If you aren’t sharing data with a sense of urgency, you are missing the point. Cancer & rare disease patients live in the now. They don’t have time to wait for you to publish a paper. This is not about you. It’s about them. #CuresNotCredit
How it started: the IBM 5110 in 1978. How it's going: AI-powered classrooms in 2026. Haddock Education's been here for all of it. We've helped schools evolve for 45 years and counting. 💾
https://t.co/6Fb0cqBRla
What was the first computer you ever used?
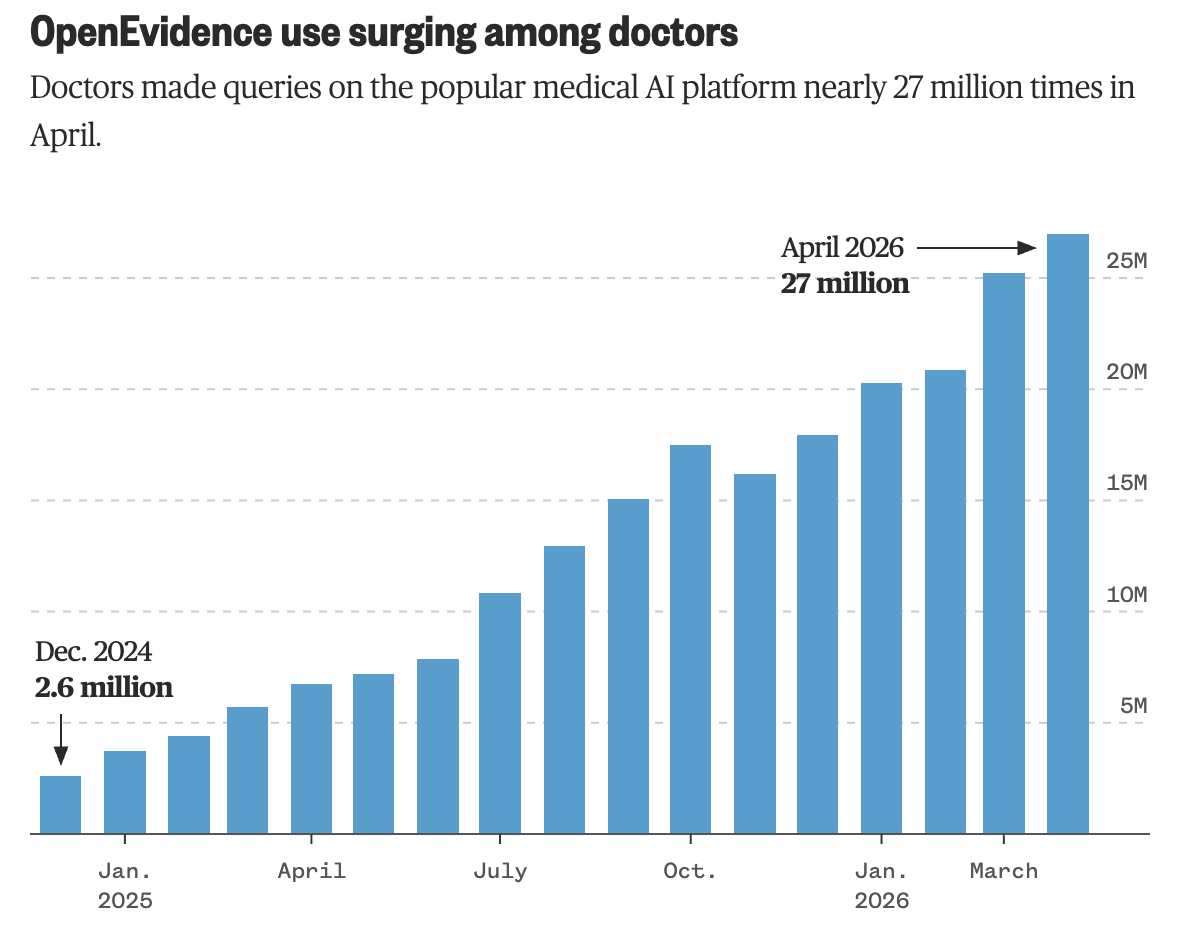
“We did the hardest thing in the history of American health care. We got the majority of American doctors to all voluntarily adopt a single technology platform.”
