( عمل لا مثل له )
-قال أبو أمامة رضي الله عنه:
يا رسول الله، مرني بأمر ينفعني الله به.
قال ﷺ :"عليك ب #الصوم، فإنه لا مثل له".
وفي رواية: "لا عدل له".
رواه #النسائي.
وفي رواية: فما رُئي أبو أمامة، ولا امرأته، ولا خادمه، إلا صياما، فكان إذا رئي في دارهم دخان بالنهار، قيل: اعتراهم ضيف.
-وفي أول الحديث قال أبو أمامة: أنشأ رسول الله ﷺ غزوا، فأتيته، فقلت: يا رسول الله، ادع الله لي بالشهادة، فقال: اللهم سَلِّمْهُم، وغَنِّمْهُم، فغزونا، فسلمنا وغنمنا، ثم أنشأ غزوا آخر، فأتيته، فقلت: يا رسول الله، ادع الله لي بالشهادة، قال: اللهم سَلِّمْهُم، وغَنِّمْهُم، فغزونا، فسلمنا وغنمنا، ثم أنشأ غزوا آخر، فأتيته، فقلت: يا رسول الله، أتيتك تترى ثلاثا، أسألك أن تدعو الله لي بالشهادة، فقلت: اللهم سَلِّمْهُم، وغَنِّمْهُم، فغزونا، فسلمنا وغنمنا، فمرني يا رسول الله بأمر ينفعني الله به، قال: عليك بالصوم. . .".
The minimum ST elevation criteria for diagnosing STEMI in limb leads is:
a) ≥0.5 mm in 2 contiguous leads
b) ≥1 mm in 2 contiguous leads
c) ≥2 mm in 2 contiguous leads
d) ≥3 mm in 2 contiguous leads
#عيد_الأضحى يتبعه ثلاثة أيام تسمى #أيام_التشريق، وهي:
الحادي عشر، والثاني عشر، والثالث عشر.
يحرم صومها إلا لمن لم يجد الهدي من الحجاج.
حتى لو وافقت الاثنين أو الخميس، فإنه يحرم صومها.
-فالأيام التي يحرم صومها في السنة خمسة، هي:
يوم الفطر، ويوم الأضحى، وأيام التشريق الثلاثة.
(السؤال):
السلام عليكم .. متى يبدأ دعاء #يوم_عرفه بعد الزوال إلى الغروب؟ أو متى؟ وهل الترغيب في الدعاء خاص بالحاج أو عام له ولغيره؟
(الجواب):
-جميع النهار محل دعاء، لكن أفضله وأحراه يبدأ بعد الظهر إلى المغرب
كما فعل النبي ﷺ، حيث رفع يديه يدعو في #عرفة بعد الظهر حتى غربت الشمس.
يعني ظل النبي ﷺ رافعا يديه نحو ست ساعات ﷺ يدعو يدعو إلى الغروب.
وكان إذا سقط خطام ناقته أخذه بيده، ويده الأخرى مرفوعة.
-والترغيب في الدعاء في هذا اليوم عام للحاج وغير الحاج.
سئل #الإمام_أحمد عن الجلوس للدعاء يوم عرفة لغير الحاج فقال: لا بأس به، إنما هو دعاء وذكر.
وقال الشيخ الفوزان: "يشرع لغير الحجاج الاجتهاد في الدعاء ليشاركوا الحجاج في هذا الفضل، فالاجتهاد في الدعاء يوم عرفة لغير الحاج مشروع وفضيل".
Doppler stroke volume: simple physics, clinically powerful.
⚪Measure LVOT diameter (D) on 2D echo
⚪Calculate area assuming a circle: CSA = 3.14 × (D/2)²
⚪Trace LVOT Doppler to obtain VTI (distance blood travels in one beat)
Stroke volume = CSA × VTI
Conceptually, the LV ejects blood as a cylinder:
📍Base = LVOT cross-sectional area
📍Height = VTI from the velocity–time curve
(also approximates mean velocity × ejection time)
Key assumptions for accuracy:
- Precise diameter measurement (small errors are squared)
- Laminar flow with a relatively flat velocity profile
- Doppler beam aligned parallel to flow (angle ~0°)
- Diameter and VTI measured at the same anatomic site
Used for cardiac output, continuity equation, and hemodynamic assessment.
