Home
Language
English
Türkçe
Bahasa Indonesia
About
Privacy Policy
Terms of Service
Pricing
Sign In
Download All
Share
Rameses10
@AstroRMin10
Strictly Introvert I ISTP | NSFW opinion | บ่นชีวิตบ้าง ก่นด่าเผด็จการบ้าง 18+บ้าง มีวิชาการบ้าง | lock : @AstroRMinX
Bangkok, Thailand
Joined August 2016
743
Following
8.6K
Followers
12.9K
Posts
Pinned Tweet
Rameses10
@AstroRMin10
almost 3 years ago
กติกา การเข้า acc lock https://t.co/JJB4KPnPsh - กด follow acc นี้ และ acc lock แค่นั้น พอ ง่ายมะ 😆
Rameses10
@AstroRMin10
15 days ago
@Jkitikitty
อกแน่นมากกก
Rameses10
@AstroRMin10
16 days ago
·
Phasi Charoen
@nerdglassisbest
แล้วแต่ รพ.ครับ ของผม ตอนนั้น ขนาดสิทธิ ขรก เฝจอง กพ ได้ทำ ตค 😅
Rameses10
@AstroRMin10
17 days ago
·
Nong Khang Phlu
BP ลงแบบ dramatic มาก คุมได้ด้วยยา dose ต่ำ เพียงแค่ control osa ได้ แถม ทำงานสบาย ไม่ง่วงเจียนตายด้วย ปัญหาคือ sleep lab รพ.รัฐ คิว 2ชาติครึ่ง ส่วนเอกชน แทบจะนัดตามใจอยาก แต่ก็ (แบบมี โปร) ก็ หลัก หมื่น แต่ก็ 1หมื่น ติ๋มๆนั คุ้มกว่า ค่า pci หรือ ค่าเตียงผู้พิการแน่ๆ
无羁😎
@heijix86
18 days ago
ภาวะหยุดหายใจขณะนอนหลับ มาคลินิคนิวโรด้วยอาการขี้ลืมสมาธิสั้น บางครั้งก็มาด้วยวูบเป็นลมหาเหตุไม่เจอ บางครั้งเกิดอุบัติเหตุบนท้องถนน ทำให้ความดันโลหิตสูงคุมยาก เป็นปัจจัยเสี่ยงโรคหัวใจห้องบนเต้นผิดจังหวะได้ เป็นโรคที่ยังวินิจฉัยกันน้อย เพราะไม่ได้ไปตรวจ หมอๆก็อาจจะเป็นเช่นกัน 😅
See More
Who to follow
Z SPA
@Zspawellness
สนใจจองคิวแอดไลน์ @ zspa หรือ https://t.co/GS5h1olTw3
The Woods
@thewoodsbkk
เดอะวูดส์ สปาชายย่านนนทบุรี เปิดบริการ 12.00-21.00 จองนวดแอดไลน์ https://t.co/23koVRXnxM The woods 男人按摩店在暖武里府中心 營業時間 12.00 -21.00 點 預定按摩 DM
tcsspa
@tcsspa
TCS Spa at Charoenkrung & Ari 🟢 Line : @tcsspa 📞0804142944
Rameses10
@AstroRMin10
17 days ago
·
Phasi Charoen
ตัวช่วยลดภาระการกินยา ht ของแท้เลย เป็นปัจจัยแฝงเงียบ ที่ถ้ารัฐลงทุนดีๆ เพิ่ม accessibility การทำ sleep lab และ เครื่อง *pap นอกจากอนุรักษ์วัยแรงงานได้แล้ว ยังลดงบยา HT และ งบยา MI และ Arrhythmia ได้อีกเยอะเลย แต่อย่างว่า รัฐบางรัฐ เขาเน้นปลายเหตุ เน้นเฉพาะหน้า แค่ปาหี่โชว์ไปวันๆ คงไม่คิดทำอะไรเพิ่มหรอก
See More
Rameses10
@AstroRMin10
17 days ago
日本語を勉強しましょう!👊🔥
#日本語
#タイゴ
#タイ語
Rameses10
@AstroRMin10
25 days ago
@heijix86
ไม่ได้ใช้เป็นแม้แต่ 3rd line มานานแล้ว ขนาดclinic รากหญ้า ก็แทบไม่มีให้เห็นเท่าไหร่ ตั้งแต่ losartan หลุด patent
Rameses10
@AstroRMin10
26 days ago
@9Suphanat
ส้นตีนมาก ดวงน่าจะจบลงที่ลูกปืนนะ
Rameses10
@AstroRMin10
about 1 month ago
@Gazpaka
พยายามอยู่ครับ เหมือนจะไม่ใช่ทาง เลยว่า เห็นด้วยมสกๆ คนที่รุกก็ได้รับก็ได้ บุญหนามากจริงๆ
Rameses10
@AstroRMin10
about 1 month ago
@heijix86
@gusstation
ตอนเด็กกว่านี้ ยังมีปัญญาจอง jugendherberge ที่ grindelwald ตอนนั้ รร. Only จ้า วิวสวย หมอกลง ก็สวย
Rameses10
@AstroRMin10
about 2 months ago
@heijix86
ขนมปัง choc chip ใน coop คือ the best 😋
Rameses10
@AstroRMin10
about 2 months ago
@Peony_sweetie
ไม่ และบางครั้ง กับลูกค้า ก็ไม่พูดแทนตัวว่าหมอด้วย ถ้าน่ารำคาญ หรือกำลังเคือง จะใช้ ผม ด้วยซ้ำ
Rameses10
@AstroRMin10
about 2 months ago
@heijix86
ฟาดเคราะห์ครับ🫂
Rameses10
@AstroRMin10
about 2 months ago
@heijix86
ขี้อายพอๆกับ fujisan ขึ้นไป gornergrat แล้วยัง
Rameses10
@AstroRMin10
about 2 months ago
@Jkitikitty
เคยถาม อ.สูติ "...พวก case OPD / pv โง่ๆ อาจมี request หมอหญิงบ้าง แต่เวลาหน้าสิ่วหน้าขวาน เวลาจะคลอด ไม่เคยมีใครสน หรือระบุเพศหมอ"
Rameses10
@AstroRMin10
about 2 months ago
Rameses10
@AstroRMin10
about 2 months ago
Bookmark ไว้แล้วทุกคอม (update ASCVD online calculator) https://t.co/wjkXm4gLTt
#PREVENT
#ASCVD
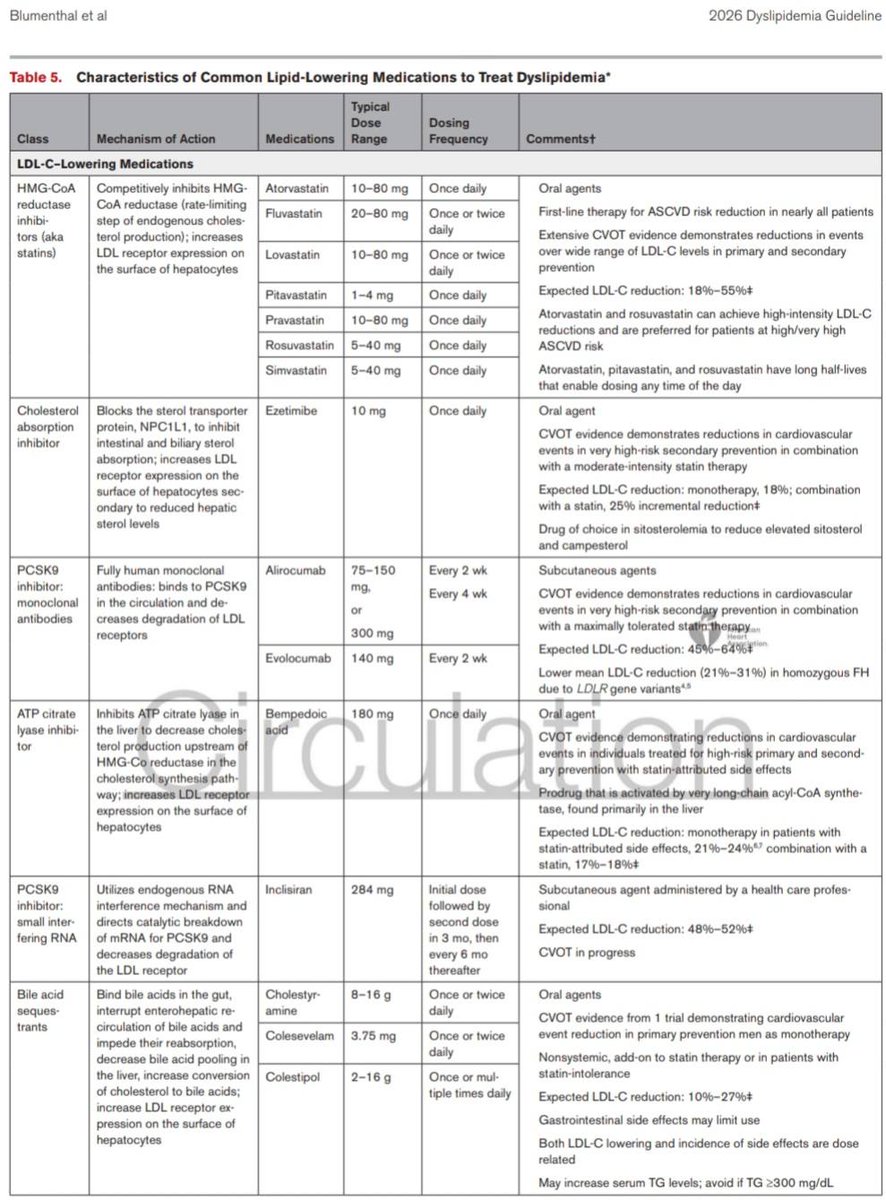
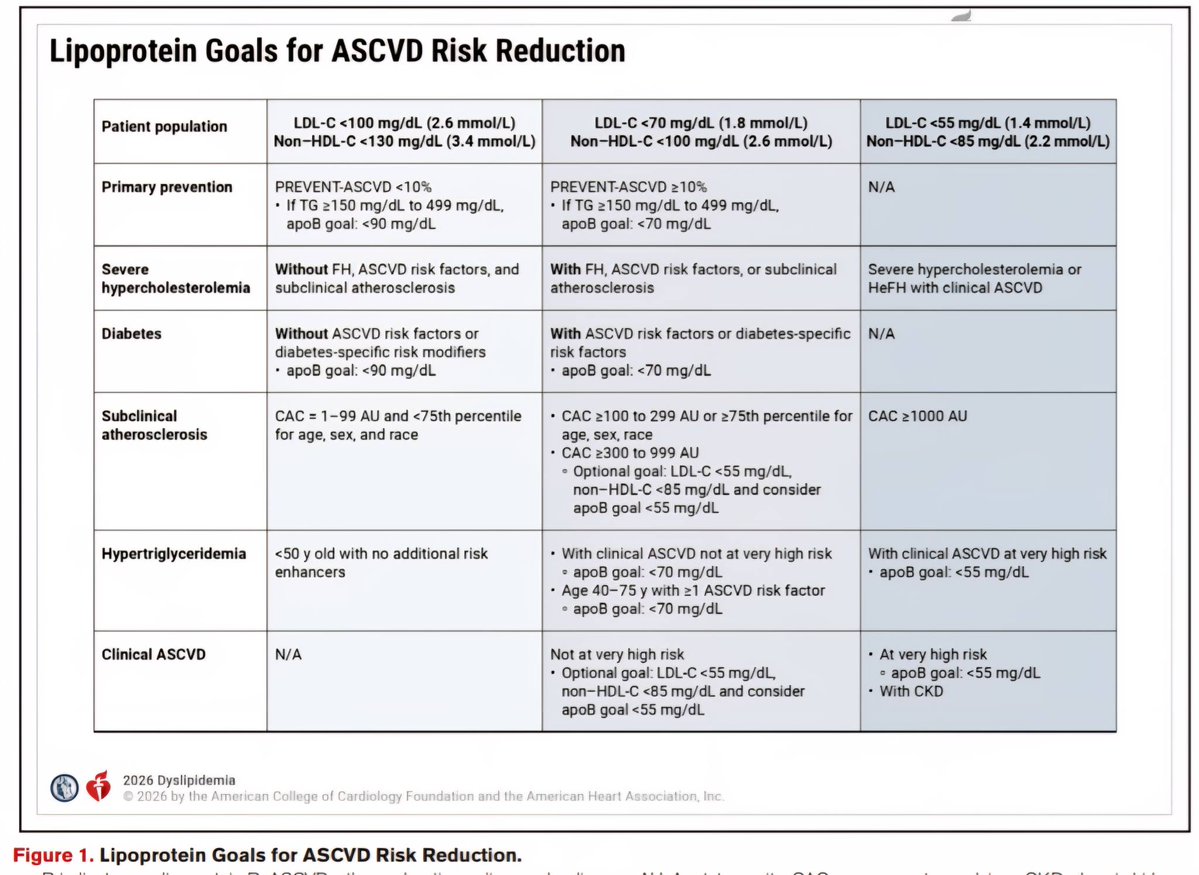
ไม่ได้เชียร์ Statin เบอร์นั้น แต่ถ้าต้องให้ ก็จงให้ ---- Credit : คลินิกแพทย์ครรชิต-แพทย์สุวิโชติ เชี่ยวชาญ https://t.co/rm8RqVA8Od แนวทางรักษาไขมันสูง ใหม่ล่าสุด 2026 !! จาก New 2026 ACC/AHA guideline Dyslipid ออกมาเมื่อ 13 มี.ค.2026 📷 สรุปวิธีรักษาไขมันสูง ในคนไข้ 8 กลุ่ม 📷 อายุ 30-79 + LDL 70-189 without ASCVD 📷 Calcium score (CAC score) • ควรตรวจในคนไข้รายไหน ? • ตรวจและแปลผลอย่างไร ? • นำมาพิจารณาให้ Statin อย่างไร ? 📷 Severe hypercholesterolemia : LDL ≥190 📷 DM without established ASCVD 📷 Secondary ASCVD Prevention 📷 CKD stage 3 or higher 📷 คนไข้ HIV 📷 คนไข้มะเร็ง 📷 ยาลดไขมัน ชนิด, Dose, รายละเอียดของยาแต่ละตัว 📷 Lp(a) คืออะไร ?, มีอันตรายอย่างไร ? เจาะแล้วมีประโยชน์อย่างไร ? ควรเจาะในคนไข้รายไหน ? ต้องงดอาหารก่อนเจาะหรือไม่ ? วิธีลด Lp(a) มีอะไรบ้าง ? เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ? 📷 ApoB คืออะไร ? มีความสำคัญอย่างไร ? ควรเจาะในคนไข้รายไหน ? __________________________________________ 📷 อายุ 30-79 + LDL 70-189 without ASCVD __________________________________________ 📷 ประเมิน ASCVD risk ก่อนนะครับ !! โดยใช้ "PREVENT-ASCVD equations" !! 📷 Low 10-y risk (<3%) 📷 LDL 160-189 or 30-y ASCVD risk ≥10% (สำหรับคนอายุ 30–59 y) 📷 moderate-intensity statin (class 2a) (goal = LDL <100 + ลดลง ≥30% + non-HDL C <130) 📷 LDL <160 and 30-y ASCVD risk <10% 📷 health behavior counseling (class 1) 📷 Borderline 10-y risk (3% to <5%) 📷 moderate-intensity statin (class 2a) (goal = LDL <100 + ลดลง ≥30% + non-HDL C <130) 📷 ควรประเมิน Risk enhancer (ดูจากตารางด้านล่าง) ประกอบการพิจารณาให้ statin ด้วย (class 2a) 📷 if high-sensitivity C-reactive protein (hsCRP) ≥2 mg/L on 2 successive occasions โดยไม่มีสาเหตุ --> ให้ high-intensity statin (class 2a) 📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin ให้ประเมิน CAC testing (coronary artery calcium) โดยใช้ non-contrast-gated cardiac CT (class 1) (โดยทั่วไปแนะนำให้ทำในชายอายุ ≥40 และ หญิงอายุ ≥45) 📷 if CAC >0 --> ให้ statin (class 1) 📷 if CAC =0 --> health behavior counseling + repeat CAC 3-7 y (class 1) 📷 Intermediate 10-y risk (5% to <10%) 📷 moderate-high intensity statin (class 1) (goal = LDL <100 + ลดลง ≥30% to ≥50% + non-HDL C <130) (class 2a) (ถ้าคนไข้อยู่ใน higher end of this risk range แนะนำให้ใช้ high intensity statin เพื่อลด LDL ≥50%) 📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin ให้ประเมิน CAC testing (class 1) 📷 พิจารณาให้ statin จาก CAC ในเกณฑ์เดียวกับกรณี borderline 10-y risk ข้างต้น 📷 High 10-y risk (≥10%) 📷 high intensity statin (class 1) (goal = LDL <70 + ลดลง ≥50% + non-HDL C <100) (class 2a) 📷 if not achieved LDL & non-HDL C goal 📷 add ezetimibe (class 2a) 📷 add PCSK9 mAb or Bempedoic acid (with or without ezetimibe) (class 2b) 📷 Special consideration 📷 if life expectancy <1 y 📷 อาจพิจารณาหยุดยาลดไขมัน (class 2b) 📷 คนไข้ที่มี baseline untreated LDL <70 และ non–HDL-C <100 without additional ASCVD risk factors 📷 ไม่ต้องให้ยา statin (class 3 ; No benefit) __________________________________________ 📷 Calcium score (CAC score) (Coronary artery calcium score) นำมาพิจารณาให้ Statin อย่างไร ? __________________________________________ 📷 Calcium score (CAC score) ควรตรวจในคนไข้รายไหน ? 📷 Men ≥40 or Women ≥45 Years ที่ประเมินความเสี่ยงโดยใช้ PREVENT-ASCVD equations แล้วตกอยู่ในกลุ่ม Intermediate 10-y risk (5% to <10%) หรือ Borderline 10-y risk (3% to <5%) และยังตัดสินใจไม่ได้แน่ชัดว่าควรให้ยา statin หรือไม่ 📷 CAC score ตรวจและแปลผลอย่างไร ? 📷 ตรวจโดยใช้ non-contrast-gated cardiac CT 📷 แปลผล 📷 CAC score แสดงถึง overall amount of calcified coronary plaque ซึ่งบ่งบอกถึงการมี subclinical atherosclerosis โดยที่ CAC score ยิ่งสูง ก็จะพยากรณ์ได้ว่าคนไข้ยิ่งมีโอกาสสูงที่จะเกิด MACE (major adverse CV event) ในอนาคต และความสัมพันธ์ระหว่าง CAC score กับการเกิด MACE นี้พบว่าเป็นไปในแบบที่แทบจะเป็น linear relationship เลยทีเดียวครับ 📷 CAC score แบ่งระดับความรุนแรงได้ดังนี้ 📷 absent (0 AU) 📷 minimal (1-9 AU) 📷 mild (10-99 AU) 📷 moderate (100-299 AU) 📷 severe (300-999 AU) 📷 extensive (≥1000 AU) 📷 CAC score นำมาพิจารณาให้ Statin อย่างไร ? 📷 CAC score 1-99 AU and <75th standardized percentile for age, sex & race 📷 moderate intensity statin (class 2a) 📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a) 📷 CAC score 100-299 AU or ≥75th standardized percentile for age, sex & race 📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx) (class 1) 📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) 📷 CAC score 300-999 AU (severe) 📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx) (class 1) 📷 Goal 📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70 📷 optional : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55 (โดยใช้วิธีเพิ่ม intensity of statin หรือ add ezetimibe, PCSK9 mAb, or bempedoic acid) (class 2a) 📷 CAC score ≥1000 AU (extensive) 📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx) (class 1) 📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55 📷 incidental finding of mild CAC on noncardiac CT scan 📷 moderate intensity statin (class 2a) 📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a) 📷 moderate-to-severe incidental coronary atherosclerosis identified on noncardiac CT scans (eg, by visual estimation or a validated artificial intelligence-based algorithm) 📷 moderate-high intensity statin (class 2a) 📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a) 📷 คนไข้ที่มี LDL ต่ำกว่า targets สำหรับแต่ละ CAC levels อยู่แล้วโดยที่ไม่ได้ on statin 📷 ก็ยังแนะนำให้ใช้ยาเพื่อลด LDL ลง ≥30% ด้วยนะครับ 📷 CCTA (coronary CT angiography) พิจารณาทำในรายไหน ? 