I aspire to identify stocks that can be purchased now and held for a year to achieve long term capital gains. I seek to identify stocks that will at least double in value. I encourage you to consider these stocks yet do your own research before investing.
What makes you think they are hiding something? Did you see how packed with content that poster was? There is simply not space to report all of the relevant content in this format. You need a longer format like a publication in a journal. It is too early for this data.
For now, we need to seek to use content from several different sources to evaluate these early outcomes.
$FATE Reminder of EULAR Abstract Text
I went back and looked at the original EULAR abstact. In the dose 2 group, there is a participant who had a setback between months 6 and 9. This person stopped taking 2 medications at their own initiative. I suspect the person did not slowly titrate off the medication. This appears to have prompted issues.
This is a reminder that interpreting these graphs accurately requires more information.
https://t.co/jJuSe8M2Zx
$CRDF Short Version of the Legal Issue
NMS approaches Cardiff seeking to increase the royalties NMS will receive. NMS uses Cardiff's need to raise more funds by the first quarter 2027 to pressure them. They threaten to tell Cardiff’s investors and investment banks that they are going to revoke the licensing agreement.
NMS says all will be good if Cardiff adds a NMS scientist to two patents. This would function to extend royalties. It is illegal to present false information for a patent and voids the patent.
Rather than comply, Cardiff files in federal court asking for an order ending these actions by NMS and maintaining the licensing agreement. They also seek a jury trial to award damages. They do this at the point when NMS seeks to pressure them into illegal actions.
If NMS is smart, they will settle this quickly. Their actions are damaging their own royalties and making them liable for huge damages.
(Yes, this is similar to "You have nice company there - it would be a shame if something happened to it." Ok, NMS is an Italian company, but there are persons of every nationality capable of mafia-like activity.)
@Mohamed42146618@mdurgin1 I think it is better to use the sSLEDAI-2K here. I prefer to see any blood-based data on a separate chart. I think it is an improvement to report the sSLEDAI-2K. It was created for this kind of data analysis.
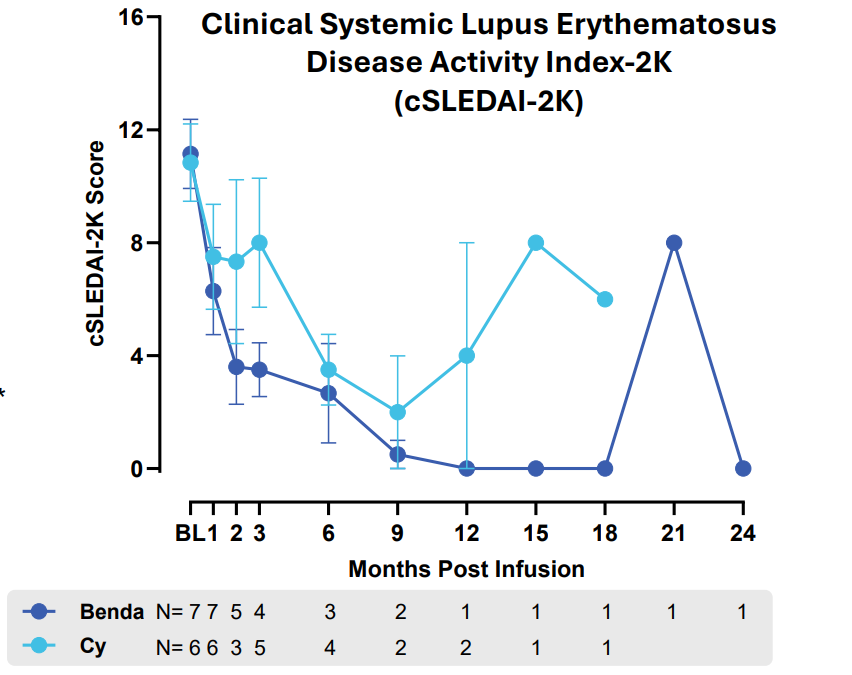
$FATE Today's SLE FT-819 SLEDAI-2K Results
Measure: The SLEDAI-2K (Systemic Lupus Erythematosus Disease Activity Index – 2000) is a 24‑item, weighted disease‑activity index for systemic lupus erythematosus that scores only active manifestations present at the visit or within the prior 30 days. It includes 8-point, 4-point, and 2-point items that total to a maximum of 105 points.