Reference: Catherine M Otto, textbook
🫀 #CardioNugget: Flail Gap vs Flail Width in MR
📍 Flail Gap
➡️ Distance between the flail leaflet tip and the coaptation line
➡️ Think: “How far is the leaflet flying into the LA?”
🔴 Larger gap = more severe MR
✅ MitraClip-friendly: <10 mm
📍 Flail Width
➡️ Medial–lateral extent of the flail segment
➡️ Think: “How wide is the damaged portion?”
🔴 Wider segment = more complex repair
✅ MitraClip-friendly: <15 mm
🎯 Why it matters?
Both help determine severity + feasibility of transcatheter repair (e.g., MitraClip)
#CardioNuggets #MedEd #TEE #MitraClip
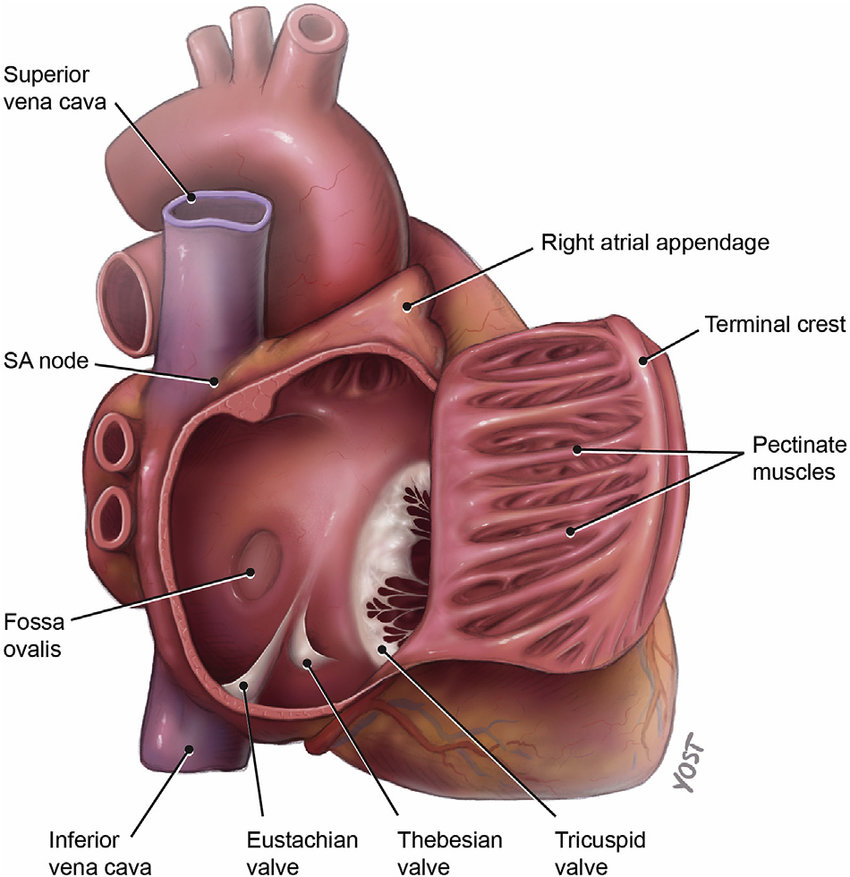
Apical 4-chamber view: a single window that maps cardiac anatomy and relationships.
How to obtain it:
🔵 Place the transducer at the point of maximal impulse (LV apex)
🔵 Keep the probe index marker directed toward the patient’s left side (≈3 o’clock)
🔵 Aim the beam toward the base of the heart (toward the right shoulder)
🔵 Fine-tune tilt/rotation until all four chambers are symmetric and the septum is vertical
From the LV apex, you see all four chambers in one plane (LV, RV, LA, RA) with correct orientation (apex near the probe, atria deeper).