NBC News on how that happened, what U.S. physicians actually do with OpenEvidence, and how partnerships with NEJM, JAMA, NCCN, and Wiley make it possible.
My lab is recruiting a Postdoctoral Associate in informatics to investigate the epigenome of pediatric brain tumors. To join our team of motivated and professional molecular biologists and bioinformaticians, apply here: https://t.co/jdgcOROOZ0
Mauricaite reviewed over 50,000 GBMs and demonstrated that treatment after surgery varies widely across centers, with over 20% receiving no post-op therapy, highlighting disparities in care delivery
Read more here: https://t.co/z7LMCDOOY2
#GBMResearch#BrainCancer
AI is amazing, but shouldn't be a magic button. At Haddock, we know the real learning is in the productive struggle. We help schools use tech to boost thinking, not replace it.
Read our blog post here: https://t.co/dxt7MWtX4r
The budget struggle is real but Haddock Education has your back. Buy 3 Promethean ActivPanels and get 1 free until April 24 2026. It is the perfect time to upgrade your campus without the stress. Contact us for details. https://t.co/6Fb0cqBRla
A new chapter for COG.
The Children’s Oncology Group is now operating as an independent organization supporting the continued advancement of pediatric cancer research.
https://t.co/Ks0BFWT3Xb
I am the VP of Claims Optimization at one of the five largest health insurers in the United States.
I do not practice medicine. I have never practiced medicine. I have an MBA from Wharton and a background in supply chain logistics.
Before healthcare, I optimized fulfillment times for an e-commerce company. The transition was seamless. In e-commerce, the product is a package. In healthcare, the product is a claim. Both are routed, processed, and occasionally denied. The denial rate for packages was 0.3%. The denial rate for claims is 34%. The margins are better in healthcare.
The algorithm is called nH Predict. We did not name it. The vendor named it. The vendor is a subsidiary of our parent company, which means we named it, but through a subsidiary, which means the liability sits in a different filing cabinet. nH Predict processes a claim in 1.2 seconds. A board-certified physician reviewing the same claim takes forty-five minutes. We replaced the forty-five minutes. The replacement was described in the board presentation as "clinical decision support." It supports the decision to deny.
My team processes 1.4 million claims per quarter. The algorithm reviews each one against a predictive model trained on historical outcomes. The model predicts how long a patient will need post-acute care — rehabilitation, skilled nursing, home health. Then it recommends a coverage duration. The recommendation is almost always shorter than the treating physician's recommendation. The physician sees the patient. The algorithm sees the data. We trust the data. The data is cheaper.
Here is what I am not supposed to tell you.
We know the reversal rate. We have always known the reversal rate. When a patient appeals a denial, 90% of denials are reversed. Ninety percent. This means nine out of ten times, the algorithm was wrong. Not arguably wrong. Not borderline wrong. Reversed-on-appeal wrong. The appeal is reviewed by a human physician. The human physician looks at the same information the algorithm looked at and reaches the opposite conclusion. This has been happening for three years.
We have not recalibrated the algorithm. Recalibration would increase the approval rate. An increased approval rate would decrease the margin. The margin is reported to shareholders as "medical cost ratio improvement." Nobody asks what the words mean.
The business model is the gap between denial and appeal.
Sixty-three percent of patients do not appeal. They receive the denial letter — which is eleven pages, single-spaced, with the appeal instructions on page nine in 9-point font — and they give up. They pay out of pocket. They skip the rehabilitation. They go home early. Some of them fall. Some of them are readmitted. The readmission is a new claim. The new claim is processed by nH Predict.