Mild disease: 1–5
Moderate disease: 6–11
High disease activity: ≥12,
Very high activity: ≥20
Interpretation: Scores in the 10 to 20 range are common. This group started with a mean baseline of 13.6. Again, we have 1 or 2 persons beyond the 9 month mark. Generally, participants appear to have moved into the mild or moderate disease levels.
It is difficult to interpret to later flair ups that are for two individuals. Could this be another short-term illness that is not related to Lupus? That seems likely with the Benda patient who returned to a score of 0 at 24 months.
I initially did not notice that this graph uses cSLEDAI-2K not the SLEDAI-2K. That is the same instrument with blood test based data omitted. This is often done in research to aid interpretation. It is typically preferred to look at the blood test data separately.
$CRDF Details about the Legal Issue.
The content below is from the legal filing by Cardiff. They appear to have a very solid case. In fact, NMS is now facing significant financial risk. Given how the stock price dropped, they could face significant damages. (Again, I am not a lawyer.)
(We will see how NMS responds. It is hard to see how they overcome what is asserted in this document.)
Content:
"Cardiff did not add Dr. Valsasina as a named inventor to the Cardiff Patents because she had no involvement in Drs. Ridinger and Erlander’s conception or reduction to practice of the claimed inventions of the Cardiff Patents. Rather, upon information and belief, Dr. Valsasina and NMS were not aware of Drs. Ridinger and Erlander’s inventions until after their innovative methods had been reduced to practice and Cardiff had filed its patent applications. A patent must accurately name the inventors of the claimed subject matter under an oath or declaration; failure to do so renders the patent invalid. NMS’s demand would have therefore required Cardiff to submit false oaths or declarations to the Patent Office that would invalidate the Cardiff Patents."
"The License Agreement does not impose an obligation on Cardiff to add an NMS employee as a named inventor to patents conceived of and reduced to practice solely by Cardiff’s employees. To the contrary, the License Agreement specifically contemplates Cardiff filing, prosecuting, and owning its own patents for its own innovations."
"NMS’s purported termination and related demands present a real and substantial risk to the cancer patients in the United States currently undergoing treatment pursuant to Cardiff’s ongoing clinical trials. NMS’s actions not only risk continuity of care for those patients undergoing clinical trials, but they jeopardize the health and safety of those patients too. The potential harm to Cardiff and these patients is immediate and urgent."
Facts Asserted:
"Drs. Erlander and Ridinger conceived of novel therapeutic methods of use for onvansertib in connection with their work for Cardiff. On September 11, 2022 and July 26, 2023, Cardiff filed provisional patent application Nos. 63/405,466 and 63/515,831, and subsequent U.S. Patent Application Nos. 18/750,971 and 18/751,014. After prosecution, the United States Patent and Trademark Office duly issued the ’813 and ’173 Patents to Cardiff on November 19, 2024 and April 1, 2025, respectively. No NMS employee contributed to the novel aspects of the inventions claimed in the Cardiff Patents."
"Dr. Valsasina did not, however, communicate with or otherwise participate in the work of Cardiff employees Drs. Erlander and Ridinger during or in temporal proximity to their inventive efforts that led to the claimed inventions of the Cardiff Patents. Tellingly, the Cardiff Patents do not claim priority to Dr. Valsasina’s work or patents; the Cardiff Patents are instead directed to and were found to be patentable by the Patent Office for separate, novel inventions that were conceived in connection with Cardiff’s work. A patent must accurately name the inventors of the claimed subject matter under an oath or declaration; failure to do so renders the patent invalid."
"On information and belief, NMS began a campaign to extract additional money or other value from Cardiff and the License Agreement in or around September 2024, including through demands that Cardiff agree to extend the royalty term of the License Agreement. NMS’s campaign later evolved to demand that an NMS employee (later identified to be Dr. Valsasina) be named as an inventor to the Cardiff Patents even though she did not jointly invent the claimed invention, to achieve a similar royalty-extending result. On information and belief, NMS’s attempts to renegotiate the License Agreement stem from NMS’s desire to negotiate more advantageous financial terms for the onvansertib drug product."
"Unless a person contributes to the conception of the invention, he is not an inventor.” MPEP § 2109 (citations omitted) (emphasis added). Even if NMS’s claims that Dr. Valsasina had suggested areas to investigate prior to the License Agreement were true “one who suggests an idea of a result to be accomplished, rather than the means of accomplishing it, is not a[] coinventor.” Id. (quoting Ex parte Smernoff, 215 USPQ 545, 547 (Bd. App. 1982).)"