📷 อาจพิจารณาทำ CCTA (coronary CT angiography) ในคนไข้ที่ไม่เคยมี ASCVD แต่ likely ที่จะมี high burden of "noncalcified" plaque (eg, inflammatory disorders, HIV, and diabetes) เพื่อช่วยตัดสินใจในการให้ statin (class 2b) __________________________________________ 📷 Severe hypercholesterolemia : LDL ≥190 __________________________________________ 📷 without clinical ASCVD, additional ASCVD risk factors, HeFH, or subclinical atherosclerosis 📷 maximally tolerated statin (class 1) (goal = LDL <100 + non-HDL C <130) 📷 if not achieved LDL & non-HDL C goal 📷 add ezetimibe, PCSK9 mAb and/or bempedoic acid (class 1) 📷 add inclisiran (as alternative to PCSK9 mAb) with or without ezetimibe (class 2a) (ณ ชั่วโมงนี้ inclisiran ยังถือเป็น second-line PCSK9i โดยยังได้ข้อบ่งชี้เพียงแค่ใช้ลด LDL เท่านั้น เนื่องจากยังต้องรอดู CV benefit จาก CV outcome trials อยู่ครับ) 📷 without clinical ASCVD but with HeFH, additional ASCVD risk factors, or subclinical atherosclerosis (documented coronary calcification) 📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <70 + non-HDL C <100 📷 with clinical ASCVD 📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <55 + non-HDL C <85 + optional apoB goal <55 __________________________________________ 📷 DM without established ASCVD __________________________________________ 📷 อายุ 20-39 📷 moderate-intensity statin ใน 2 กรณี 📷อายุ ≥30 + PREVENT ASCVD 10-y risk ≥3% หรือ 30-y risk ≥10% (class 2a) 📷 มี Diabetes-specific risk enhancer (DM of long duration [≥10 y of T2DM, ≥20 y of T1DM], albuminuria (≥30 μg of albumin/ mg cr), eGFR <60, retinopathy, neuropathy, or ABI <0.9) (class 2b) 📷 อายุ 40-75 📷 moderate-intensity statin (class 1) 📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 1) + optional apoB goal <90 📷 high intensity statin (class 2a) if PREVENT ASCVD 10-y risk ≥10% or multiple ASCVD risk factors 📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a) + optional apoB goal <70 📷 add ezetimibe or PCSK9 mAb (class 2b) if not achieved LDL & non-HDL C goal 📷 add IPE (after a statin) (class 2b) if additional ASCVD risk factor(s) + LDL<100 + fasting TG 150–499 หมายเหตุ Additional ASCVD risk factor(s) ในกรณีนี้ ดูจาก REDUCE-IT inclusion criteria ได้แก่ men ≥55 y, women ≥65 y, cigarette smoking or stopped smoking within 3 mo, HT (SBP ≥140 or DBP ≥90 or ใช้ยา HT อยู่), HDL ≤40 for men or ≤50 for women, hs-CRP >3.0 mg/L, CrCl >30 and <60, retinopathy, albuminuria (≥30 μg of albumin/mg Cr), ABI <0.9 📷 อายุ >75 + estimated life expectancy≥2.5y 📷 moderate-intensity statin (class 2b) 📷 ถ้ามี statin-attributed side effects 📷 initiation of ezetimibe and/or bempedoic acid or a PCSK9 mAb (class 1) __________________________________________ 📷 Secondary ASCVD Prevention __________________________________________ 📷 Clinical ASCVD "Not at Very High Risk" (ดู criteria สำหรับ Very High Risk จากรูปด้านล่างนะครับ) 📷 goal 📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70 📷 optional goal : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55 📷 ยา 📷 high intensity statin (class 1) 📷 if not achieved LDL & non-HDL C goal 📷 add ezetimibe, PCSK9 mAb and/or bempedoic acid (class 2a) 📷 inclisiran (with or without ezetimibe) ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a) 📷 Clinical ASCVD "at Very High Risk" (include ASCVD with CKD) 📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55 📷 ยา 📷 high intensity statin (class 1) 📷 if not achieved LDL & non-HDL C goal 📷 add ezetimibe and/or PCSK9 mAb (class 1) 📷 add bempedoic acid, with or without ezetimibe and/or PCSK9 mAb (class 2a) 📷 inclisiran (with or without ezetimibe) ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a) 📷 HFrEF Due to ASCVD (IHD) + มี reasonable life expectancy (3–5 y) + not already on a statin 📷 อาจพิจารณาเริ่มให้ moderate-intensity statin เพื่อลด ASCVD events (class 2b) 📷 HFrEF ที่ไม่มี ASCVD + ไม่มีข้อบ่งชี้อื่นของ statin --> ไม่แนะนำให้ statin (class 3 ; No benefit) __________________________________________ 📷 CKD stage 3 or higher __________________________________________ 📷 CKD stage 3 or higher + อายุ 40-75 + LDL 70-189 📷 แนะนำให้ moderate-intensity statin or moderate-intensity statin + ezetimibe เพื่อลด ASCVD risk (class 1) 📷 CKD stage 3 or higher + clinical ASCVD 📷 แนะนำให้ high-intensity statin with or without ezetimibe and/or a PCSK9 mAb (goal : LDL <55 + ลดลง ≥50% + non-HDL C <85) (class 1) 📷 CKD ที่ require maintenance hemodialysis 📷 อาจพิจารณา continue statin เพื่อลด risk of ASCVD events โดยพิจารณาจากหลายๆปัจจัย เช่น expected survival, other comorbidities, and severity of ASCVD (class 2b) __________________________________________ 📷 คนไข้ HIV __________________________________________ 📷 คนไข้ HIV อายุ 40-75 📷 แนะนำให้ statin เพื่อลด risk of a first ASCVD event และลด rate of coronary atherosclerosis progression (class 1) __________________________________________ 📷 คนไข้ cancer __________________________________________ 📷 if life expectancy ≥ 2 y ให้พิจารณาใช้ statin ได้ตามข้อบ่งชี้เหมือนคนไข้ที่ไม่ได้เป็นมะเร็ง 📷 อาจพิจารณาเริ่มให้ statin เพื่อ prevent anthracycline-induced cardiotoxicity (class 2b) __________________________________________ 📷 ยาลดไขมัน ชนิด, Dose, รายละเอียดของยาแต่ละตัว ดูจากตารางด้านล่าง __________________________________________ __________________________________________ 📷 Lp(a) __________________________________________ 📷 Lp(a) คืออะไร ? 📷 คือ LDL-like particle ที่มี structure แตกต่างไปจาก LDL โดยจะ carries a single apoprotein(a) strand bound to its apoB-100 component 📷 Lp(a) มีอันตรายอย่างไร ? 📷 Lp(a) เป็น genetic risk factor ในการเกิด ASCVD ครับ (independent of LDL and other risk factors) 📷 ระดับของ Lp(a) ที่สูงจะสัมพันธ์กับการเกิด ASCVD อย่างชัดเจน โดยผ่านกลไกหลายๆอย่าง เช่น proatherogenic and proinflammatory effects ซึ่งส่วนหนึ่งก็ถูกกระตุ้นจาก oxidized phospholipids on Lp(a) นั่นเอง 📷 เจาะแล้วมีประโยชน์อย่างไร ? 📷 เจาะเพื่อ identify คนไข้ที่ increased ASCVD risk (independent of LDL and other risk factors) 📷 ควรเจาะในคนไข้รายไหน ? 📷 in all adults !! ควรเจาะอย่างน้อย 1 ครั้งในชีวิตครับ (class 1) (ระดับของ Lp(a) จะไม่ค่อยเปลี่ยนแปลงตามกาลเวลา และไม่ค่อยเปลี่ยนแปลงตาม lifestyle factors ด้วยครับ เนื่องจากเป็นปัจจัยทาง genetic ยกเว้น ช่วง menopause transition อาจจะมีค่าเปลี่ยนแปลงได้บ้าง หรือมี secondary cause of elevated Lp(a) เช่น kidney, liver, thyroid disease, pregnancy, certain medications) 📷 เจาะใน first-degree family members ของคนไข้ที่เป็น FH, premature ASCVD, or high Lp(a) (class 1) 📷 ต้องงดอาหารก่อนเจาะหรือไม่ ? 📷 ไม่ต้อง fasting เลยครับ !! 📷 วิธีลด Lp(a) มีอะไรบ้าง ? 📷 PCSK9i (mAbs and small-interfering RNA) --> ลด Lp(a) ได้ ∼15-30% (ณ ชั่วโมงนี้ PCSK9i ยังไม่ได้รับ FDA-approved for Lp(a) lowering นะครับ แต่ก็เริ่มมีข้อมูลสนับสนุนมากขึ้นเรื่อยๆในแง่ของ clinical outcome) 📷 Specific Lp(a)-lowering therapies (ลด Lp(a) production ได้แก่ mRNA therapies or oral small-molecule inhibitors) --> กำลังมีการศึกษาใน randomized clinical outcomes trials อดใจรออีกซักหน่อยนะครับ !! 📷 lipoprotein-apheresis 📷 Lifestyle management -->ไม่ค่อยมีผลต่อระดับ Lp(a) ครับ เพราะเป็นปัจจัยทาง genetic 📷 statin --> ไม่มีผลลดระดับ Lp(a) และอาจเพิ่มระดับ Lp(a) เล็กน้อยด้วยซ้ำ โดยเฉลี่ยแล้วจะเพิ่ม ~1.1 mg/dL แต่ก็ถือว่าไม่จำเป็นต้องหยุดใช้ statin นะครับ เนื่องจากมี strong benefit ในการ prevent ASCVD 📷 เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ? (Lp(a) ≥50 mg/dL จึงจะถือว่าสูงนะครับ โดยพบได้ ~20% ของประชากร) 📷 คนไข้ที่ยังไม่มี ASCVD 📷 แนะนำให้รีบ optimal early control of modifiable CV risk factors โดยการคุม BP, BS, lipid ให้ดีที่สุด รวมถึงการพิจารณาเริ่มให้หรือ intensified statin เพื่อลด LDL และลด ASCVD risk (class 1) 📷 คนไข้ที่มี clinical ASCVD + elevated Lp(a) + ได้ maximally tolerated statin แล้วยังไม่ achieved LDL and non–HDL goals 📷 ให้ add PCSK9 mAb (class 1) เพื่อให้ achieved LDL, non–HDL, ApoB goal + potential additional benefit of moderate Lp(a) lowering 📷 คนไข้ที่ Lp(a) ≥60 mg/dL + FH + (CAD or PAD) 📷 ให้ทำ lipoprotein-apheresis (FDA-approved based on observational data) __________________________________________ 📷 ApoB __________________________________________ 📷 ApoB คืออะไร ? 📷 ApoB เป็นการวัด atherogenic particle number โดยตรง ซึ่งจะมีจำนวน 1 molecule per LDL, VLDL and Lp(a) particle ซึ่งแตกต่างจากตัวเลข LDL ที่จะ reflects ถึง cholesterol mass ที่อยู่ภายใน LDL particles มากกว่าที่จะ reflects ถึง number of atherogenic lipoproteins (แต่ LDL ยังคงเป็น traditional lipid marker for ASCVD risk assessment and treatment targets อยู่นะครับ) 📷 ApoB มีความสำคัญอย่างไร ? 📷 ApoB สามารถ predicts ASCVD risk ได้ accurate กว่า LDL ใน setting คนไข้ที่มี discordance กันระหว่างตัวเลข LDL และ ApoB เช่น LDL อยู่ใน target ดีแล้ว แต่ ApoB ยังสูงเกิน goal ซึ่งจะถือว่าคนไข้จะยังมี persistent atherogenic particle burden (ยังมี residual CVD risk in statin-treated populations) ที่จำเป็นต้องปรับยาเพิ่มต่อครับ โดย pattern แบบนี้มักพบในกลุ่มคนไข้ cardiometabolic disease, including ASCVD, CKM syndrome, diabetes, and/or TG ≥150 mg/dL ซึ่งในกรณีแบบนี้เราจะถือว่า ApoB เป็น more reliable marker for ASCVD risk and therapeutic guidance ครับ 📷 ApoB ยังสัมพันธ์กับการเกิด CV events independent of LDL ด้วยครับ 📷 ตัวเลข ApoB จึงสามารถใช้เป็นได้ทั้ง target ในการใช้ยารักษา และใช้เป็นตัวบอก ASCVD risk ได้ด้วย 📷 ควรเจาะในคนไข้รายไหน ? 📷 คนไข้ที่ใช้ยาลดไขมันอยู่แล้ว โดยเฉพาะคนไข้ที่เป็น ASCVD, CKM syndrome, type 2 diabetes, and/or elevated TG ที่ achieved LDL and/or non–HDL-C goals แล้ว ควรเจาะ ApoB ดูเพื่อช่วยตัดสินใจว่าจะต้องปรับยาเพิ่มต่ออีกหรือไม่ (class 2a) 📷 คนไข้ที่ยังไม่ได้ใช้ยาลดไขมัน อาจพิจารณาเจาะ ApoB เพื่อช่วย enhance ASCVD risk assessment และช่วยตัดสินใจในการเริ่มให้ยา และช่วย characterize inherited lipid disorders (class 2b) __________________________________________ Reference 📷 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/ AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines 13 มี.ค.2026 #dyslipidemia #accahaguideline #ไขมันในเลือดสูง
See More
Rameses10
@AstroRMin10
about 2 months ago
Last Seen Users on Sotwe
Anh Thợ Móc
Seen from
Vietnam
_Hùngˇ☻
Seen from
Vietnam
kenjiro hosaka
Seen from
Japan
Haty Evli çiftiz
Seen from
Turkey
marc
Seen from
Netherlands
Soos_Time (nsfw art)
Seen from
United Kingdom
صديق مصرى
💲
Seen from
United States
سونييـي
Seen from
Turkey
salope75018
Seen from
Algeria
Trends for you
1
Karmelo
Under 10K tweets
2
Belfast
Under 10K tweets
3
$XDC
Under 10K tweets
4
Nintendo
Under 10K tweets
5
#loveislandusa
Under 10K tweets
6
Ireland
Under 10K tweets
7
Good Wednesday
Under 10K tweets
8
Fable 5
Under 10K tweets
9
California
Under 10K tweets
10
Knicks
Under 10K tweets
Most Popular Users
1
Elon Musk
@elonmusk
240.2M followers
2
Barack Obama
@barackobama
119.3M followers
3
Donald J. Trump
@realdonaldtrump
111.6M followers
4
Cristiano Ronaldo
@cristiano
109.2M followers
5
Narendra Modi
@narendramodi
106.9M followers
6
Rihanna
@rihanna
97.3M followers
7
NASA
@nasa
92.1M followers
8
Justin Bieber
@justinbieber
90.6M followers
9
KATY PERRY
@katyperry
86.9M followers
10
Taylor Swift
@taylorswift13
80.8M followers
11
Lady Gaga
@ladygaga
72.3M followers
12
Kim Kardashian
@kimkardashian
69.4M followers
13
Virat Kohli
@imvkohli
68.7M followers
14
YouTube
@youtube
68.6M followers
15
Bill Gates
@billgates
63.5M followers
16
The Ellen Show
@theellenshow
62.5M followers
17
CNN
@cnn
61.9M followers
18
Neymar Jr
@neymarjr
61.3M followers
19
X
@x
60.9M followers
20
Selena Gomez
@selenagomez
60M followers
Olivia
Online
✨
⭐
💫





![AstroRMin10's tweet photo. Bookmark ไว้แล้วทุกคอม (update ASCVD online calculator)
https://t.co/wjkXm4gLTt
#PREVENT #ASCVD
ไม่ได้เชียร์ Statin เบอร์นั้น แต่ถ้าต้องให้ ก็จงให้
----
Credit : คลินิกแพทย์ครรชิต-แพทย์สุวิโชติ เชี่ยวชาญ
https://t.co/rm8RqVA8Od
แนวทางรักษาไขมันสูง ใหม่ล่าสุด 2026 !!
