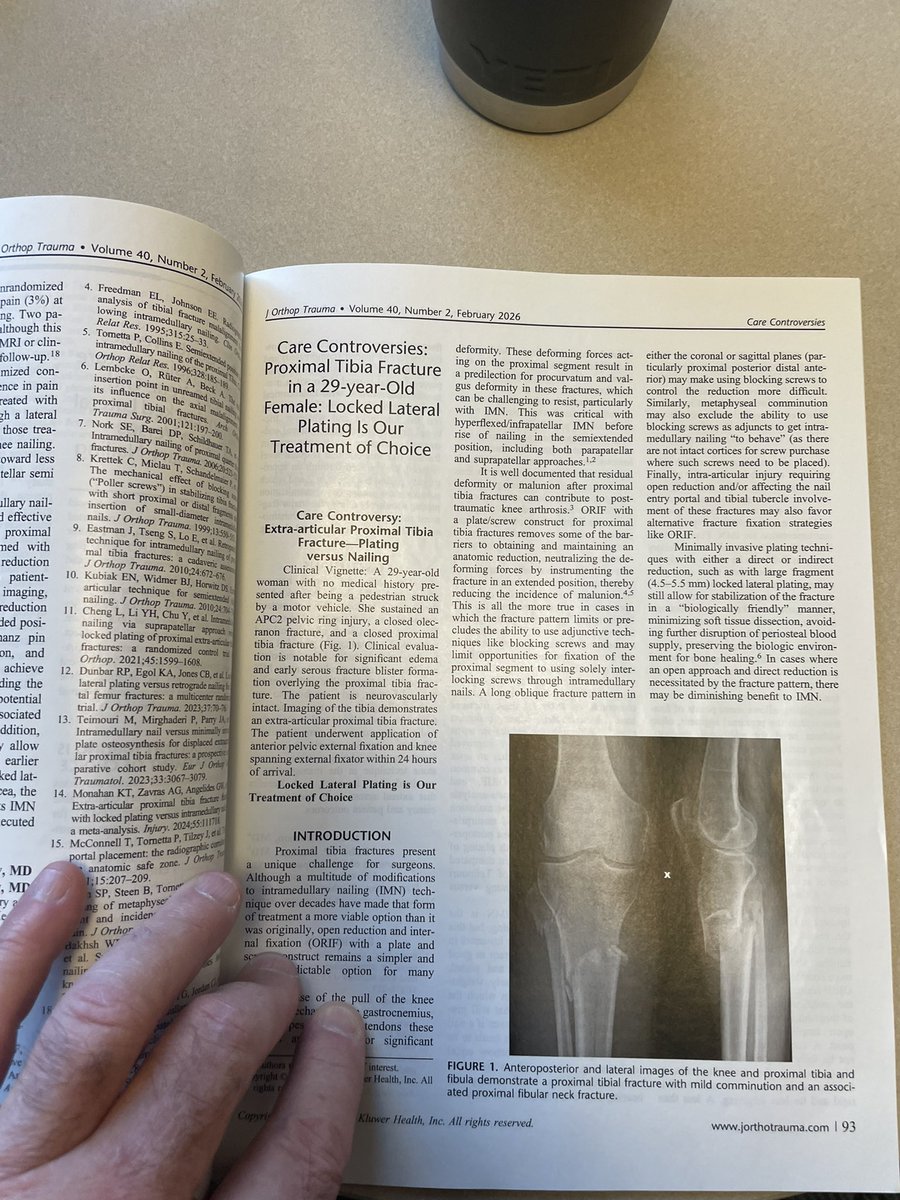
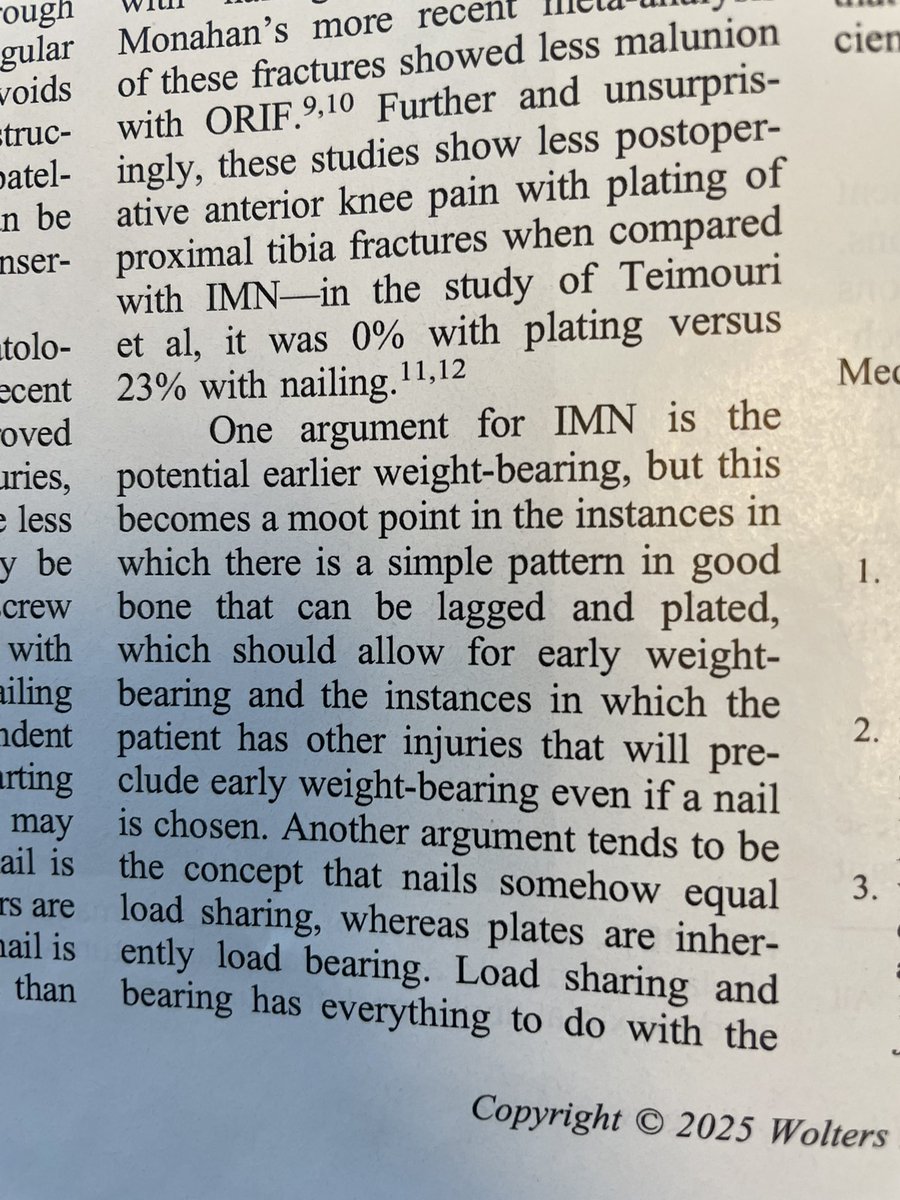
So, the whole Nail = load sharing & plate = has always seemed like b.s. to me but I never saw it written anywhere (maybe I just couldn’t find). So I wrote it (w/LS). Generations of residents (& attendings) have parroted this. No more.
@DrBhavinJadav I agree that fixing the deltoid provides stability. I personally find it difficult to reconcile the isometry to optimize outcomes. Anecdotally when fixed, ankles end up stiff. I’m not sure if it’s the lack of motion out of the gate, the injury, over tensioned repair, etc.
I’ve been an orthopedic surgeon for nearly 30 years, and a few patterns have become impossible to ignore. One is that many musculoskeletal problems in adults aren’t sudden injuries. They’re the moment when declining capacity and awful metabolic health finally reveals itself.
Over the decades your strength fades, muscle mass declines, as your aerobic capacity tanks. Tendons and connective tissues lose substance, stiffness, and resilience. For years the body compensated... quietly. Then one day a knee hurts during a run to get the train, or shoulder aches reaching overhead, or a back tightens lifting something simple.
At that point the story usually becomes more about structural damage. An MRI gets ordered. Welcome to high-tech, low-medicine. And the MRI almost always finds something. A meniscus tear. A rotator cuff tear. A disc bulge. Why? Because by midlife these findings are extremely common — even in people with no pain at all. If you have a tear in one shoulder, image the other shoulder... you probably have the same tear there. But I digress.
Once the scan appears, the narrative changes. The image becomes the diagnosis. Now the patient believes something is broken, and the focus often shifts to fixing what the MRI shows.
What often gets lost in this is the reason the symptoms appeared in the first place. Many so-called “atraumatic” orthopedic complaints are not purely mechanical failures. They are the moment when reduced strength, declining tissue capacity, and sometimes broader metabolic health issues finally reach a tipping point. Our tissues change over the decades... get over it.
In other words, the MRI didn’t create the problem. Well... it sort of did in this scenario. But all the MRI showed was something that was already there.... because of your age, lifestyle, health and so on.