Action Requested:
"Cardiff therefore requests preliminary and permanent injunctive relief from the Court ensuring that NMS continues to perform under the License Agreement and declaratory judgments that Cardiff did not breach the License Agreement, that NMS’s purported termination is ineffective, and that Drs. Ridinger and Erlander are the correct inventors on the Cardiff Patents. Cardiff further requests all other available remedies in law and equity, including damages, resulting from NMS’s conduct and breaches of the License Agreement and the implied covenant of good faith and fair dealing."
Nothing "creepy and suspicious...terrible" here. This is how real data works with human subjects. We do not expect persons to have perfect health after treatment - people still have other health issues.
All data like this demands high level thinking to interpret. One place were this is required with about every drug is evaluating side effects. You need to make judgments about how likely a health issue was due to the drug.
$IOVA Australia Approval
There are some logistical challenges of serving Australia with a travel time of about a day to Philadelphia. Yet, they will sort those out.
I am particularly interested in learning the financial details of treating patients under the Australia healthcare system.
I view this as a very encouraging development. Yet, the positive financial impact will likely not occur until 2027. In fact, there will probably be some added expenses in 2026 related to developing this market.
@n_hatami We are going to see expansion soon into other indications like NSCLC. When persons start talking about all cancers, I do not see that. Yet, I do see some improvements to TIL in the pipeline that have the potential to bring in some more major cancer categories.
@maddstone1@JessieChimni@FateThx Yes, take FT819 with low chemo to FDA as soon as possible. FT839 is expected to offer improved response with no chemo. Approval of FT839 would be about 1.5 years after FT819.
@maddstone1@JessieChimni@FateThx I would just say we do not have many participants that are 6 months post-treatment. We also have noise to contend with when physicians fill out these rating scales. When patients get a UTI or the Flu, that is going to influence these numbers.
$FATE Today's SLE FT-819 FACIT Results
Measure: Fatigue using the FACIT (Functional Assessment of Chronic Illness Therapy). This has 13 items like: “I feel fatigued.” “I need to sleep during the day,” “I have no limit to my social activity because I am tired.” It uses a scale of 0 to 4: 0 -Not at all 1 -A little bit 2- Somewhat 3- Quite a Bit 4- Very Much. When this is scored, they reverse the values so that a score of 52 represents answering 0 to all the questions.
Interpretation: Patients are beginning with baseline score which represents severe fatigue (mean 26.4). The increases in scores after treatment represent moving into the little or no fatigue level.
(Note: After the six month mark, some of these values are based on a single patient. I ponder how this data is impacted by a short-term illness like the Flu.)
$FATE Today's SLE FT-819 PGA Results
Measure: The Physician Global Assessment (PGA) for lupus is a single‑item measure where the doctor provides an overall rating of SLE disease activity. PGA SCALE: 0 – lack of activity, 0.5–1 – mild activity, 1–2 – moderate activity, 2–3 – severe illness.
This is a subjective measure, but it also provides the opportunity to capture elements of daily functioning that are not recorded with measures like lab tests.
Interpretation: Participants with Lupus are starting at a baseline level of severe illness (mean 2.18). There is significant improvement happening here. We need to exercise caution about values beyond the 9 month mark due to low subject numbers.
There is evidence of some individual patients having a shorter term flare up at a year beyond treatment. Could that be a normal illness like the Flu or Covid? Are some going to need a booster treatment?
This is such a subjective measure. What is one to make of a loss in daily function recorded by a doctor that is not reflected on a test of kidney functioning or patient reported fatigue?
$FATE Today's SLE FT-819 UPCr Results
Measure: Urine Protein-to-Creatinine Ratio (UPCR). During the filtering process, the kidneys should return most protein to the blood and place waste products in urine. When kidneys don’t work as expected, more protein than normal can leak into urine. Creatinine is a waste product that muscle cells make when they use energy. This test has some limitations. It can be impacted by exercise, dehydration, and stress.
With Lupus there is a lot of individual variability in the level of kidney impairment. We know that fibrosis (scaring) can replace healthy tissue and result in permanent damage. In severe cases, this can get so bad that persons need dialysis or even a kidney transplant.
For UPCR, the normal value is <0.2 mg/mg. The mildly increased range is about 0.2–0.5 mg/mg.
Interpretation: The decreases reported here are encouraging. It appears many who receive FT-819 treatment will see kidney functioning return to a level of mild impairment. This will likely divert many persons from the path towards more pronounced impairment.
(Note: After the six month mark, these values are based on a single patient.)