จาก New 2026 ACC/AHA guideline Dyslipid ออกมาเมื่อ 13 มี.ค.2026
📷 สรุปวิธีรักษาไขมันสูง ในคนไข้ 8 กลุ่ม
📷 อายุ 30-79 + LDL 70-189 without ASCVD
📷 Calcium score (CAC score)
• ควรตรวจในคนไข้รายไหน ?
• ตรวจและแปลผลอย่างไร ?
• นำมาพิจารณาให้ Statin อย่างไร ?
📷 Severe hypercholesterolemia : LDL ≥190
📷 DM without established ASCVD
📷 Secondary ASCVD Prevention
📷 CKD stage 3 or higher
📷 คนไข้ HIV
📷 คนไข้มะเร็ง
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
📷 Lp(a)
คืออะไร ?, มีอันตรายอย่างไร ?
เจาะแล้วมีประโยชน์อย่างไร ?
ควรเจาะในคนไข้รายไหน ?
ต้องงดอาหารก่อนเจาะหรือไม่ ?
วิธีลด Lp(a) มีอะไรบ้าง ?
เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
📷 ApoB
คืออะไร ?
มีความสำคัญอย่างไร ?
ควรเจาะในคนไข้รายไหน ?
__________________________________________
📷 อายุ 30-79 + LDL 70-189 without ASCVD
__________________________________________
📷 ประเมิน ASCVD risk ก่อนนะครับ !!
โดยใช้ "PREVENT-ASCVD equations" !!
📷 Low 10-y risk (<3%)
📷 LDL 160-189 or 30-y ASCVD risk ≥10% (สำหรับคนอายุ 30–59 y)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 LDL <160 and 30-y ASCVD risk <10%
📷 health behavior counseling (class 1)
📷 Borderline 10-y risk (3% to <5%)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
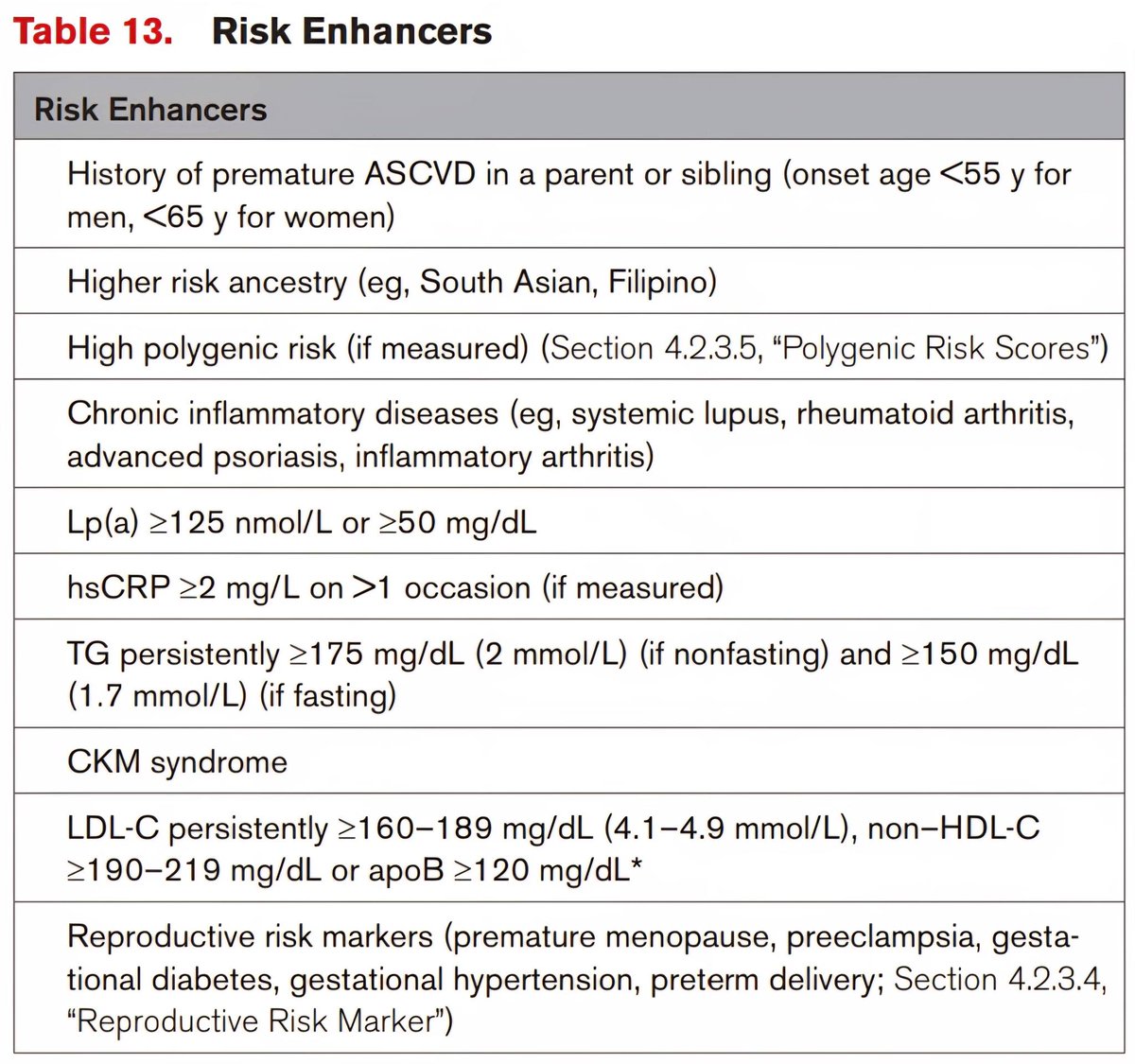
📷 ควรประเมิน Risk enhancer (ดูจากตารางด้านล่าง) ประกอบการพิจารณาให้ statin ด้วย
(class 2a)
📷 if high-sensitivity C-reactive protein (hsCRP) ≥2 mg/L on 2 successive occasions โดยไม่มีสาเหตุ
--> ให้ high-intensity statin (class 2a)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (coronary artery calcium) โดยใช้ non-contrast-gated cardiac CT (class 1) (โดยทั่วไปแนะนำให้ทำในชายอายุ ≥40 และ หญิงอายุ ≥45)
📷 if CAC >0 --> ให้ statin (class 1)
📷 if CAC =0 --> health behavior counseling
+ repeat CAC 3-7 y (class 1)
📷 Intermediate 10-y risk (5% to <10%)
📷 moderate-high intensity statin (class 1)
(goal = LDL <100 + ลดลง ≥30% to ≥50% + non-HDL C <130) (class 2a)
(ถ้าคนไข้อยู่ใน higher end of this risk range แนะนำให้ใช้ high intensity statin เพื่อลด LDL ≥50%)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (class 1)
📷 พิจารณาให้ statin จาก CAC ในเกณฑ์เดียวกับกรณี borderline 10-y risk ข้างต้น
📷 High 10-y risk (≥10%)
📷 high intensity statin (class 1)
(goal = LDL <70 + ลดลง ≥50% + non-HDL C <100) (class 2a)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe (class 2a)
📷 add PCSK9 mAb or Bempedoic acid
(with or without ezetimibe) (class 2b)
📷 Special consideration
📷 if life expectancy <1 y
📷 อาจพิจารณาหยุดยาลดไขมัน (class 2b)
📷 คนไข้ที่มี baseline untreated LDL <70 และ
non–HDL-C <100 without additional ASCVD
risk factors
📷 ไม่ต้องให้ยา statin (class 3 ; No benefit)
__________________________________________
📷 Calcium score (CAC score)
(Coronary artery calcium score)
นำมาพิจารณาให้ Statin อย่างไร ?
__________________________________________
📷 Calcium score (CAC score)
ควรตรวจในคนไข้รายไหน ?
📷 Men ≥40 or Women ≥45 Years ที่ประเมินความเสี่ยงโดยใช้ PREVENT-ASCVD equations แล้วตกอยู่ในกลุ่ม Intermediate 10-y risk (5% to <10%) หรือ Borderline 10-y risk (3% to <5%) และยังตัดสินใจไม่ได้แน่ชัดว่าควรให้ยา statin หรือไม่
📷 CAC score ตรวจและแปลผลอย่างไร ?
📷 ตรวจโดยใช้ non-contrast-gated cardiac CT
📷 แปลผล
📷 CAC score แสดงถึง overall amount of calcified coronary plaque ซึ่งบ่งบอกถึงการมี subclinical atherosclerosis โดยที่ CAC score ยิ่งสูง ก็จะพยากรณ์ได้ว่าคนไข้ยิ่งมีโอกาสสูงที่จะเกิด MACE (major adverse CV event) ในอนาคต และความสัมพันธ์ระหว่าง CAC score กับการเกิด MACE นี้พบว่าเป็นไปในแบบที่แทบจะเป็น linear relationship เลยทีเดียวครับ
📷 CAC score แบ่งระดับความรุนแรงได้ดังนี้
📷 absent (0 AU)
📷 minimal (1-9 AU)
📷 mild (10-99 AU)
📷 moderate (100-299 AU)
📷 severe (300-999 AU)
📷 extensive (≥1000 AU)
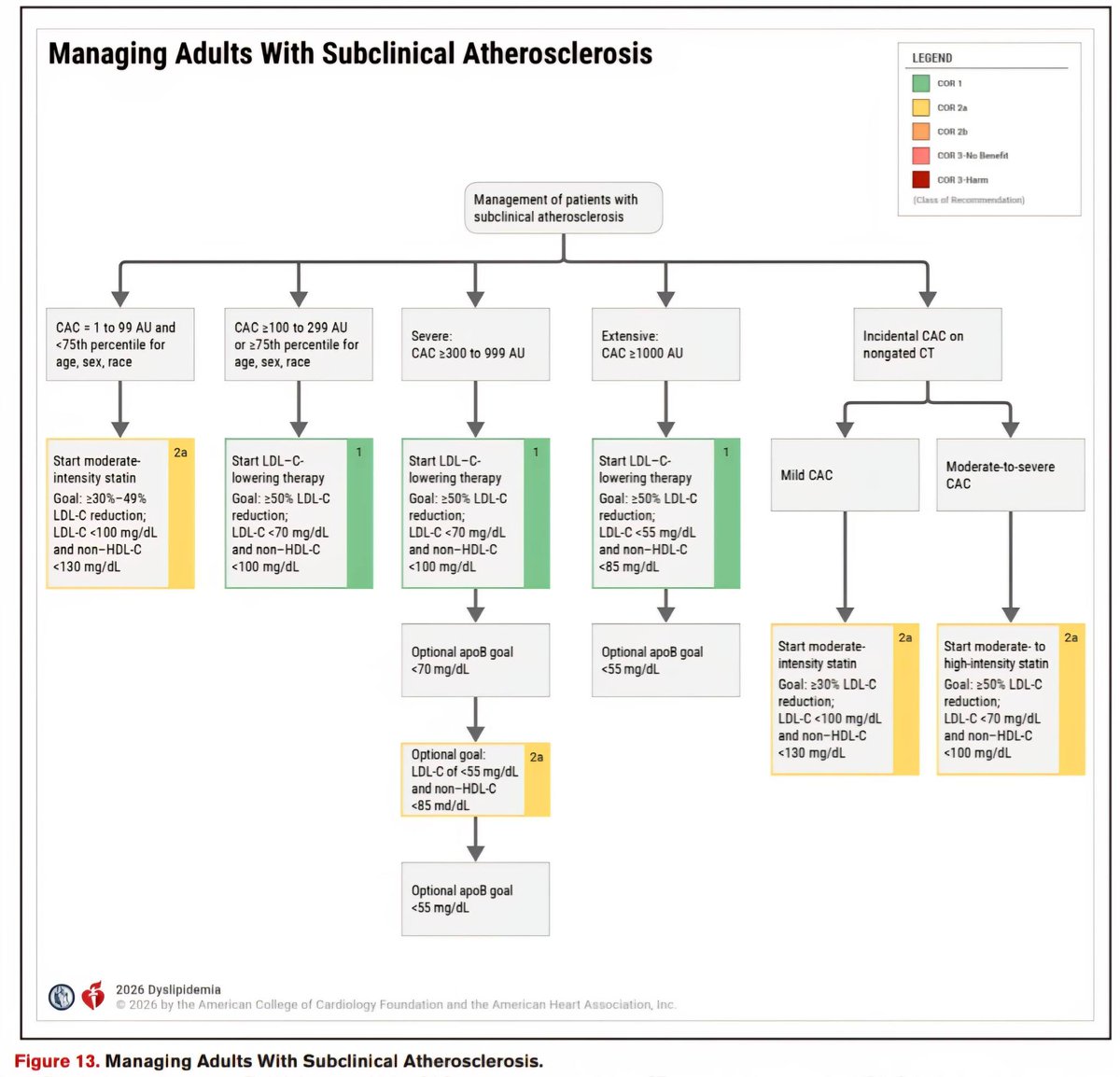
📷 CAC score นำมาพิจารณาให้ Statin อย่างไร ?