The real driver of symptoms is often loss of physiologic reserve. Less muscle. Less tendon or aerobic resilience. Less tolerance for load, etc.
Once the MRI enters the picture, the risk becomes overtreatment. This is probably the number one reason people have surgery. When in many cases the most powerful intervention was never the scan or the procedure.
It was rebuilding capacity.
Strong muscles stabilize joints. Aerobic fitness improves metabolic health and tissue perfusion. Gradual loading restores tolerance.
But people often don't take PT seriously prior to surgery. They often take PT very seriously afterwards. Therefore, PT is probably the reason you feel better, despite the surgery.
The irony is that the treatment many people ultimately need is the same thing that might have prevented the problem in the first place.
Staying strong. Staying active. Maintaining the reserve that protects our joints/tendons/muscles/abilities as we age.
@AbudBakri@getchroma How long are you using on the D mode (UVB)?
I’m waiting to have my VitD levels drop down before utilizing it more than a minute or two daily.
I’m eager to try this as we get closer to summer.
It’s an easy flag for AI especially given findings are dictated/interpreted within context, eg severe, moderate, mild, and recommendations are often provided in the report.
Eg. Incidental nodule seen, recommend repeat CT in 3 months. Flag it, send report to patient/PCP/ordering doc, send repeat flag/reminder in 3 months.
To play devils advocates - as a radiologist are you absolving yourself of taking care of patients? You’re being paid for a job, even if subcontracted. Seems like a great place for AI automation.
Which scenario leads to better patient care? A phone call from someone who understands what they’re seeing or said ortho telling them about incidental findings and recommending follow up through their PCP/providing specialist referral.
I’ve had the unfortunate pleasure of fixing a similar fractures 2 weeks out. Same neck of the woods as well. I’ve also seen femoral necks, femoral shafts and even an unstable intercondylar-supracondylar distal femur “walk in” to clinic. It’s not right on so many levels and the patient suffers the most.