Key structures:
🔵 LV: papillary muscles, chordae, anterior & posterior mitral leaflets
🔵 RV: moderator band, anterior & septal tricuspid leaflets
🔵 Interatrial septum and ventriculoatrial septum (LV–RA separation)
🔵 Right superior pulmonary vein entering the LA near the septum
🔵 Descending aorta seen posterior/lateral to the LA
High-yield pearl:
The tricuspid valve annulus is normally positioned more apically than the mitral, an important landmark in structural assessment.
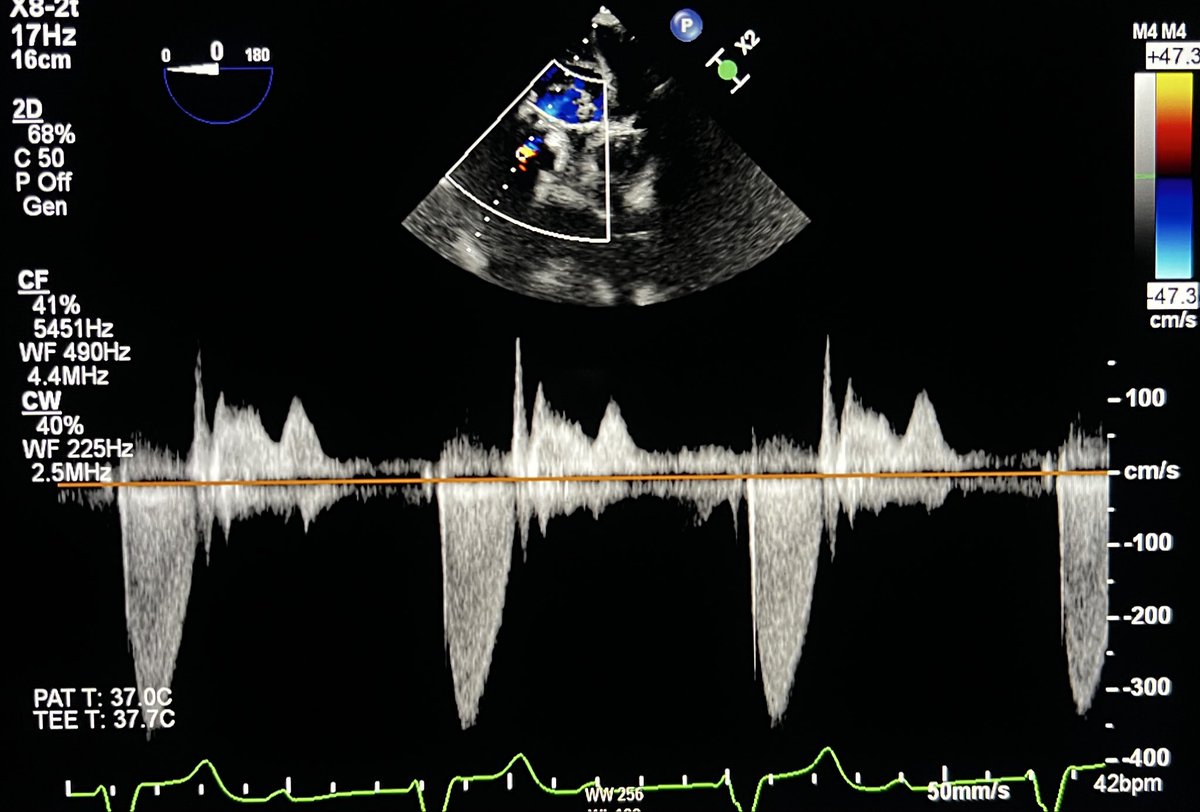
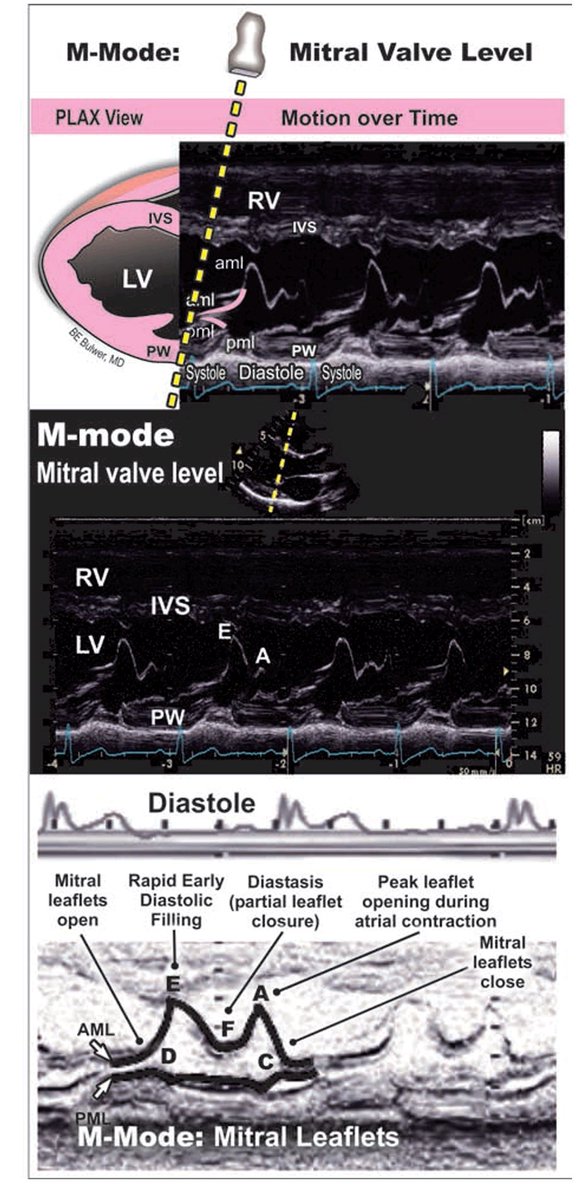
Normal M-mode echocardiography in the parasternal long-axis (PLAX) view at the mitral valve level provides a high–temporal resolution assessment of mitral leaflet motion and left ventricular filling dynamics.
The characteristic cyclical pattern of the mitral valve reflects transmitral inflow physiology across diastole. In early diastole, there is abrupt opening of the leaflets, producing the E wave, which corresponds to rapid passive LV filling driven by the pressure gradient between the left atrium and left ventricle. This is followed by diastasis, during which the pressure gradient decreases and the leaflets move toward partial closure. In late diastole, atrial contraction generates the A wave, resulting in a secondary opening of the mitral leaflets and contributing to final ventricular filling.
The E–F slope of the anterior mitral leaflet (AML) is a key parameter and reflects the rate of early diastolic closure. A steep EF slope indicates normal, brisk LV filling and good compliance, whereas a reduced or flattened slope suggests impaired filling dynamics, classically seen in conditions such as mitral stenosis. In such cases, the normal M-mode waveform becomes more "box-like," reflecting restricted leaflet mobility and reduced transmitral flow.
The posterior mitral leaflet (PML) demonstrates motion that mirrors the AML, maintaining coordinated valve dynamics. Additional structures visualized in this M-mode line include the interventricular septum (IVS) and the posterior wall of the left ventricle, which help provide anatomical context and timing relative to the cardiac cycle.
Overall, M-mode at the mitral valve level remains a simple yet powerful tool for understanding diastolic physiology, valve motion, and early pathological changes in mitral valve disease.