📷 CAC score 1-99 AU and <75th standardized percentile for age, sex & race
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 CAC score 100-299 AU or ≥75th standardized percentile for age, sex & race
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1)
📷 CAC score 300-999 AU (severe)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
(โดยใช้วิธีเพิ่ม intensity of statin หรือ add ezetimibe, PCSK9 mAb, or bempedoic
acid) (class 2a)
📷 CAC score ≥1000 AU (extensive)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 incidental finding of mild CAC on noncardiac CT scan
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 moderate-to-severe incidental coronary atherosclerosis identified on noncardiac CT scans (eg, by visual estimation or a validated artificial intelligence-based algorithm)
📷 moderate-high intensity statin (class 2a)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a)
📷 คนไข้ที่มี LDL ต่ำกว่า targets สำหรับแต่ละ CAC levels อยู่แล้วโดยที่ไม่ได้ on statin
📷 ก็ยังแนะนำให้ใช้ยาเพื่อลด LDL ลง ≥30% ด้วยนะครับ
📷 CCTA (coronary CT angiography)
พิจารณาทำในรายไหน ?
📷 อาจพิจารณาทำ CCTA (coronary CT angiography) ในคนไข้ที่ไม่เคยมี ASCVD แต่ likely ที่จะมี high burden of "noncalcified" plaque (eg, inflammatory disorders, HIV, and diabetes) เพื่อช่วยตัดสินใจในการให้ statin (class 2b)
__________________________________________
📷 Severe hypercholesterolemia : LDL ≥190
__________________________________________
📷 without clinical ASCVD, additional ASCVD risk factors, HeFH, or subclinical atherosclerosis
📷 maximally tolerated statin (class 1)
(goal = LDL <100 + non-HDL C <130)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or
bempedoic acid (class 1)
📷 add inclisiran (as alternative to PCSK9 mAb) with or without ezetimibe (class 2a)
(ณ ชั่วโมงนี้ inclisiran ยังถือเป็น second-line PCSK9i โดยยังได้ข้อบ่งชี้เพียงแค่ใช้ลด LDL เท่านั้น เนื่องจากยังต้องรอดู CV benefit จาก CV outcome trials อยู่ครับ)
📷 without clinical ASCVD but with HeFH, additional ASCVD risk factors, or subclinical atherosclerosis (documented coronary calcification)
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <70 + non-HDL C <100
📷 with clinical ASCVD
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <55 + non-HDL C <85 + optional apoB goal <55
__________________________________________
📷 DM without established ASCVD
__________________________________________
📷 อายุ 20-39
📷 moderate-intensity statin ใน 2 กรณี
📷อายุ ≥30 + PREVENT ASCVD 10-y risk ≥3% หรือ 30-y risk ≥10% (class 2a)
📷 มี Diabetes-specific risk enhancer
(DM of long duration [≥10 y of T2DM, ≥20 y of T1DM], albuminuria (≥30 μg of albumin/
mg cr), eGFR <60, retinopathy, neuropathy, or ABI <0.9) (class 2b)
📷 อายุ 40-75
📷 moderate-intensity statin (class 1)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 1) + optional apoB goal <90
📷 high intensity statin (class 2a)
if PREVENT ASCVD 10-y risk ≥10% or multiple ASCVD risk factors
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a) + optional apoB goal <70
📷 add ezetimibe or PCSK9 mAb (class 2b)
if not achieved LDL & non-HDL C goal
📷 add IPE (after a statin) (class 2b)
if additional ASCVD risk factor(s) + LDL<100 + fasting TG 150–499
หมายเหตุ
Additional ASCVD risk factor(s) ในกรณีนี้
ดูจาก REDUCE-IT inclusion criteria ได้แก่
men ≥55 y, women ≥65 y, cigarette smoking or stopped smoking within 3 mo, HT (SBP ≥140 or DBP ≥90 or ใช้ยา HT อยู่), HDL ≤40 for men or ≤50 for women, hs-CRP >3.0 mg/L, CrCl >30 and <60, retinopathy, albuminuria (≥30 μg of albumin/mg Cr), ABI <0.9
📷 อายุ >75 + estimated life expectancy≥2.5y
📷 moderate-intensity statin (class 2b)
📷 ถ้ามี statin-attributed side effects
📷 initiation of ezetimibe and/or bempedoic acid or a PCSK9 mAb (class 1)
__________________________________________
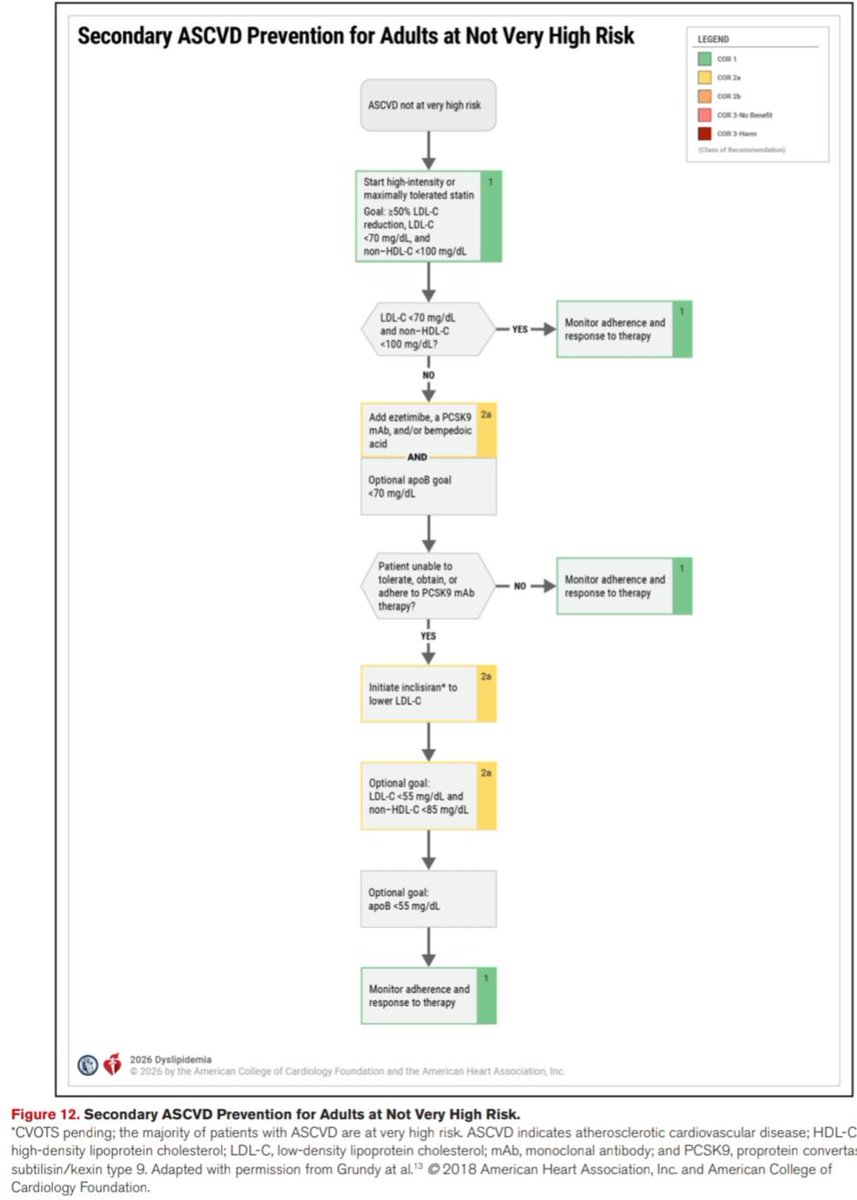
📷 Secondary ASCVD Prevention
__________________________________________
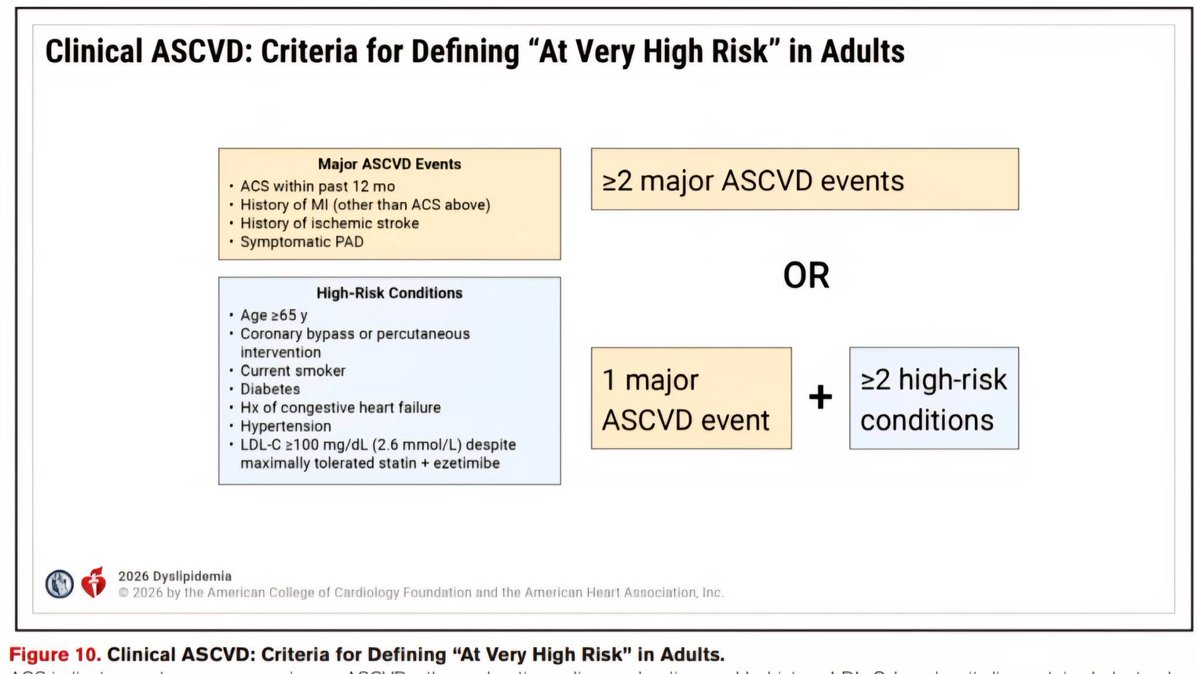
📷 Clinical ASCVD "Not at Very High Risk"
(ดู criteria สำหรับ Very High Risk จากรูปด้านล่างนะครับ)
📷 goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional goal : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or bempedoic acid (class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 Clinical ASCVD "at Very High Risk"
(include ASCVD with CKD)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe and/or PCSK9 mAb
(class 1)
📷 add bempedoic acid, with or
without ezetimibe and/or PCSK9 mAb
(class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 HFrEF Due to ASCVD (IHD) + มี reasonable life expectancy (3–5 y) + not already on a statin
📷 อาจพิจารณาเริ่มให้ moderate-intensity statin เพื่อลด ASCVD events (class 2b)
📷 HFrEF ที่ไม่มี ASCVD + ไม่มีข้อบ่งชี้อื่นของ statin --> ไม่แนะนำให้ statin (class 3 ; No benefit)
__________________________________________
📷 CKD stage 3 or higher
__________________________________________
📷 CKD stage 3 or higher + อายุ 40-75
+ LDL 70-189
📷 แนะนำให้ moderate-intensity statin or moderate-intensity statin + ezetimibe เพื่อลด ASCVD risk (class 1)
📷 CKD stage 3 or higher + clinical ASCVD
📷 แนะนำให้ high-intensity statin with or without ezetimibe and/or a PCSK9 mAb
(goal : LDL <55 + ลดลง ≥50% + non-HDL C <85) (class 1)
📷 CKD ที่ require maintenance hemodialysis
📷 อาจพิจารณา continue statin เพื่อลด risk of ASCVD events โดยพิจารณาจากหลายๆปัจจัย เช่น expected survival, other comorbidities, and severity of ASCVD (class 2b)
__________________________________________
📷 คนไข้ HIV
__________________________________________
📷 คนไข้ HIV อายุ 40-75
📷 แนะนำให้ statin เพื่อลด risk of a first
ASCVD event และลด rate of coronary
atherosclerosis progression (class 1)
__________________________________________
📷 คนไข้ cancer
__________________________________________
📷 if life expectancy ≥ 2 y ให้พิจารณาใช้ statin ได้ตามข้อบ่งชี้เหมือนคนไข้ที่ไม่ได้เป็นมะเร็ง
📷 อาจพิจารณาเริ่มให้ statin เพื่อ prevent anthracycline-induced cardiotoxicity
(class 2b)
__________________________________________
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
ดูจากตารางด้านล่าง
__________________________________________
__________________________________________
📷 Lp(a)
__________________________________________
📷 Lp(a) คืออะไร ?
📷 คือ LDL-like particle ที่มี structure แตกต่างไปจาก LDL โดยจะ carries a single apoprotein(a) strand bound to its apoB-100 component
📷 Lp(a) มีอันตรายอย่างไร ?
📷 Lp(a) เป็น genetic risk factor ในการเกิด ASCVD ครับ (independent of LDL and other risk factors)
📷 ระดับของ Lp(a) ที่สูงจะสัมพันธ์กับการเกิด ASCVD อย่างชัดเจน โดยผ่านกลไกหลายๆอย่าง เช่น proatherogenic and proinflammatory effects ซึ่งส่วนหนึ่งก็ถูกกระตุ้นจาก oxidized phospholipids on Lp(a) นั่นเอง
📷 เจาะแล้วมีประโยชน์อย่างไร ?
📷 เจาะเพื่อ identify คนไข้ที่ increased ASCVD risk (independent of LDL and other risk factors)
📷 ควรเจาะในคนไข้รายไหน ?
📷 in all adults !! ควรเจาะอย่างน้อย 1 ครั้งในชีวิตครับ (class 1)
(ระดับของ Lp(a) จะไม่ค่อยเปลี่ยนแปลงตามกาลเวลา และไม่ค่อยเปลี่ยนแปลงตาม lifestyle factors ด้วยครับ เนื่องจากเป็นปัจจัยทาง genetic ยกเว้น ช่วง menopause transition อาจจะมีค่าเปลี่ยนแปลงได้บ้าง หรือมี secondary cause of elevated Lp(a) เช่น kidney, liver, thyroid disease, pregnancy, certain medications)
📷 เจาะใน first-degree family members ของคนไข้ที่เป็น FH, premature ASCVD, or
high Lp(a) (class 1)
📷 ต้องงดอาหารก่อนเจาะหรือไม่ ?
📷 ไม่ต้อง fasting เลยครับ !!
📷 วิธีลด Lp(a) มีอะไรบ้าง ?
📷 PCSK9i (mAbs and small-interfering
RNA)
--> ลด Lp(a) ได้ ∼15-30%
(ณ ชั่วโมงนี้ PCSK9i ยังไม่ได้รับ FDA-approved for Lp(a) lowering นะครับ แต่ก็เริ่มมีข้อมูลสนับสนุนมากขึ้นเรื่อยๆในแง่ของ clinical outcome)
📷 Specific Lp(a)-lowering therapies
(ลด Lp(a) production ได้แก่ mRNA therapies or oral small-molecule inhibitors)
--> กำลังมีการศึกษาใน randomized clinical outcomes trials อดใจรออีกซักหน่อยนะครับ !!
