A middle aged woman presented with late RCA STEMI had one of the most catastrophic mechanical complications, Ventricular septal rupture. Choosing an appropriate mechanical circulatory support for these pts is imperative.
Amyloid fibrils deposits in perimysial blood vessels and within endo- and perimysial connective tissue of skeletal muscle.
Has a feature of “pseudohypertrophy” in biceps muscle in this wATTR cardiac amyloidosis pt.
** consent obtained from my patient **
PMID: 34175153
Caveats:
- Retrospective work, meaning risking residual confounding
- Treatment heterogeneity: No standardized protocol for meds/tMCS
- Needs a real-time clinical utility for validation (i.e., prospective, protocol-driven studies)
Work led by @NavinKapur4 👏🏽
Combining machine learning (ML)-based phenotypes (I–III) with SCAI stages (A–E) improves serial risk stratification in patients with cardiogenic shock when assessed at 6-hour intervals over a 72-hour period.
I'll highlight some key findings and some caveats in this work ..
Key findings:
- Most changes of phenotypes occur within first 6 hr (i.e., SCAI-B pt can die in 6 hours)!
- Aim for “Golden Day of Shock” to established meds/ tMCS to reverse the course
- Adding ML phenotypes to SCAI stages improves risk stratification >> mortality differences
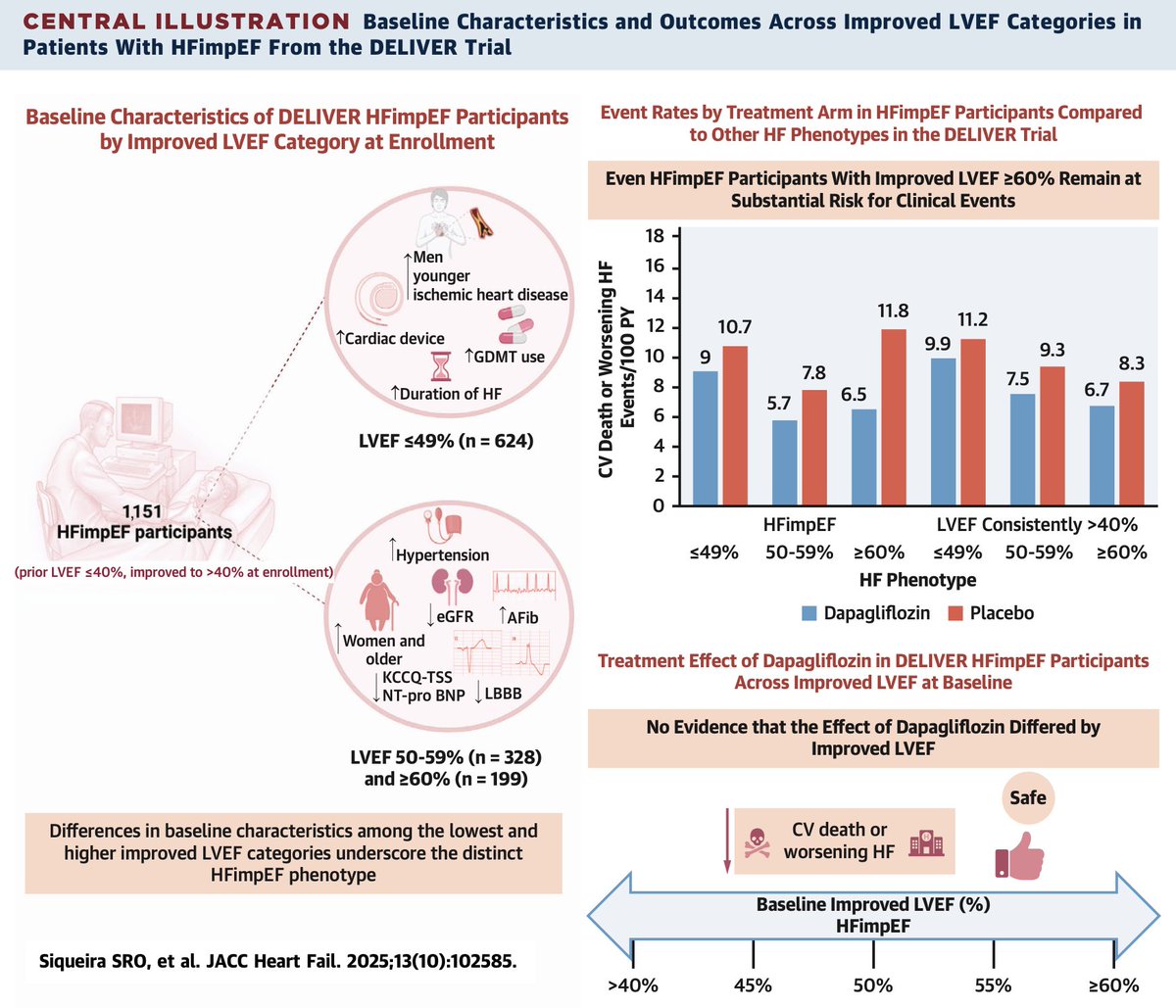
Lessons learned from DELIVER Trial:
- Dapa ↓ CV events/mortaltiy in all HFimpEF subgroups
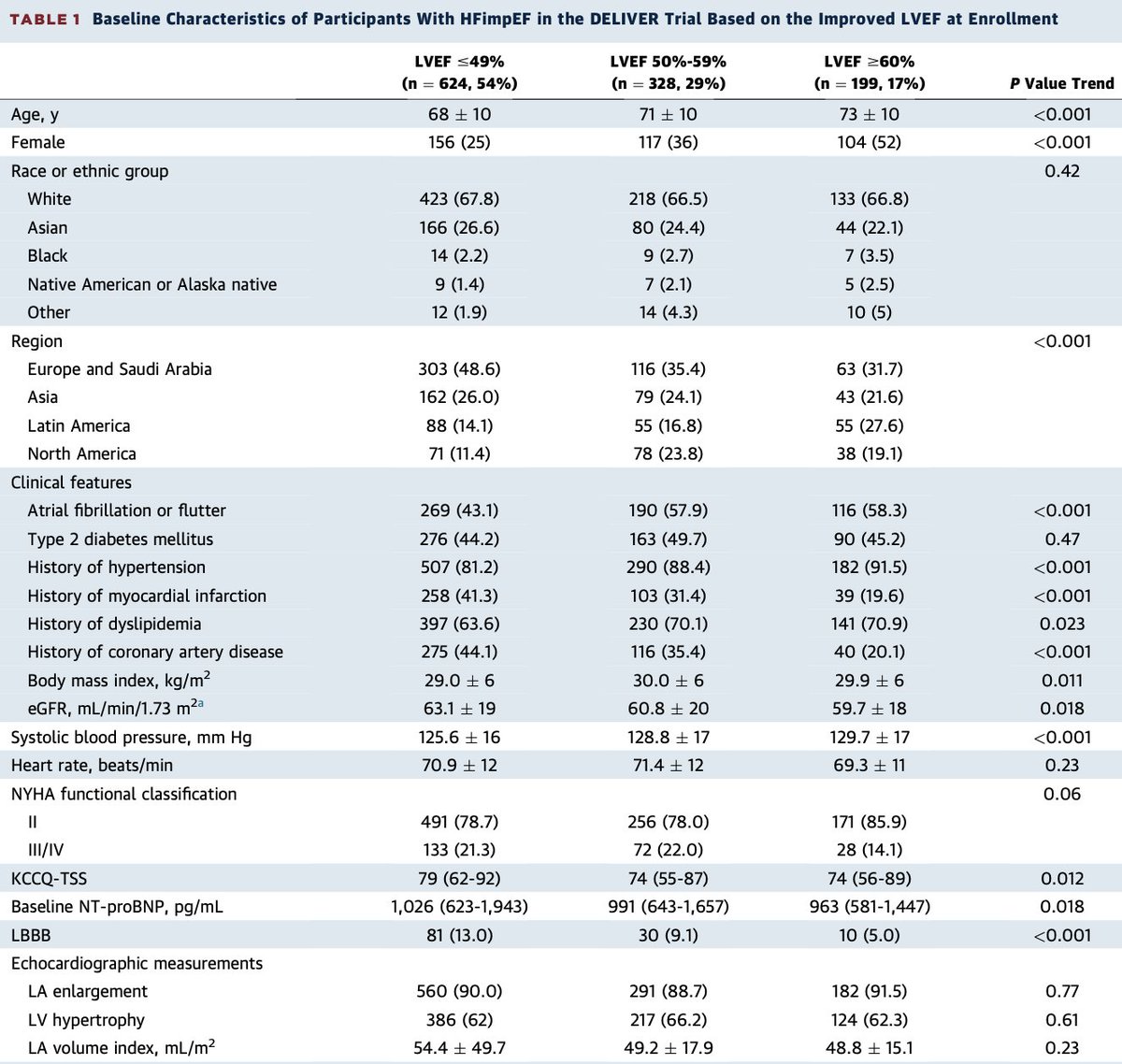
- Patients with HFimpEF (EF ≥50%) were more ♀/older/less GDMT
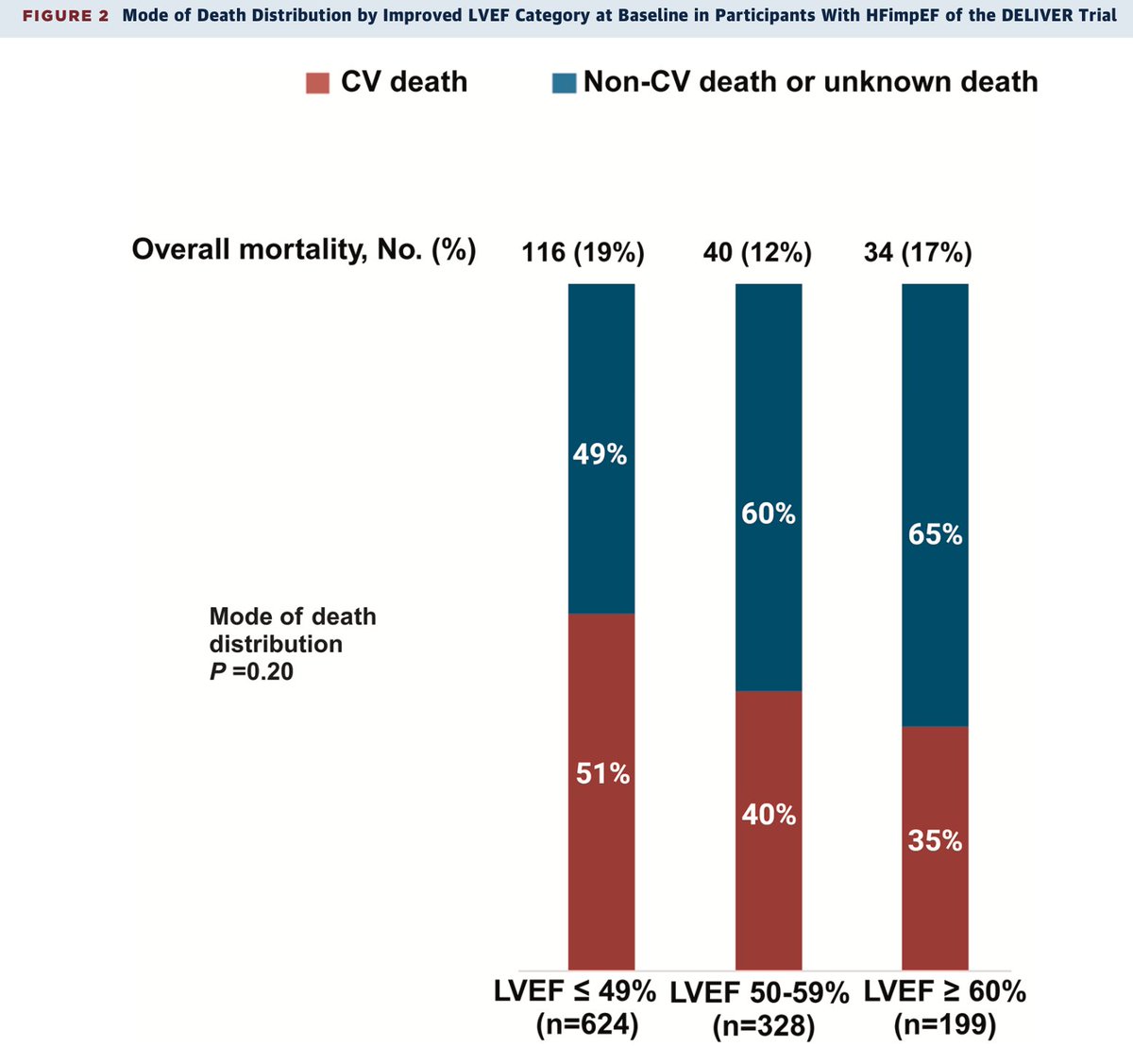
- The ↓ EF, the ↑ CV Death (NS)
- Regional enrollment differed by LVEF could represent specific geographical variables
Among pts w CardioMEMS, either:
- PA Diastolic ≤20 mmHg
- ↑PAD then ↓ to ≤20 mmHg in 90d
experienced better survival in 2yrs
Caveats:
- Although large (~ 10K pts), but still observational
- In RCTs CardioMEMS have not shown a statically significant ↓ in overall mortality
Semaglutide treat frailty in Obese+HFpEF?
Caveats:
1. Used Frailty Index (FI), i.e., overestimates frailty + no incorporation of physical frailty domains
