@tomgoom The biggest cause of repetitive stress fracturing and non union is biomechanics ie cavovarus foot /forefoot adductus. Always need to address this for long term resolution.
@BostonFootAnkle Great tips, I tend to use the para-ehl arthroscopy portal longitudinal incision and then turn blade and skirt phalanx laterally, whilst flexing IPJ slackening the fhl .
@BostonFootAnkle On the odd occasion get PF, valgus rotation or distraction, esp 100% shifts. Same way : back out screw enough to re reduce and use second screw to hold then replace 1st screw. Tbh with the flatter feet, I often dial in a bit of plantarization (not angulation).
@dr_irfan_malik Some things can’t be described in terms of severity and occasionally things get missed. More so in MSK reports, I always look at images for that reason.
@orthotraumamd I still can’t understand the need to X-ray these! My preference is dynamic uss to check gapping in PF, and any soft tissue (fat) interposition etc.
@BostonFootAnkle Thanks, that will help to reassure my patient who is pain free and eager to return to sports, 8 weeks post surgery! Only went there to get a post op check X-ray! Which shows appropriate alignment/callus / union.
@BostonFootAnkle Great technique. I’ve recently seen a report from a US DPM saying non fixation of a bunionette osteotomy would be considered malpractice in the USA!
@DrJN_SportsMed According to Bard not fully known but:
One theory: microtrauma to the tendon, which triggers the release of growth factors and other proteins that promote healing. Another is it increases blood flow to the area, which helps to deliver nutrients and oxygen to the injured tissue.
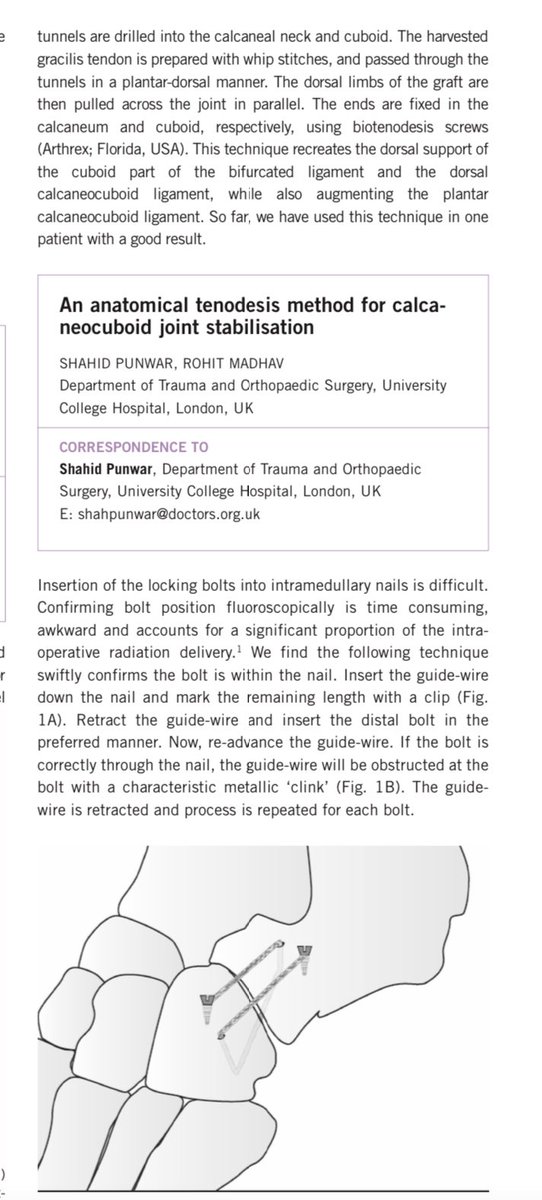
@Flawless_Physio Also occasionally CCJ can be unstable, and subluxate/dislocate. The text is a bit mixed up for some reason, but was published as a tip for stabilization. Came with hx of unstable ankle but all the time the mid-foot CCJ was dislocating!
@Flawless_Physio Great summary. With ccj and tmtj soft tissue injuries, delayed scans can be resonably normal but clinically the motion is stiff/abnormal, and the foot can’t adapt to the ground causing ongoing lateral column pains, often after “minor” kerbside sprains. Examination is the key.