📷 lipoprotein-apheresis
📷 Lifestyle management
-->ไม่ค่อยมีผลต่อระดับ Lp(a) ครับ เพราะเป็นปัจจัยทาง genetic
📷 statin
--> ไม่มีผลลดระดับ Lp(a) และอาจเพิ่มระดับ Lp(a) เล็กน้อยด้วยซ้ำ โดยเฉลี่ยแล้วจะเพิ่ม ~1.1 mg/dL แต่ก็ถือว่าไม่จำเป็นต้องหยุดใช้ statin นะครับ เนื่องจากมี strong benefit ในการ prevent ASCVD
📷 เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
(Lp(a) ≥50 mg/dL จึงจะถือว่าสูงนะครับ โดยพบได้ ~20% ของประชากร)
📷 คนไข้ที่ยังไม่มี ASCVD
📷 แนะนำให้รีบ optimal early control of modifiable CV risk factors โดยการคุม BP, BS, lipid ให้ดีที่สุด รวมถึงการพิจารณาเริ่มให้หรือ intensified statin เพื่อลด LDL และลด ASCVD risk (class 1)
📷 คนไข้ที่มี clinical ASCVD + elevated Lp(a) + ได้ maximally tolerated statin แล้วยังไม่ achieved LDL and non–HDL goals
📷 ให้ add PCSK9 mAb (class 1)
เพื่อให้ achieved LDL, non–HDL, ApoB goal +
potential additional benefit of moderate Lp(a) lowering
📷 คนไข้ที่ Lp(a) ≥60 mg/dL + FH + (CAD or PAD)
📷 ให้ทำ lipoprotein-apheresis (FDA-approved based on observational data)
__________________________________________
📷 ApoB
__________________________________________
📷 ApoB คืออะไร ?
📷 ApoB เป็นการวัด atherogenic particle number โดยตรง ซึ่งจะมีจำนวน 1 molecule per LDL, VLDL and Lp(a) particle ซึ่งแตกต่างจากตัวเลข LDL ที่จะ reflects ถึง cholesterol mass ที่อยู่ภายใน LDL particles มากกว่าที่จะ reflects ถึง number of atherogenic lipoproteins
(แต่ LDL ยังคงเป็น traditional lipid marker for ASCVD risk assessment and treatment targets อยู่นะครับ)
📷 ApoB มีความสำคัญอย่างไร ?
📷 ApoB สามารถ predicts ASCVD risk ได้
accurate กว่า LDL ใน setting คนไข้ที่มี
discordance กันระหว่างตัวเลข LDL และ ApoB เช่น LDL อยู่ใน target ดีแล้ว แต่ ApoB ยังสูงเกิน goal ซึ่งจะถือว่าคนไข้จะยังมี persistent atherogenic particle burden (ยังมี residual CVD risk in statin-treated populations)
ที่จำเป็นต้องปรับยาเพิ่มต่อครับ โดย pattern แบบนี้มักพบในกลุ่มคนไข้ cardiometabolic disease, including ASCVD, CKM syndrome, diabetes, and/or TG ≥150 mg/dL ซึ่งในกรณีแบบนี้เราจะถือว่า ApoB เป็น more reliable marker for ASCVD risk and therapeutic guidance ครับ
📷 ApoB ยังสัมพันธ์กับการเกิด CV events independent of LDL ด้วยครับ
📷 ตัวเลข ApoB จึงสามารถใช้เป็นได้ทั้ง target ในการใช้ยารักษา และใช้เป็นตัวบอก ASCVD risk ได้ด้วย
📷 ควรเจาะในคนไข้รายไหน ?
📷 คนไข้ที่ใช้ยาลดไขมันอยู่แล้ว โดยเฉพาะคนไข้ที่เป็น ASCVD, CKM syndrome, type 2 diabetes, and/or elevated TG ที่ achieved LDL and/or non–HDL-C goals แล้ว ควรเจาะ ApoB ดูเพื่อช่วยตัดสินใจว่าจะต้องปรับยาเพิ่มต่ออีกหรือไม่ (class 2a)
📷 คนไข้ที่ยังไม่ได้ใช้ยาลดไขมัน อาจพิจารณาเจาะ ApoB เพื่อช่วย enhance ASCVD risk assessment และช่วยตัดสินใจในการเริ่มให้ยา และช่วย characterize inherited lipid disorders (class 2b)
__________________________________________
Reference
📷 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/
AGS/APhA/ASPC/NLA/PCNA Guideline on
the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
13 มี.ค.2026
#dyslipidemia #accahaguideline #ไขมันในเลือดสูง](https://pbs.twimg.com/media/HFrRKQUboAAt2le.jpg)
![AstroRMin10's tweet photo. Bookmark ไว้แล้วทุกคอม (update ASCVD online calculator)
https://t.co/wjkXm4gLTt
#PREVENT #ASCVD
ไม่ได้เชียร์ Statin เบอร์นั้น แต่ถ้าต้องให้ ก็จงให้
----
Credit : คลินิกแพทย์ครรชิต-แพทย์สุวิโชติ เชี่ยวชาญ
https://t.co/rm8RqVA8Od
แนวทางรักษาไขมันสูง ใหม่ล่าสุด 2026 !!
จาก New 2026 ACC/AHA guideline Dyslipid ออกมาเมื่อ 13 มี.ค.2026
📷 สรุปวิธีรักษาไขมันสูง ในคนไข้ 8 กลุ่ม
📷 อายุ 30-79 + LDL 70-189 without ASCVD
📷 Calcium score (CAC score)
• ควรตรวจในคนไข้รายไหน ?
• ตรวจและแปลผลอย่างไร ?
• นำมาพิจารณาให้ Statin อย่างไร ?
📷 Severe hypercholesterolemia : LDL ≥190
📷 DM without established ASCVD
📷 Secondary ASCVD Prevention
📷 CKD stage 3 or higher
📷 คนไข้ HIV
📷 คนไข้มะเร็ง
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
📷 Lp(a)
คืออะไร ?, มีอันตรายอย่างไร ?
เจาะแล้วมีประโยชน์อย่างไร ?
ควรเจาะในคนไข้รายไหน ?
ต้องงดอาหารก่อนเจาะหรือไม่ ?
วิธีลด Lp(a) มีอะไรบ้าง ?
เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
📷 ApoB
คืออะไร ?
มีความสำคัญอย่างไร ?
ควรเจาะในคนไข้รายไหน ?
__________________________________________
📷 อายุ 30-79 + LDL 70-189 without ASCVD
__________________________________________
📷 ประเมิน ASCVD risk ก่อนนะครับ !!
โดยใช้ "PREVENT-ASCVD equations" !!
📷 Low 10-y risk (<3%)
📷 LDL 160-189 or 30-y ASCVD risk ≥10% (สำหรับคนอายุ 30–59 y)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 LDL <160 and 30-y ASCVD risk <10%
📷 health behavior counseling (class 1)
📷 Borderline 10-y risk (3% to <5%)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 ควรประเมิน Risk enhancer (ดูจากตารางด้านล่าง) ประกอบการพิจารณาให้ statin ด้วย
(class 2a)
📷 if high-sensitivity C-reactive protein (hsCRP) ≥2 mg/L on 2 successive occasions โดยไม่มีสาเหตุ
--> ให้ high-intensity statin (class 2a)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (coronary artery calcium) โดยใช้ non-contrast-gated cardiac CT (class 1) (โดยทั่วไปแนะนำให้ทำในชายอายุ ≥40 และ หญิงอายุ ≥45)
📷 if CAC >0 --> ให้ statin (class 1)
📷 if CAC =0 --> health behavior counseling
+ repeat CAC 3-7 y (class 1)
📷 Intermediate 10-y risk (5% to <10%)
📷 moderate-high intensity statin (class 1)
(goal = LDL <100 + ลดลง ≥30% to ≥50% + non-HDL C <130) (class 2a)
(ถ้าคนไข้อยู่ใน higher end of this risk range แนะนำให้ใช้ high intensity statin เพื่อลด LDL ≥50%)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (class 1)
📷 พิจารณาให้ statin จาก CAC ในเกณฑ์เดียวกับกรณี borderline 10-y risk ข้างต้น
📷 High 10-y risk (≥10%)
📷 high intensity statin (class 1)
(goal = LDL <70 + ลดลง ≥50% + non-HDL C <100) (class 2a)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe (class 2a)
📷 add PCSK9 mAb or Bempedoic acid
(with or without ezetimibe) (class 2b)
📷 Special consideration
📷 if life expectancy <1 y
📷 อาจพิจารณาหยุดยาลดไขมัน (class 2b)
📷 คนไข้ที่มี baseline untreated LDL <70 และ
non–HDL-C <100 without additional ASCVD
risk factors
📷 ไม่ต้องให้ยา statin (class 3 ; No benefit)
__________________________________________
📷 Calcium score (CAC score)
(Coronary artery calcium score)
นำมาพิจารณาให้ Statin อย่างไร ?
__________________________________________
📷 Calcium score (CAC score)
ควรตรวจในคนไข้รายไหน ?
📷 Men ≥40 or Women ≥45 Years ที่ประเมินความเสี่ยงโดยใช้ PREVENT-ASCVD equations แล้วตกอยู่ในกลุ่ม Intermediate 10-y risk (5% to <10%) หรือ Borderline 10-y risk (3% to <5%) และยังตัดสินใจไม่ได้แน่ชัดว่าควรให้ยา statin หรือไม่
📷 CAC score ตรวจและแปลผลอย่างไร ?
📷 ตรวจโดยใช้ non-contrast-gated cardiac CT
📷 แปลผล
📷 CAC score แสดงถึง overall amount of calcified coronary plaque ซึ่งบ่งบอกถึงการมี subclinical atherosclerosis โดยที่ CAC score ยิ่งสูง ก็จะพยากรณ์ได้ว่าคนไข้ยิ่งมีโอกาสสูงที่จะเกิด MACE (major adverse CV event) ในอนาคต และความสัมพันธ์ระหว่าง CAC score กับการเกิด MACE นี้พบว่าเป็นไปในแบบที่แทบจะเป็น linear relationship เลยทีเดียวครับ
📷 CAC score แบ่งระดับความรุนแรงได้ดังนี้
📷 absent (0 AU)
📷 minimal (1-9 AU)
📷 mild (10-99 AU)
📷 moderate (100-299 AU)
📷 severe (300-999 AU)
📷 extensive (≥1000 AU)
📷 CAC score นำมาพิจารณาให้ Statin อย่างไร ?
📷 CAC score 1-99 AU and <75th standardized percentile for age, sex & race
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 CAC score 100-299 AU or ≥75th standardized percentile for age, sex & race
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1)
📷 CAC score 300-999 AU (severe)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
(โดยใช้วิธีเพิ่ม intensity of statin หรือ add ezetimibe, PCSK9 mAb, or bempedoic
acid) (class 2a)
📷 CAC score ≥1000 AU (extensive)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 incidental finding of mild CAC on noncardiac CT scan
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 moderate-to-severe incidental coronary atherosclerosis identified on noncardiac CT scans (eg, by visual estimation or a validated artificial intelligence-based algorithm)
📷 moderate-high intensity statin (class 2a)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a)
📷 คนไข้ที่มี LDL ต่ำกว่า targets สำหรับแต่ละ CAC levels อยู่แล้วโดยที่ไม่ได้ on statin
📷 ก็ยังแนะนำให้ใช้ยาเพื่อลด LDL ลง ≥30% ด้วยนะครับ
📷 CCTA (coronary CT angiography)
พิจารณาทำในรายไหน ?
📷 อาจพิจารณาทำ CCTA (coronary CT angiography) ในคนไข้ที่ไม่เคยมี ASCVD แต่ likely ที่จะมี high burden of "noncalcified" plaque (eg, inflammatory disorders, HIV, and diabetes) เพื่อช่วยตัดสินใจในการให้ statin (class 2b)
__________________________________________
📷 Severe hypercholesterolemia : LDL ≥190
__________________________________________
📷 without clinical ASCVD, additional ASCVD risk factors, HeFH, or subclinical atherosclerosis
📷 maximally tolerated statin (class 1)
(goal = LDL <100 + non-HDL C <130)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or
bempedoic acid (class 1)
📷 add inclisiran (as alternative to PCSK9 mAb) with or without ezetimibe (class 2a)
(ณ ชั่วโมงนี้ inclisiran ยังถือเป็น second-line PCSK9i โดยยังได้ข้อบ่งชี้เพียงแค่ใช้ลด LDL เท่านั้น เนื่องจากยังต้องรอดู CV benefit จาก CV outcome trials อยู่ครับ)
📷 without clinical ASCVD but with HeFH, additional ASCVD risk factors, or subclinical atherosclerosis (documented coronary calcification)
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <70 + non-HDL C <100
📷 with clinical ASCVD
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <55 + non-HDL C <85 + optional apoB goal <55
__________________________________________
📷 DM without established ASCVD
__________________________________________
📷 อายุ 20-39
📷 moderate-intensity statin ใน 2 กรณี
📷อายุ ≥30 + PREVENT ASCVD 10-y risk ≥3% หรือ 30-y risk ≥10% (class 2a)
📷 มี Diabetes-specific risk enhancer
(DM of long duration [≥10 y of T2DM, ≥20 y of T1DM], albuminuria (≥30 μg of albumin/
mg cr), eGFR <60, retinopathy, neuropathy, or ABI <0.9) (class 2b)
📷 อายุ 40-75
📷 moderate-intensity statin (class 1)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 1) + optional apoB goal <90
📷 high intensity statin (class 2a)
if PREVENT ASCVD 10-y risk ≥10% or multiple ASCVD risk factors
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a) + optional apoB goal <70
📷 add ezetimibe or PCSK9 mAb (class 2b)
if not achieved LDL & non-HDL C goal
📷 add IPE (after a statin) (class 2b)
if additional ASCVD risk factor(s) + LDL<100 + fasting TG 150–499
หมายเหตุ
Additional ASCVD risk factor(s) ในกรณีนี้
ดูจาก REDUCE-IT inclusion criteria ได้แก่
men ≥55 y, women ≥65 y, cigarette smoking or stopped smoking within 3 mo, HT (SBP ≥140 or DBP ≥90 or ใช้ยา HT อยู่), HDL ≤40 for men or ≤50 for women, hs-CRP >3.0 mg/L, CrCl >30 and <60, retinopathy, albuminuria (≥30 μg of albumin/mg Cr), ABI <0.9
📷 อายุ >75 + estimated life expectancy≥2.5y
📷 moderate-intensity statin (class 2b)
📷 ถ้ามี statin-attributed side effects
📷 initiation of ezetimibe and/or bempedoic acid or a PCSK9 mAb (class 1)
__________________________________________
📷 Secondary ASCVD Prevention
__________________________________________
📷 Clinical ASCVD "Not at Very High Risk"
(ดู criteria สำหรับ Very High Risk จากรูปด้านล่างนะครับ)
📷 goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional goal : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or bempedoic acid (class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 Clinical ASCVD "at Very High Risk"
(include ASCVD with CKD)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe and/or PCSK9 mAb
(class 1)
📷 add bempedoic acid, with or
without ezetimibe and/or PCSK9 mAb
(class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 HFrEF Due to ASCVD (IHD) + มี reasonable life expectancy (3–5 y) + not already on a statin
📷 อาจพิจารณาเริ่มให้ moderate-intensity statin เพื่อลด ASCVD events (class 2b)
📷 HFrEF ที่ไม่มี ASCVD + ไม่มีข้อบ่งชี้อื่นของ statin --> ไม่แนะนำให้ statin (class 3 ; No benefit)
__________________________________________
📷 CKD stage 3 or higher
__________________________________________
📷 CKD stage 3 or higher + อายุ 40-75
+ LDL 70-189
📷 แนะนำให้ moderate-intensity statin or moderate-intensity statin + ezetimibe เพื่อลด ASCVD risk (class 1)
📷 CKD stage 3 or higher + clinical ASCVD
📷 แนะนำให้ high-intensity statin with or without ezetimibe and/or a PCSK9 mAb
(goal : LDL <55 + ลดลง ≥50% + non-HDL C <85) (class 1)
📷 CKD ที่ require maintenance hemodialysis
📷 อาจพิจารณา continue statin เพื่อลด risk of ASCVD events โดยพิจารณาจากหลายๆปัจจัย เช่น expected survival, other comorbidities, and severity of ASCVD (class 2b)
__________________________________________
📷 คนไข้ HIV
__________________________________________
📷 คนไข้ HIV อายุ 40-75
📷 แนะนำให้ statin เพื่อลด risk of a first
ASCVD event และลด rate of coronary
atherosclerosis progression (class 1)
__________________________________________
📷 คนไข้ cancer
__________________________________________
📷 if life expectancy ≥ 2 y ให้พิจารณาใช้ statin ได้ตามข้อบ่งชี้เหมือนคนไข้ที่ไม่ได้เป็นมะเร็ง
📷 อาจพิจารณาเริ่มให้ statin เพื่อ prevent anthracycline-induced cardiotoxicity
(class 2b)
__________________________________________
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
ดูจากตารางด้านล่าง
__________________________________________
__________________________________________
📷 Lp(a)
__________________________________________
📷 Lp(a) คืออะไร ?