2. 2ndr analysis (STEP-HFpEF) > not adequately powered for clinical events
3. No measures of body composition + adiposity
The "balanced distribution" between🤍/🫘 + selective strong antagonism against aldosterone + lack of active metabolite with short half life are the recipe for potential benefits of finerenone (@Bayer) in HF across the board.
"Let's do IVC check to guide diuretics therapy"
#RIP
Per CAVA-ADHF-DZHK10, > 300 pts were RCTs to IVC check + clinical assessment vs. clinical assessment alone. Additional U/S evaluation of IVC did not improve decongestion treatment compared with clinical assessment alone.
A step forward to precision medicine.
Grant et al. used data from the ARIC study (>15K pt) to evaluate how clinical, lab, and echo factors within the PREVENT-HF model relate to preclinical HF and to determine whether these factors improve HF risk prediction.
#CardioX
AMR remains one of the most devastating outcomes post OHTx, yet the evidence on Dx/Rx has a huge gap. This position statement emphasizes the current understanding and outlining priorities for future research to improve patient outcomes.
#CardioX
In the extended 13.2-yrs f/u of DANISH trial, ICD in NICMP HFrEF did not ↓ overall mortality but did ↓ SCD [HR: 0.54; 95% CI: 0.36-0.80] in younger pts. Should continue to shy away from ICD in NICMP > 70 yrs?
#CardioX Ref: https://t.co/taRijVEH9C
















![AzizJoury's tweet photo. In the extended 13.2-yrs f/u of DANISH trial, ICD in NICMP HFrEF did not ↓ overall mortality but did ↓ SCD [HR: 0.54; 95% CI: 0.36-0.80] in younger pts. Should continue to shy away from ICD in NICMP > 70 yrs?
#CardioX Ref: https://t.co/taRijVEH9C https://t.co/ijGtNm4qMc](https://pbs.twimg.com/media/G3994EXXYAAt0PJ.jpg)





















![AzizJoury's tweet photo. In the extended 13.2-yrs f/u of DANISH trial, ICD in NICMP HFrEF did not ↓ overall mortality but did ↓ SCD [HR: 0.54; 95% CI: 0.36-0.80] in younger pts. Should continue to shy away from ICD in NICMP > 70 yrs?
#CardioX Ref: https://t.co/taRijVEH9C https://t.co/ijGtNm4qMc](https://pbs.twimg.com/media/G3994EYW4AAEeEr.jpg)





