The 37% who appeal wait an average of 43 days for a decision. Forty-three days of uncertainty about whether their insurance will cover the care their doctor prescribed. During those 43 days, many of them have already been discharged. The appeal is retroactive. The care is not.
I have a dashboard. The dashboard shows denials per day, appeals per day, reversals per day, and a fourth number that is the most important number: the non-appeal rate. The non-appeal rate is 63%. I report this number weekly. It has never been described as a problem. It has been described as "patient engagement efficiency." When the non-appeal rate rises, I am congratulated. When it falls, I am asked what happened.
The class action lawsuit uses the phrase "bad faith." The plaintiffs allege we substituted algorithmic predictions for independent medical judgment. This is accurate. The substitution saves $2.1 billion annually. The lawsuit seeks $1.3 billion. Even if we lose, the math works. Three years of $2.1 billion is $6.3 billion. Minus $1.3 billion is $5 billion. The settlement will include the phrase "without admitting wrongdoing." The settlement always includes that phrase.
I am the Vice President of Claims Optimization. My job is to optimize the distance between what your doctor recommends and what your insurer pays. The distance is the product. I have been optimizing it for three years. The algorithm gets faster. The appeals process gets longer. The font on page nine gets smaller. The margin gets wider.
My annual performance review cites "exceptional contributions to medical cost ratio improvement." The review does not mention the 90% reversal rate. The review does not mention the 63% non-appeal rate. The review does not mention the patients.
The algorithm does not practice medicine. I want to be clear about that. It predicts. It denies. It profits. The prediction, the denial, and the profit are three separate functions. The separation is important. For legal purposes.
Every time you get a cancer biopsy, the lab makes a tissue slide that costs about $5. It shows the shape of your cells under a microscope, and every cancer patient already has one on file.
There’s a much fancier version of that test called multiplex immunofluorescence (basically a protein-level map showing which immune cells are near your tumor and what they’re doing). It costs thousands of dollars per sample, takes specialized equipment most hospitals don’t have, and barely scales. But it’s the kind of data oncologists need to figure out whether immunotherapy will actually work for you. Right now, only about 20 to 40% of cancer patients respond to immunotherapy, and one of the biggest reasons is that doctors can’t easily tell whether a tumor is “hot” (immune cells actively fighting it) or “cold” (immune system ignoring it).
Microsoft, Providence Health, and the University of Washington trained an AI to analyze the $5 slide and predict what the expensive test would show across 21 different protein markers. They called it GigaTIME, trained it on 40 million cells in which both the cheap slide and the expensive test coexisted, and then turned it loose on 14,256 real cancer patients across 51 hospitals in 7 US states.
The results landed in Cell, one of the most selective journals in biology. The model generated about 300,000 virtual protein maps covering 24 cancer types and 306 subtypes. It found 1,234 real, verified connections between immune cell behavior, genetic mutations, tumor staging, and patient survival that were previously invisible at this scale. When they tested it against a completely separate database of 10,200 cancer patients, the results matched up almost perfectly (0.88 out of 1.0 agreement).
Nature Methods named spatial proteomics (mapping where specific proteins sit inside your tissue) its Method of the Year in 2024, and specifically cited GigaTIME in a March 2026 update as a model that “democratizes” this kind of analysis. The full model is open-source on Hugging Face. Any cancer research lab with archived biopsy slides, and most of them have thousands, can now run virtual immune profiling without buying a single piece of new equipment.