📷 คือ LDL-like particle ที่มี structure แตกต่างไปจาก LDL โดยจะ carries a single apoprotein(a) strand bound to its apoB-100 component
📷 Lp(a) มีอันตรายอย่างไร ?
📷 Lp(a) เป็น genetic risk factor ในการเกิด ASCVD ครับ (independent of LDL and other risk factors)
📷 ระดับของ Lp(a) ที่สูงจะสัมพันธ์กับการเกิด ASCVD อย่างชัดเจน โดยผ่านกลไกหลายๆอย่าง เช่น proatherogenic and proinflammatory effects ซึ่งส่วนหนึ่งก็ถูกกระตุ้นจาก oxidized phospholipids on Lp(a) นั่นเอง
📷 เจาะแล้วมีประโยชน์อย่างไร ?
📷 เจาะเพื่อ identify คนไข้ที่ increased ASCVD risk (independent of LDL and other risk factors)
📷 ควรเจาะในคนไข้รายไหน ?
📷 in all adults !! ควรเจาะอย่างน้อย 1 ครั้งในชีวิตครับ (class 1)
(ระดับของ Lp(a) จะไม่ค่อยเปลี่ยนแปลงตามกาลเวลา และไม่ค่อยเปลี่ยนแปลงตาม lifestyle factors ด้วยครับ เนื่องจากเป็นปัจจัยทาง genetic ยกเว้น ช่วง menopause transition อาจจะมีค่าเปลี่ยนแปลงได้บ้าง หรือมี secondary cause of elevated Lp(a) เช่น kidney, liver, thyroid disease, pregnancy, certain medications)
📷 เจาะใน first-degree family members ของคนไข้ที่เป็น FH, premature ASCVD, or
high Lp(a) (class 1)
📷 ต้องงดอาหารก่อนเจาะหรือไม่ ?
📷 ไม่ต้อง fasting เลยครับ !!
📷 วิธีลด Lp(a) มีอะไรบ้าง ?
📷 PCSK9i (mAbs and small-interfering
RNA)
--> ลด Lp(a) ได้ ∼15-30%
(ณ ชั่วโมงนี้ PCSK9i ยังไม่ได้รับ FDA-approved for Lp(a) lowering นะครับ แต่ก็เริ่มมีข้อมูลสนับสนุนมากขึ้นเรื่อยๆในแง่ของ clinical outcome)
📷 Specific Lp(a)-lowering therapies
(ลด Lp(a) production ได้แก่ mRNA therapies or oral small-molecule inhibitors)
--> กำลังมีการศึกษาใน randomized clinical outcomes trials อดใจรออีกซักหน่อยนะครับ !!
📷 lipoprotein-apheresis
📷 Lifestyle management
-->ไม่ค่อยมีผลต่อระดับ Lp(a) ครับ เพราะเป็นปัจจัยทาง genetic
📷 statin
--> ไม่มีผลลดระดับ Lp(a) และอาจเพิ่มระดับ Lp(a) เล็กน้อยด้วยซ้ำ โดยเฉลี่ยแล้วจะเพิ่ม ~1.1 mg/dL แต่ก็ถือว่าไม่จำเป็นต้องหยุดใช้ statin นะครับ เนื่องจากมี strong benefit ในการ prevent ASCVD
📷 เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
(Lp(a) ≥50 mg/dL จึงจะถือว่าสูงนะครับ โดยพบได้ ~20% ของประชากร)
📷 คนไข้ที่ยังไม่มี ASCVD
📷 แนะนำให้รีบ optimal early control of modifiable CV risk factors โดยการคุม BP, BS, lipid ให้ดีที่สุด รวมถึงการพิจารณาเริ่มให้หรือ intensified statin เพื่อลด LDL และลด ASCVD risk (class 1)
📷 คนไข้ที่มี clinical ASCVD + elevated Lp(a) + ได้ maximally tolerated statin แล้วยังไม่ achieved LDL and non–HDL goals
📷 ให้ add PCSK9 mAb (class 1)
เพื่อให้ achieved LDL, non–HDL, ApoB goal +
potential additional benefit of moderate Lp(a) lowering
📷 คนไข้ที่ Lp(a) ≥60 mg/dL + FH + (CAD or PAD)
📷 ให้ทำ lipoprotein-apheresis (FDA-approved based on observational data)
__________________________________________
📷 ApoB
__________________________________________
📷 ApoB คืออะไร ?
📷 ApoB เป็นการวัด atherogenic particle number โดยตรง ซึ่งจะมีจำนวน 1 molecule per LDL, VLDL and Lp(a) particle ซึ่งแตกต่างจากตัวเลข LDL ที่จะ reflects ถึง cholesterol mass ที่อยู่ภายใน LDL particles มากกว่าที่จะ reflects ถึง number of atherogenic lipoproteins
(แต่ LDL ยังคงเป็น traditional lipid marker for ASCVD risk assessment and treatment targets อยู่นะครับ)
📷 ApoB มีความสำคัญอย่างไร ?
📷 ApoB สามารถ predicts ASCVD risk ได้
accurate กว่า LDL ใน setting คนไข้ที่มี
discordance กันระหว่างตัวเลข LDL และ ApoB เช่น LDL อยู่ใน target ดีแล้ว แต่ ApoB ยังสูงเกิน goal ซึ่งจะถือว่าคนไข้จะยังมี persistent atherogenic particle burden (ยังมี residual CVD risk in statin-treated populations)
ที่จำเป็นต้องปรับยาเพิ่มต่อครับ โดย pattern แบบนี้มักพบในกลุ่มคนไข้ cardiometabolic disease, including ASCVD, CKM syndrome, diabetes, and/or TG ≥150 mg/dL ซึ่งในกรณีแบบนี้เราจะถือว่า ApoB เป็น more reliable marker for ASCVD risk and therapeutic guidance ครับ
📷 ApoB ยังสัมพันธ์กับการเกิด CV events independent of LDL ด้วยครับ
📷 ตัวเลข ApoB จึงสามารถใช้เป็นได้ทั้ง target ในการใช้ยารักษา และใช้เป็นตัวบอก ASCVD risk ได้ด้วย
📷 ควรเจาะในคนไข้รายไหน ?
📷 คนไข้ที่ใช้ยาลดไขมันอยู่แล้ว โดยเฉพาะคนไข้ที่เป็น ASCVD, CKM syndrome, type 2 diabetes, and/or elevated TG ที่ achieved LDL and/or non–HDL-C goals แล้ว ควรเจาะ ApoB ดูเพื่อช่วยตัดสินใจว่าจะต้องปรับยาเพิ่มต่ออีกหรือไม่ (class 2a)
📷 คนไข้ที่ยังไม่ได้ใช้ยาลดไขมัน อาจพิจารณาเจาะ ApoB เพื่อช่วย enhance ASCVD risk assessment และช่วยตัดสินใจในการเริ่มให้ยา และช่วย characterize inherited lipid disorders (class 2b)
__________________________________________
Reference
📷 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/
AGS/APhA/ASPC/NLA/PCNA Guideline on
the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
13 มี.ค.2026
#dyslipidemia #accahaguideline #ไขมันในเลือดสูง](https://pbs.twimg.com/media/HFrRKQPbwAAryUR.jpg)
![AstroRMin10's tweet photo. Bookmark ไว้แล้วทุกคอม (update ASCVD online calculator)
https://t.co/wjkXm4gLTt
#PREVENT #ASCVD
ไม่ได้เชียร์ Statin เบอร์นั้น แต่ถ้าต้องให้ ก็จงให้
----
Credit : คลินิกแพทย์ครรชิต-แพทย์สุวิโชติ เชี่ยวชาญ
https://t.co/rm8RqVA8Od
แนวทางรักษาไขมันสูง ใหม่ล่าสุด 2026 !!
จาก New 2026 ACC/AHA guideline Dyslipid ออกมาเมื่อ 13 มี.ค.2026
📷 สรุปวิธีรักษาไขมันสูง ในคนไข้ 8 กลุ่ม
📷 อายุ 30-79 + LDL 70-189 without ASCVD
📷 Calcium score (CAC score)
• ควรตรวจในคนไข้รายไหน ?
• ตรวจและแปลผลอย่างไร ?
• นำมาพิจารณาให้ Statin อย่างไร ?
📷 Severe hypercholesterolemia : LDL ≥190
📷 DM without established ASCVD
📷 Secondary ASCVD Prevention
📷 CKD stage 3 or higher
📷 คนไข้ HIV
📷 คนไข้มะเร็ง
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
📷 Lp(a)
คืออะไร ?, มีอันตรายอย่างไร ?
เจาะแล้วมีประโยชน์อย่างไร ?
ควรเจาะในคนไข้รายไหน ?
ต้องงดอาหารก่อนเจาะหรือไม่ ?
วิธีลด Lp(a) มีอะไรบ้าง ?
เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
📷 ApoB
คืออะไร ?
มีความสำคัญอย่างไร ?
ควรเจาะในคนไข้รายไหน ?
__________________________________________
📷 อายุ 30-79 + LDL 70-189 without ASCVD
__________________________________________
📷 ประเมิน ASCVD risk ก่อนนะครับ !!
โดยใช้ "PREVENT-ASCVD equations" !!
📷 Low 10-y risk (<3%)
📷 LDL 160-189 or 30-y ASCVD risk ≥10% (สำหรับคนอายุ 30–59 y)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 LDL <160 and 30-y ASCVD risk <10%
📷 health behavior counseling (class 1)
📷 Borderline 10-y risk (3% to <5%)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 ควรประเมิน Risk enhancer (ดูจากตารางด้านล่าง) ประกอบการพิจารณาให้ statin ด้วย
(class 2a)
📷 if high-sensitivity C-reactive protein (hsCRP) ≥2 mg/L on 2 successive occasions โดยไม่มีสาเหตุ
--> ให้ high-intensity statin (class 2a)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (coronary artery calcium) โดยใช้ non-contrast-gated cardiac CT (class 1) (โดยทั่วไปแนะนำให้ทำในชายอายุ ≥40 และ หญิงอายุ ≥45)
📷 if CAC >0 --> ให้ statin (class 1)
📷 if CAC =0 --> health behavior counseling
+ repeat CAC 3-7 y (class 1)
📷 Intermediate 10-y risk (5% to <10%)
📷 moderate-high intensity statin (class 1)
(goal = LDL <100 + ลดลง ≥30% to ≥50% + non-HDL C <130) (class 2a)
(ถ้าคนไข้อยู่ใน higher end of this risk range แนะนำให้ใช้ high intensity statin เพื่อลด LDL ≥50%)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (class 1)
📷 พิจารณาให้ statin จาก CAC ในเกณฑ์เดียวกับกรณี borderline 10-y risk ข้างต้น
📷 High 10-y risk (≥10%)
📷 high intensity statin (class 1)
(goal = LDL <70 + ลดลง ≥50% + non-HDL C <100) (class 2a)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe (class 2a)
📷 add PCSK9 mAb or Bempedoic acid
(with or without ezetimibe) (class 2b)
📷 Special consideration
📷 if life expectancy <1 y
📷 อาจพิจารณาหยุดยาลดไขมัน (class 2b)
📷 คนไข้ที่มี baseline untreated LDL <70 และ
non–HDL-C <100 without additional ASCVD
risk factors
📷 ไม่ต้องให้ยา statin (class 3 ; No benefit)
__________________________________________
📷 Calcium score (CAC score)
(Coronary artery calcium score)
นำมาพิจารณาให้ Statin อย่างไร ?
__________________________________________
📷 Calcium score (CAC score)
ควรตรวจในคนไข้รายไหน ?
📷 Men ≥40 or Women ≥45 Years ที่ประเมินความเสี่ยงโดยใช้ PREVENT-ASCVD equations แล้วตกอยู่ในกลุ่ม Intermediate 10-y risk (5% to <10%) หรือ Borderline 10-y risk (3% to <5%) และยังตัดสินใจไม่ได้แน่ชัดว่าควรให้ยา statin หรือไม่
📷 CAC score ตรวจและแปลผลอย่างไร ?
📷 ตรวจโดยใช้ non-contrast-gated cardiac CT
📷 แปลผล
📷 CAC score แสดงถึง overall amount of calcified coronary plaque ซึ่งบ่งบอกถึงการมี subclinical atherosclerosis โดยที่ CAC score ยิ่งสูง ก็จะพยากรณ์ได้ว่าคนไข้ยิ่งมีโอกาสสูงที่จะเกิด MACE (major adverse CV event) ในอนาคต และความสัมพันธ์ระหว่าง CAC score กับการเกิด MACE นี้พบว่าเป็นไปในแบบที่แทบจะเป็น linear relationship เลยทีเดียวครับ
📷 CAC score แบ่งระดับความรุนแรงได้ดังนี้
📷 absent (0 AU)
📷 minimal (1-9 AU)
📷 mild (10-99 AU)
📷 moderate (100-299 AU)
📷 severe (300-999 AU)
📷 extensive (≥1000 AU)
📷 CAC score นำมาพิจารณาให้ Statin อย่างไร ?
📷 CAC score 1-99 AU and <75th standardized percentile for age, sex & race
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 CAC score 100-299 AU or ≥75th standardized percentile for age, sex & race
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1)
📷 CAC score 300-999 AU (severe)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
(โดยใช้วิธีเพิ่ม intensity of statin หรือ add ezetimibe, PCSK9 mAb, or bempedoic
acid) (class 2a)
📷 CAC score ≥1000 AU (extensive)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 incidental finding of mild CAC on noncardiac CT scan
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 moderate-to-severe incidental coronary atherosclerosis identified on noncardiac CT scans (eg, by visual estimation or a validated artificial intelligence-based algorithm)
📷 moderate-high intensity statin (class 2a)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a)
📷 คนไข้ที่มี LDL ต่ำกว่า targets สำหรับแต่ละ CAC levels อยู่แล้วโดยที่ไม่ได้ on statin
📷 ก็ยังแนะนำให้ใช้ยาเพื่อลด LDL ลง ≥30% ด้วยนะครับ
📷 CCTA (coronary CT angiography)
พิจารณาทำในรายไหน ?