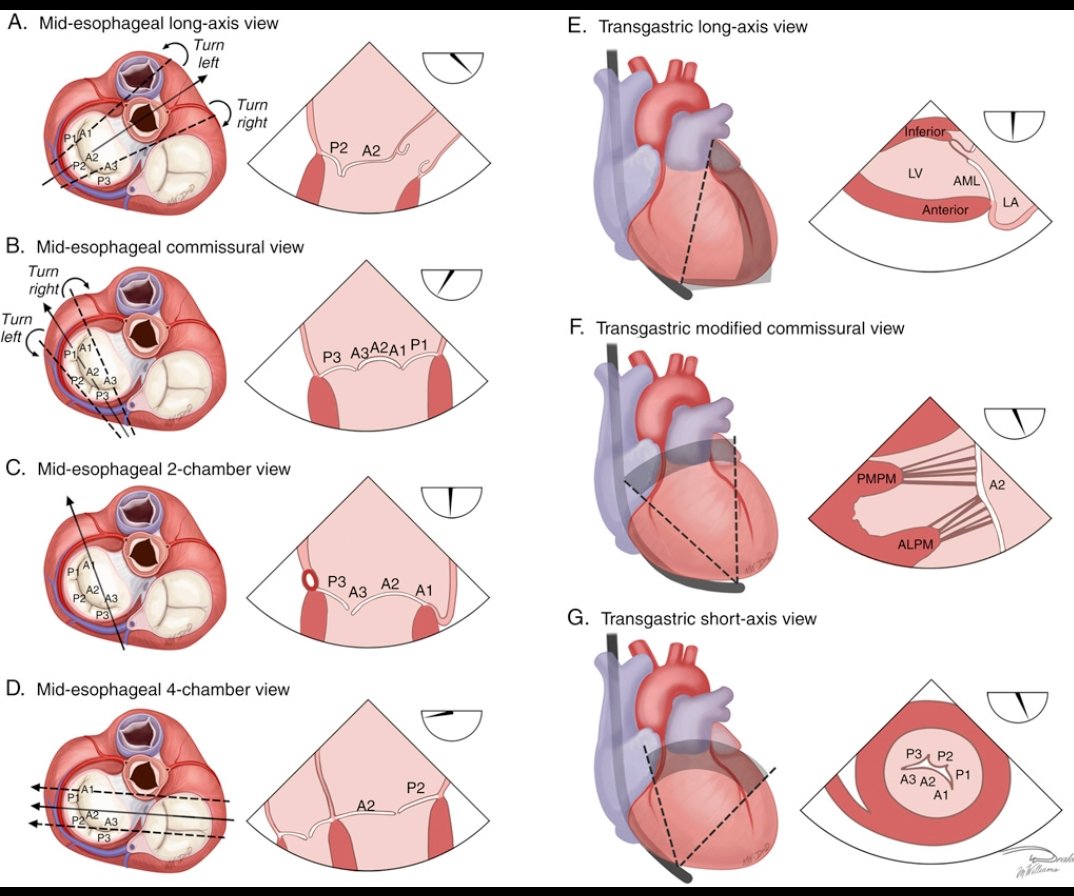
Standard 2D TEE Views for Mitral Valve Assessment
Transesophageal echocardiography (TEE) is essential for evaluating mitral valve anatomy and function. These standard views help identify leaflet segments, coaptation zones, and pathologies such as mitral regurgitation or stenosis.
Key Views & Insights:
Mid-esophageal views:
- Long-axis: Focuses on A2/P2 coaptation.
- Commissural: Visualizes A1/P1 and A3/P3 segments.
- 2-chamber: Shows the coronary sinus and LA appendage.
- 4-chamber: Offers a broader perspective of both leaflets.
Transgastric views:
- Long-axis: Similar to mid-esophageal long-axis.
- Modified commissural: Highlights papillary muscles and leaflet chords.
- Short-axis: Provides a complete en face view of all six mitral segments.
Understanding these views is crucial for diagnosing mitral valve disease and guiding interventions like mitral repair or replacement.
#Cardiology #TEE #Echocardiography
Reference: Sidebotham D, Auckland City Hospital