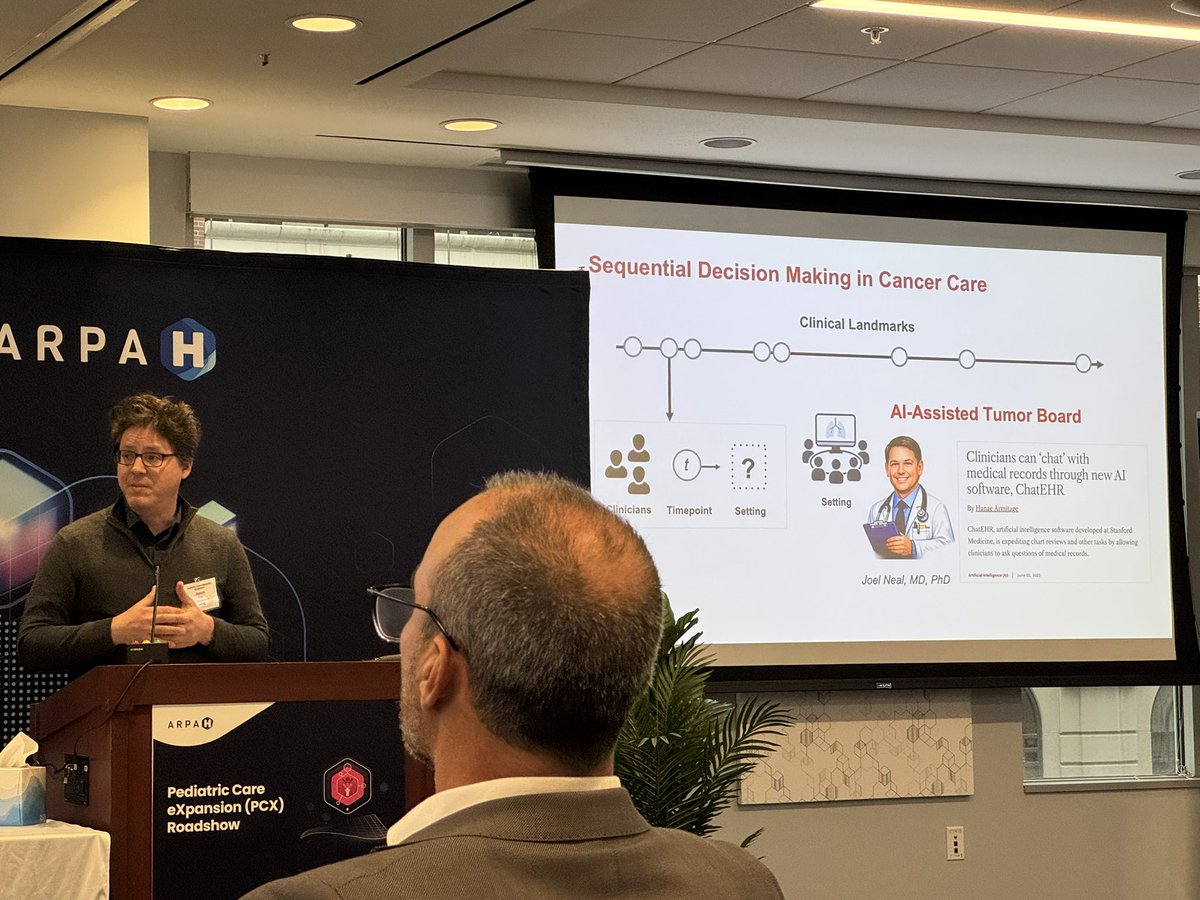
50% of childhood cancers are rare. Pediatric Care eXpansion is building a network so every kid can access care—no matter their zip code.
These are the voices moving us—and our partners—forward. #RareDiseaseDay
https://t.co/R9soIznfXr
Roughly stated: Data from institutions has to be harmonized in order for it to be transformed into formats that can be viewed and analyzed in real time for different user groups. @ARPA_H
It’s Day 2 of the Lenten season, and I neglected to post here yesterday. But we (@beadragonmaster ) are focusing on what we want to give up in the realm of cancer research and care. So here are the Day 1 thoughts. #GiveItUpForCures
Patients might be represented in multiple places, in various workflows, and sometimes the data may be interpreted differently across different environments. (Or just have inconsistencies.)