📷 อาจพิจารณาทำ CCTA (coronary CT angiography) ในคนไข้ที่ไม่เคยมี ASCVD แต่ likely ที่จะมี high burden of "noncalcified" plaque (eg, inflammatory disorders, HIV, and diabetes) เพื่อช่วยตัดสินใจในการให้ statin (class 2b)
__________________________________________
📷 Severe hypercholesterolemia : LDL ≥190
__________________________________________
📷 without clinical ASCVD, additional ASCVD risk factors, HeFH, or subclinical atherosclerosis
📷 maximally tolerated statin (class 1)
(goal = LDL <100 + non-HDL C <130)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or
bempedoic acid (class 1)
📷 add inclisiran (as alternative to PCSK9 mAb) with or without ezetimibe (class 2a)
(ณ ชั่วโมงนี้ inclisiran ยังถือเป็น second-line PCSK9i โดยยังได้ข้อบ่งชี้เพียงแค่ใช้ลด LDL เท่านั้น เนื่องจากยังต้องรอดู CV benefit จาก CV outcome trials อยู่ครับ)
📷 without clinical ASCVD but with HeFH, additional ASCVD risk factors, or subclinical atherosclerosis (documented coronary calcification)
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <70 + non-HDL C <100
📷 with clinical ASCVD
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <55 + non-HDL C <85 + optional apoB goal <55
__________________________________________
📷 DM without established ASCVD
__________________________________________
📷 อายุ 20-39
📷 moderate-intensity statin ใน 2 กรณี
📷อายุ ≥30 + PREVENT ASCVD 10-y risk ≥3% หรือ 30-y risk ≥10% (class 2a)
📷 มี Diabetes-specific risk enhancer
(DM of long duration [≥10 y of T2DM, ≥20 y of T1DM], albuminuria (≥30 μg of albumin/
mg cr), eGFR <60, retinopathy, neuropathy, or ABI <0.9) (class 2b)
📷 อายุ 40-75
📷 moderate-intensity statin (class 1)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 1) + optional apoB goal <90
📷 high intensity statin (class 2a)
if PREVENT ASCVD 10-y risk ≥10% or multiple ASCVD risk factors
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a) + optional apoB goal <70
📷 add ezetimibe or PCSK9 mAb (class 2b)
if not achieved LDL & non-HDL C goal
📷 add IPE (after a statin) (class 2b)
if additional ASCVD risk factor(s) + LDL<100 + fasting TG 150–499
หมายเหตุ
Additional ASCVD risk factor(s) ในกรณีนี้
ดูจาก REDUCE-IT inclusion criteria ได้แก่
men ≥55 y, women ≥65 y, cigarette smoking or stopped smoking within 3 mo, HT (SBP ≥140 or DBP ≥90 or ใช้ยา HT อยู่), HDL ≤40 for men or ≤50 for women, hs-CRP >3.0 mg/L, CrCl >30 and <60, retinopathy, albuminuria (≥30 μg of albumin/mg Cr), ABI <0.9
📷 อายุ >75 + estimated life expectancy≥2.5y
📷 moderate-intensity statin (class 2b)
📷 ถ้ามี statin-attributed side effects
📷 initiation of ezetimibe and/or bempedoic acid or a PCSK9 mAb (class 1)
__________________________________________
📷 Secondary ASCVD Prevention
__________________________________________
📷 Clinical ASCVD "Not at Very High Risk"
(ดู criteria สำหรับ Very High Risk จากรูปด้านล่างนะครับ)
📷 goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional goal : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or bempedoic acid (class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 Clinical ASCVD "at Very High Risk"
(include ASCVD with CKD)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe and/or PCSK9 mAb
(class 1)
📷 add bempedoic acid, with or
without ezetimibe and/or PCSK9 mAb
(class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 HFrEF Due to ASCVD (IHD) + มี reasonable life expectancy (3–5 y) + not already on a statin
📷 อาจพิจารณาเริ่มให้ moderate-intensity statin เพื่อลด ASCVD events (class 2b)
📷 HFrEF ที่ไม่มี ASCVD + ไม่มีข้อบ่งชี้อื่นของ statin --> ไม่แนะนำให้ statin (class 3 ; No benefit)
__________________________________________
📷 CKD stage 3 or higher
__________________________________________
📷 CKD stage 3 or higher + อายุ 40-75
+ LDL 70-189
📷 แนะนำให้ moderate-intensity statin or moderate-intensity statin + ezetimibe เพื่อลด ASCVD risk (class 1)
📷 CKD stage 3 or higher + clinical ASCVD
📷 แนะนำให้ high-intensity statin with or without ezetimibe and/or a PCSK9 mAb
(goal : LDL <55 + ลดลง ≥50% + non-HDL C <85) (class 1)
📷 CKD ที่ require maintenance hemodialysis
📷 อาจพิจารณา continue statin เพื่อลด risk of ASCVD events โดยพิจารณาจากหลายๆปัจจัย เช่น expected survival, other comorbidities, and severity of ASCVD (class 2b)
__________________________________________
📷 คนไข้ HIV
__________________________________________
📷 คนไข้ HIV อายุ 40-75
📷 แนะนำให้ statin เพื่อลด risk of a first
ASCVD event และลด rate of coronary
atherosclerosis progression (class 1)
__________________________________________
📷 คนไข้ cancer
__________________________________________
📷 if life expectancy ≥ 2 y ให้พิจารณาใช้ statin ได้ตามข้อบ่งชี้เหมือนคนไข้ที่ไม่ได้เป็นมะเร็ง
📷 อาจพิจารณาเริ่มให้ statin เพื่อ prevent anthracycline-induced cardiotoxicity
(class 2b)
__________________________________________
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
ดูจากตารางด้านล่าง
__________________________________________
__________________________________________
📷 Lp(a)
__________________________________________
📷 Lp(a) คืออะไร ?
📷 คือ LDL-like particle ที่มี structure แตกต่างไปจาก LDL โดยจะ carries a single apoprotein(a) strand bound to its apoB-100 component
📷 Lp(a) มีอันตรายอย่างไร ?
📷 Lp(a) เป็น genetic risk factor ในการเกิด ASCVD ครับ (independent of LDL and other risk factors)
📷 ระดับของ Lp(a) ที่สูงจะสัมพันธ์กับการเกิด ASCVD อย่างชัดเจน โดยผ่านกลไกหลายๆอย่าง เช่น proatherogenic and proinflammatory effects ซึ่งส่วนหนึ่งก็ถูกกระตุ้นจาก oxidized phospholipids on Lp(a) นั่นเอง
📷 เจาะแล้วมีประโยชน์อย่างไร ?
📷 เจาะเพื่อ identify คนไข้ที่ increased ASCVD risk (independent of LDL and other risk factors)
📷 ควรเจาะในคนไข้รายไหน ?
📷 in all adults !! ควรเจาะอย่างน้อย 1 ครั้งในชีวิตครับ (class 1)
(ระดับของ Lp(a) จะไม่ค่อยเปลี่ยนแปลงตามกาลเวลา และไม่ค่อยเปลี่ยนแปลงตาม lifestyle factors ด้วยครับ เนื่องจากเป็นปัจจัยทาง genetic ยกเว้น ช่วง menopause transition อาจจะมีค่าเปลี่ยนแปลงได้บ้าง หรือมี secondary cause of elevated Lp(a) เช่น kidney, liver, thyroid disease, pregnancy, certain medications)
📷 เจาะใน first-degree family members ของคนไข้ที่เป็น FH, premature ASCVD, or
high Lp(a) (class 1)
📷 ต้องงดอาหารก่อนเจาะหรือไม่ ?
📷 ไม่ต้อง fasting เลยครับ !!
📷 วิธีลด Lp(a) มีอะไรบ้าง ?
📷 PCSK9i (mAbs and small-interfering
RNA)
--> ลด Lp(a) ได้ ∼15-30%
(ณ ชั่วโมงนี้ PCSK9i ยังไม่ได้รับ FDA-approved for Lp(a) lowering นะครับ แต่ก็เริ่มมีข้อมูลสนับสนุนมากขึ้นเรื่อยๆในแง่ของ clinical outcome)
📷 Specific Lp(a)-lowering therapies
(ลด Lp(a) production ได้แก่ mRNA therapies or oral small-molecule inhibitors)
--> กำลังมีการศึกษาใน randomized clinical outcomes trials อดใจรออีกซักหน่อยนะครับ !!
📷 lipoprotein-apheresis
📷 Lifestyle management
-->ไม่ค่อยมีผลต่อระดับ Lp(a) ครับ เพราะเป็นปัจจัยทาง genetic
📷 statin
--> ไม่มีผลลดระดับ Lp(a) และอาจเพิ่มระดับ Lp(a) เล็กน้อยด้วยซ้ำ โดยเฉลี่ยแล้วจะเพิ่ม ~1.1 mg/dL แต่ก็ถือว่าไม่จำเป็นต้องหยุดใช้ statin นะครับ เนื่องจากมี strong benefit ในการ prevent ASCVD
📷 เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
(Lp(a) ≥50 mg/dL จึงจะถือว่าสูงนะครับ โดยพบได้ ~20% ของประชากร)
📷 คนไข้ที่ยังไม่มี ASCVD
📷 แนะนำให้รีบ optimal early control of modifiable CV risk factors โดยการคุม BP, BS, lipid ให้ดีที่สุด รวมถึงการพิจารณาเริ่มให้หรือ intensified statin เพื่อลด LDL และลด ASCVD risk (class 1)
📷 คนไข้ที่มี clinical ASCVD + elevated Lp(a) + ได้ maximally tolerated statin แล้วยังไม่ achieved LDL and non–HDL goals
📷 ให้ add PCSK9 mAb (class 1)
เพื่อให้ achieved LDL, non–HDL, ApoB goal +
potential additional benefit of moderate Lp(a) lowering
📷 คนไข้ที่ Lp(a) ≥60 mg/dL + FH + (CAD or PAD)
📷 ให้ทำ lipoprotein-apheresis (FDA-approved based on observational data)
__________________________________________
📷 ApoB
__________________________________________
📷 ApoB คืออะไร ?
📷 ApoB เป็นการวัด atherogenic particle number โดยตรง ซึ่งจะมีจำนวน 1 molecule per LDL, VLDL and Lp(a) particle ซึ่งแตกต่างจากตัวเลข LDL ที่จะ reflects ถึง cholesterol mass ที่อยู่ภายใน LDL particles มากกว่าที่จะ reflects ถึง number of atherogenic lipoproteins
(แต่ LDL ยังคงเป็น traditional lipid marker for ASCVD risk assessment and treatment targets อยู่นะครับ)
📷 ApoB มีความสำคัญอย่างไร ?
📷 ApoB สามารถ predicts ASCVD risk ได้
accurate กว่า LDL ใน setting คนไข้ที่มี
discordance กันระหว่างตัวเลข LDL และ ApoB เช่น LDL อยู่ใน target ดีแล้ว แต่ ApoB ยังสูงเกิน goal ซึ่งจะถือว่าคนไข้จะยังมี persistent atherogenic particle burden (ยังมี residual CVD risk in statin-treated populations)
ที่จำเป็นต้องปรับยาเพิ่มต่อครับ โดย pattern แบบนี้มักพบในกลุ่มคนไข้ cardiometabolic disease, including ASCVD, CKM syndrome, diabetes, and/or TG ≥150 mg/dL ซึ่งในกรณีแบบนี้เราจะถือว่า ApoB เป็น more reliable marker for ASCVD risk and therapeutic guidance ครับ
📷 ApoB ยังสัมพันธ์กับการเกิด CV events independent of LDL ด้วยครับ
📷 ตัวเลข ApoB จึงสามารถใช้เป็นได้ทั้ง target ในการใช้ยารักษา และใช้เป็นตัวบอก ASCVD risk ได้ด้วย
📷 ควรเจาะในคนไข้รายไหน ?
📷 คนไข้ที่ใช้ยาลดไขมันอยู่แล้ว โดยเฉพาะคนไข้ที่เป็น ASCVD, CKM syndrome, type 2 diabetes, and/or elevated TG ที่ achieved LDL and/or non–HDL-C goals แล้ว ควรเจาะ ApoB ดูเพื่อช่วยตัดสินใจว่าจะต้องปรับยาเพิ่มต่ออีกหรือไม่ (class 2a)
📷 คนไข้ที่ยังไม่ได้ใช้ยาลดไขมัน อาจพิจารณาเจาะ ApoB เพื่อช่วย enhance ASCVD risk assessment และช่วยตัดสินใจในการเริ่มให้ยา และช่วย characterize inherited lipid disorders (class 2b)
__________________________________________
Reference
📷 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/
AGS/APhA/ASPC/NLA/PCNA Guideline on
the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
13 มี.ค.2026
#dyslipidemia #accahaguideline #ไขมันในเลือดสูง](https://pbs.twimg.com/media/HFrRKQPbQAAVpyv.jpg)

















![AstroRMin10's tweet photo. Bookmark ไว้แล้วทุกคอม (update ASCVD online calculator)
https://t.co/wjkXm4gLTt
#PREVENT #ASCVD
ไม่ได้เชียร์ Statin เบอร์นั้น แต่ถ้าต้องให้ ก็จงให้
----
Credit : คลินิกแพทย์ครรชิต-แพทย์สุวิโชติ เชี่ยวชาญ
https://t.co/rm8RqVA8Od
แนวทางรักษาไขมันสูง ใหม่ล่าสุด 2026 !!
จาก New 2026 ACC/AHA guideline Dyslipid ออกมาเมื่อ 13 มี.ค.2026
📷 สรุปวิธีรักษาไขมันสูง ในคนไข้ 8 กลุ่ม
📷 อายุ 30-79 + LDL 70-189 without ASCVD
📷 Calcium score (CAC score)
• ควรตรวจในคนไข้รายไหน ?
• ตรวจและแปลผลอย่างไร ?
• นำมาพิจารณาให้ Statin อย่างไร ?
📷 Severe hypercholesterolemia : LDL ≥190
📷 DM without established ASCVD
📷 Secondary ASCVD Prevention
📷 CKD stage 3 or higher
📷 คนไข้ HIV
📷 คนไข้มะเร็ง
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
📷 Lp(a)
คืออะไร ?, มีอันตรายอย่างไร ?
เจาะแล้วมีประโยชน์อย่างไร ?
ควรเจาะในคนไข้รายไหน ?
ต้องงดอาหารก่อนเจาะหรือไม่ ?
วิธีลด Lp(a) มีอะไรบ้าง ?
เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
📷 ApoB
คืออะไร ?
มีความสำคัญอย่างไร ?
ควรเจาะในคนไข้รายไหน ?
__________________________________________
📷 อายุ 30-79 + LDL 70-189 without ASCVD
__________________________________________
📷 ประเมิน ASCVD risk ก่อนนะครับ !!
โดยใช้ "PREVENT-ASCVD equations" !!
📷 Low 10-y risk (<3%)
📷 LDL 160-189 or 30-y ASCVD risk ≥10% (สำหรับคนอายุ 30–59 y)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 LDL <160 and 30-y ASCVD risk <10%
📷 health behavior counseling (class 1)
📷 Borderline 10-y risk (3% to <5%)
📷 moderate-intensity statin (class 2a)
(goal = LDL <100 + ลดลง ≥30% + non-HDL C <130)
📷 ควรประเมิน Risk enhancer (ดูจากตารางด้านล่าง) ประกอบการพิจารณาให้ statin ด้วย
(class 2a)
📷 if high-sensitivity C-reactive protein (hsCRP) ≥2 mg/L on 2 successive occasions โดยไม่มีสาเหตุ
--> ให้ high-intensity statin (class 2a)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (coronary artery calcium) โดยใช้ non-contrast-gated cardiac CT (class 1) (โดยทั่วไปแนะนำให้ทำในชายอายุ ≥40 และ หญิงอายุ ≥45)
📷 if CAC >0 --> ให้ statin (class 1)
📷 if CAC =0 --> health behavior counseling
+ repeat CAC 3-7 y (class 1)
📷 Intermediate 10-y risk (5% to <10%)
📷 moderate-high intensity statin (class 1)
(goal = LDL <100 + ลดลง ≥30% to ≥50% + non-HDL C <130) (class 2a)
(ถ้าคนไข้อยู่ใน higher end of this risk range แนะนำให้ใช้ high intensity statin เพื่อลด LDL ≥50%)
📷 ถ้ายังตัดสินใจไม่ได้เรื่องการให้ statin
ให้ประเมิน CAC testing (class 1)
📷 พิจารณาให้ statin จาก CAC ในเกณฑ์เดียวกับกรณี borderline 10-y risk ข้างต้น
📷 High 10-y risk (≥10%)
📷 high intensity statin (class 1)
(goal = LDL <70 + ลดลง ≥50% + non-HDL C <100) (class 2a)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe (class 2a)
📷 add PCSK9 mAb or Bempedoic acid
(with or without ezetimibe) (class 2b)
📷 Special consideration
📷 if life expectancy <1 y
📷 อาจพิจารณาหยุดยาลดไขมัน (class 2b)
📷 คนไข้ที่มี baseline untreated LDL <70 และ
non–HDL-C <100 without additional ASCVD
risk factors
📷 ไม่ต้องให้ยา statin (class 3 ; No benefit)
__________________________________________
📷 Calcium score (CAC score)
(Coronary artery calcium score)
นำมาพิจารณาให้ Statin อย่างไร ?
__________________________________________
📷 Calcium score (CAC score)
ควรตรวจในคนไข้รายไหน ?
📷 Men ≥40 or Women ≥45 Years ที่ประเมินความเสี่ยงโดยใช้ PREVENT-ASCVD equations แล้วตกอยู่ในกลุ่ม Intermediate 10-y risk (5% to <10%) หรือ Borderline 10-y risk (3% to <5%) และยังตัดสินใจไม่ได้แน่ชัดว่าควรให้ยา statin หรือไม่
📷 CAC score ตรวจและแปลผลอย่างไร ?
📷 ตรวจโดยใช้ non-contrast-gated cardiac CT
📷 แปลผล
📷 CAC score แสดงถึง overall amount of calcified coronary plaque ซึ่งบ่งบอกถึงการมี subclinical atherosclerosis โดยที่ CAC score ยิ่งสูง ก็จะพยากรณ์ได้ว่าคนไข้ยิ่งมีโอกาสสูงที่จะเกิด MACE (major adverse CV event) ในอนาคต และความสัมพันธ์ระหว่าง CAC score กับการเกิด MACE นี้พบว่าเป็นไปในแบบที่แทบจะเป็น linear relationship เลยทีเดียวครับ
📷 CAC score แบ่งระดับความรุนแรงได้ดังนี้
📷 absent (0 AU)
📷 minimal (1-9 AU)
📷 mild (10-99 AU)
📷 moderate (100-299 AU)
📷 severe (300-999 AU)
📷 extensive (≥1000 AU)
📷 CAC score นำมาพิจารณาให้ Statin อย่างไร ?
📷 CAC score 1-99 AU and <75th standardized percentile for age, sex & race
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 CAC score 100-299 AU or ≥75th standardized percentile for age, sex & race
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1)
📷 CAC score 300-999 AU (severe)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 Goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
(โดยใช้วิธีเพิ่ม intensity of statin หรือ add ezetimibe, PCSK9 mAb, or bempedoic
acid) (class 2a)
📷 CAC score ≥1000 AU (extensive)
📷 ให้เริ่มยาลดไขมัน (statin เป็น first-line Rx)
(class 1)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 incidental finding of mild CAC on noncardiac CT scan
📷 moderate intensity statin (class 2a)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 2a)
📷 moderate-to-severe incidental coronary atherosclerosis identified on noncardiac CT scans (eg, by visual estimation or a validated artificial intelligence-based algorithm)
📷 moderate-high intensity statin (class 2a)
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a)
📷 คนไข้ที่มี LDL ต่ำกว่า targets สำหรับแต่ละ CAC levels อยู่แล้วโดยที่ไม่ได้ on statin
📷 ก็ยังแนะนำให้ใช้ยาเพื่อลด LDL ลง ≥30% ด้วยนะครับ
📷 CCTA (coronary CT angiography)
พิจารณาทำในรายไหน ?
📷 อาจพิจารณาทำ CCTA (coronary CT angiography) ในคนไข้ที่ไม่เคยมี ASCVD แต่ likely ที่จะมี high burden of "noncalcified" plaque (eg, inflammatory disorders, HIV, and diabetes) เพื่อช่วยตัดสินใจในการให้ statin (class 2b)
__________________________________________
📷 Severe hypercholesterolemia : LDL ≥190
__________________________________________
📷 without clinical ASCVD, additional ASCVD risk factors, HeFH, or subclinical atherosclerosis
📷 maximally tolerated statin (class 1)
(goal = LDL <100 + non-HDL C <130)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or
bempedoic acid (class 1)
📷 add inclisiran (as alternative to PCSK9 mAb) with or without ezetimibe (class 2a)
(ณ ชั่วโมงนี้ inclisiran ยังถือเป็น second-line PCSK9i โดยยังได้ข้อบ่งชี้เพียงแค่ใช้ลด LDL เท่านั้น เนื่องจากยังต้องรอดู CV benefit จาก CV outcome trials อยู่ครับ)
📷 without clinical ASCVD but with HeFH, additional ASCVD risk factors, or subclinical atherosclerosis (documented coronary calcification)
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <70 + non-HDL C <100
📷 with clinical ASCVD
📷 รักษาเหมือนข้อ 1 แต่ขยับ goal = LDL <55 + non-HDL C <85 + optional apoB goal <55
__________________________________________
📷 DM without established ASCVD
__________________________________________
📷 อายุ 20-39
📷 moderate-intensity statin ใน 2 กรณี
📷อายุ ≥30 + PREVENT ASCVD 10-y risk ≥3% หรือ 30-y risk ≥10% (class 2a)
📷 มี Diabetes-specific risk enhancer
(DM of long duration [≥10 y of T2DM, ≥20 y of T1DM], albuminuria (≥30 μg of albumin/
mg cr), eGFR <60, retinopathy, neuropathy, or ABI <0.9) (class 2b)
📷 อายุ 40-75
📷 moderate-intensity statin (class 1)
📷 Goal = LDL <100 + ลดลง ≥30-49% + non-HDL C <130 (class 1) + optional apoB goal <90
📷 high intensity statin (class 2a)
if PREVENT ASCVD 10-y risk ≥10% or multiple ASCVD risk factors
📷 Goal = LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 2a) + optional apoB goal <70
📷 add ezetimibe or PCSK9 mAb (class 2b)
if not achieved LDL & non-HDL C goal
📷 add IPE (after a statin) (class 2b)
if additional ASCVD risk factor(s) + LDL<100 + fasting TG 150–499
หมายเหตุ
Additional ASCVD risk factor(s) ในกรณีนี้
ดูจาก REDUCE-IT inclusion criteria ได้แก่
men ≥55 y, women ≥65 y, cigarette smoking or stopped smoking within 3 mo, HT (SBP ≥140 or DBP ≥90 or ใช้ยา HT อยู่), HDL ≤40 for men or ≤50 for women, hs-CRP >3.0 mg/L, CrCl >30 and <60, retinopathy, albuminuria (≥30 μg of albumin/mg Cr), ABI <0.9
📷 อายุ >75 + estimated life expectancy≥2.5y
📷 moderate-intensity statin (class 2b)
📷 ถ้ามี statin-attributed side effects
📷 initiation of ezetimibe and/or bempedoic acid or a PCSK9 mAb (class 1)
__________________________________________
📷 Secondary ASCVD Prevention
__________________________________________
📷 Clinical ASCVD "Not at Very High Risk"
(ดู criteria สำหรับ Very High Risk จากรูปด้านล่างนะครับ)
📷 goal
📷 LDL <70 + ลดลง ≥50% + non-HDL C <100 (class 1) + optional apoB goal <70
📷 optional goal : LDL <55 + non-HDL C <85 (class 2a) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe, PCSK9 mAb and/or bempedoic acid (class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 Clinical ASCVD "at Very High Risk"
(include ASCVD with CKD)
📷 goal : LDL <55 + ลดลง ≥50% + non-HDL C <85 (class 1) + optional apoB goal <55
📷 ยา
📷 high intensity statin (class 1)
📷 if not achieved LDL & non-HDL C goal
📷 add ezetimibe and/or PCSK9 mAb
(class 1)
📷 add bempedoic acid, with or
without ezetimibe and/or PCSK9 mAb
(class 2a)
📷 inclisiran (with or without ezetimibe)
ใช้แทน PCSK9 mAb เมื่อไม่สามารถใช้ PCSK9 mAb ได้ หรือมี strong preference for less frequent dosing (class 2a)
📷 HFrEF Due to ASCVD (IHD) + มี reasonable life expectancy (3–5 y) + not already on a statin
📷 อาจพิจารณาเริ่มให้ moderate-intensity statin เพื่อลด ASCVD events (class 2b)
📷 HFrEF ที่ไม่มี ASCVD + ไม่มีข้อบ่งชี้อื่นของ statin --> ไม่แนะนำให้ statin (class 3 ; No benefit)
__________________________________________
📷 CKD stage 3 or higher
__________________________________________
📷 CKD stage 3 or higher + อายุ 40-75
+ LDL 70-189
📷 แนะนำให้ moderate-intensity statin or moderate-intensity statin + ezetimibe เพื่อลด ASCVD risk (class 1)
📷 CKD stage 3 or higher + clinical ASCVD
📷 แนะนำให้ high-intensity statin with or without ezetimibe and/or a PCSK9 mAb
(goal : LDL <55 + ลดลง ≥50% + non-HDL C <85) (class 1)
📷 CKD ที่ require maintenance hemodialysis
📷 อาจพิจารณา continue statin เพื่อลด risk of ASCVD events โดยพิจารณาจากหลายๆปัจจัย เช่น expected survival, other comorbidities, and severity of ASCVD (class 2b)
__________________________________________
📷 คนไข้ HIV
__________________________________________
📷 คนไข้ HIV อายุ 40-75
📷 แนะนำให้ statin เพื่อลด risk of a first
ASCVD event และลด rate of coronary
atherosclerosis progression (class 1)
__________________________________________
📷 คนไข้ cancer
__________________________________________
📷 if life expectancy ≥ 2 y ให้พิจารณาใช้ statin ได้ตามข้อบ่งชี้เหมือนคนไข้ที่ไม่ได้เป็นมะเร็ง
📷 อาจพิจารณาเริ่มให้ statin เพื่อ prevent anthracycline-induced cardiotoxicity
(class 2b)
__________________________________________
📷 ยาลดไขมัน
ชนิด, Dose, รายละเอียดของยาแต่ละตัว
ดูจากตารางด้านล่าง
__________________________________________
__________________________________________
📷 Lp(a)
__________________________________________
📷 Lp(a) คืออะไร ?
📷 คือ LDL-like particle ที่มี structure แตกต่างไปจาก LDL โดยจะ carries a single apoprotein(a) strand bound to its apoB-100 component
📷 Lp(a) มีอันตรายอย่างไร ?
📷 Lp(a) เป็น genetic risk factor ในการเกิด ASCVD ครับ (independent of LDL and other risk factors)
📷 ระดับของ Lp(a) ที่สูงจะสัมพันธ์กับการเกิด ASCVD อย่างชัดเจน โดยผ่านกลไกหลายๆอย่าง เช่น proatherogenic and proinflammatory effects ซึ่งส่วนหนึ่งก็ถูกกระตุ้นจาก oxidized phospholipids on Lp(a) นั่นเอง
📷 เจาะแล้วมีประโยชน์อย่างไร ?
📷 เจาะเพื่อ identify คนไข้ที่ increased ASCVD risk (independent of LDL and other risk factors)
📷 ควรเจาะในคนไข้รายไหน ?
📷 in all adults !! ควรเจาะอย่างน้อย 1 ครั้งในชีวิตครับ (class 1)
(ระดับของ Lp(a) จะไม่ค่อยเปลี่ยนแปลงตามกาลเวลา และไม่ค่อยเปลี่ยนแปลงตาม lifestyle factors ด้วยครับ เนื่องจากเป็นปัจจัยทาง genetic ยกเว้น ช่วง menopause transition อาจจะมีค่าเปลี่ยนแปลงได้บ้าง หรือมี secondary cause of elevated Lp(a) เช่น kidney, liver, thyroid disease, pregnancy, certain medications)
📷 เจาะใน first-degree family members ของคนไข้ที่เป็น FH, premature ASCVD, or
high Lp(a) (class 1)
📷 ต้องงดอาหารก่อนเจาะหรือไม่ ?
📷 ไม่ต้อง fasting เลยครับ !!
📷 วิธีลด Lp(a) มีอะไรบ้าง ?
📷 PCSK9i (mAbs and small-interfering
RNA)
--> ลด Lp(a) ได้ ∼15-30%
(ณ ชั่วโมงนี้ PCSK9i ยังไม่ได้รับ FDA-approved for Lp(a) lowering นะครับ แต่ก็เริ่มมีข้อมูลสนับสนุนมากขึ้นเรื่อยๆในแง่ของ clinical outcome)
📷 Specific Lp(a)-lowering therapies
(ลด Lp(a) production ได้แก่ mRNA therapies or oral small-molecule inhibitors)
--> กำลังมีการศึกษาใน randomized clinical outcomes trials อดใจรออีกซักหน่อยนะครับ !!
📷 lipoprotein-apheresis
📷 Lifestyle management
-->ไม่ค่อยมีผลต่อระดับ Lp(a) ครับ เพราะเป็นปัจจัยทาง genetic
📷 statin
--> ไม่มีผลลดระดับ Lp(a) และอาจเพิ่มระดับ Lp(a) เล็กน้อยด้วยซ้ำ โดยเฉลี่ยแล้วจะเพิ่ม ~1.1 mg/dL แต่ก็ถือว่าไม่จำเป็นต้องหยุดใช้ statin นะครับ เนื่องจากมี strong benefit ในการ prevent ASCVD
📷 เจาะแล้วพบว่า Lp(a) สูง ทำอย่างไร ?
(Lp(a) ≥50 mg/dL จึงจะถือว่าสูงนะครับ โดยพบได้ ~20% ของประชากร)
📷 คนไข้ที่ยังไม่มี ASCVD
📷 แนะนำให้รีบ optimal early control of modifiable CV risk factors โดยการคุม BP, BS, lipid ให้ดีที่สุด รวมถึงการพิจารณาเริ่มให้หรือ intensified statin เพื่อลด LDL และลด ASCVD risk (class 1)
📷 คนไข้ที่มี clinical ASCVD + elevated Lp(a) + ได้ maximally tolerated statin แล้วยังไม่ achieved LDL and non–HDL goals
📷 ให้ add PCSK9 mAb (class 1)
เพื่อให้ achieved LDL, non–HDL, ApoB goal +
potential additional benefit of moderate Lp(a) lowering
📷 คนไข้ที่ Lp(a) ≥60 mg/dL + FH + (CAD or PAD)
📷 ให้ทำ lipoprotein-apheresis (FDA-approved based on observational data)
__________________________________________
📷 ApoB
__________________________________________
📷 ApoB คืออะไร ?
📷 ApoB เป็นการวัด atherogenic particle number โดยตรง ซึ่งจะมีจำนวน 1 molecule per LDL, VLDL and Lp(a) particle ซึ่งแตกต่างจากตัวเลข LDL ที่จะ reflects ถึง cholesterol mass ที่อยู่ภายใน LDL particles มากกว่าที่จะ reflects ถึง number of atherogenic lipoproteins
(แต่ LDL ยังคงเป็น traditional lipid marker for ASCVD risk assessment and treatment targets อยู่นะครับ)
📷 ApoB มีความสำคัญอย่างไร ?
📷 ApoB สามารถ predicts ASCVD risk ได้
accurate กว่า LDL ใน setting คนไข้ที่มี
discordance กันระหว่างตัวเลข LDL และ ApoB เช่น LDL อยู่ใน target ดีแล้ว แต่ ApoB ยังสูงเกิน goal ซึ่งจะถือว่าคนไข้จะยังมี persistent atherogenic particle burden (ยังมี residual CVD risk in statin-treated populations)
ที่จำเป็นต้องปรับยาเพิ่มต่อครับ โดย pattern แบบนี้มักพบในกลุ่มคนไข้ cardiometabolic disease, including ASCVD, CKM syndrome, diabetes, and/or TG ≥150 mg/dL ซึ่งในกรณีแบบนี้เราจะถือว่า ApoB เป็น more reliable marker for ASCVD risk and therapeutic guidance ครับ
📷 ApoB ยังสัมพันธ์กับการเกิด CV events independent of LDL ด้วยครับ
📷 ตัวเลข ApoB จึงสามารถใช้เป็นได้ทั้ง target ในการใช้ยารักษา และใช้เป็นตัวบอก ASCVD risk ได้ด้วย
📷 ควรเจาะในคนไข้รายไหน ?
📷 คนไข้ที่ใช้ยาลดไขมันอยู่แล้ว โดยเฉพาะคนไข้ที่เป็น ASCVD, CKM syndrome, type 2 diabetes, and/or elevated TG ที่ achieved LDL and/or non–HDL-C goals แล้ว ควรเจาะ ApoB ดูเพื่อช่วยตัดสินใจว่าจะต้องปรับยาเพิ่มต่ออีกหรือไม่ (class 2a)
📷 คนไข้ที่ยังไม่ได้ใช้ยาลดไขมัน อาจพิจารณาเจาะ ApoB เพื่อช่วย enhance ASCVD risk assessment และช่วยตัดสินใจในการเริ่มให้ยา และช่วย characterize inherited lipid disorders (class 2b)
__________________________________________
Reference
📷 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/
AGS/APhA/ASPC/NLA/PCNA Guideline on
the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
13 มี.ค.2026
#dyslipidemia #accahaguideline #ไขมันในเลือดสูง](https://pbs.twimg.com/media/HFrRKQcaIAA-4sX.jpg)



















