After years of working in thoracic anaesthesia, there comes a moment when you realise the gap between what you were taught and what you actually need to know.
For me, that gap was in One Lung Ventilation.
It's one of the most technically demanding parts of our practice, yet for a long time, dedicated teaching just wasn't there. So I made it my mission to change that.
l've spent years teaching and building resources for anaesthetists, ODPs and cardiothoracic teams at all stages of their careers to pave the way for confident, well-prepared clinicians. Because when the teaching is right, better outcomes follow.
That's why I built the FREE ONE-LUNG UK tutorial series.
You can already watch the teaser videos now on https://t.co/k07z3QmzGj https://t.co/YiUmc16g8f
The full chapters drop this Thursday.
And if you want hands-on experience, join us for the live ONE-LUNG UK course on 29th May at Guy's Hospital.
More info
& https://t.co/6yCzcTFWnw
#OneLungVentilation @GSTTanaesthesia
Cancer used to be a death sentence.
Now many are >90% survivable.
Childhood leukemia: 5% → 92%
HER2+ breast: 25% → 90%
CML: 22% → 87%
This is not "luck".
Its decades of funding towards time & infra that compounds discovery.
Pancreatic cancer today is the breast cancer of 1985, and Glioblastoma ≈ leukemia of 1970.
The scientists who will solve them
are already in labs NOW.
The question is whether we fund them long enough.
Funding doesn’t just support science.
It literally rewrites outcomes.
This plot is proof.
Source: SEER + NIH via @Jori_health
🏃♂️🫀 Exercise Prescriptions Should Be Risk-Stratified — Not Generic
Current guidelines recommend ≥150 min/week of moderate-to-vigorous physical activity (MVPA) for everyone.
But is that optimal for a 45-year-old low-risk individual and a 70-year-old very high-risk patient?
This large UK Biobank cohort (72,884 participants, median 13.2-year follow-up) provides a more nuanced answer .
🔬 What’s innovative?
• Objective 7-day wrist accelerometer data
• ESC-aligned SCORE2 risk stratification
• Isotemporal substitution modeling (reallocating sedentary time)
• Identification of optimal vigorous activity thresholds by risk group
📊 Key findings
Each +150 min/week MVPA →
• 20% lower CVD risk in very high-risk individuals
• 16% reduction in high- and low-to-moderate-risk groups
Higher-risk individuals benefit the most from increasing activity.
BUT intensity matters.
When replacing 300 min/week sedentary time:
🔹 Low-to-moderate risk → Any mix of moderate (MPA) and vigorous (VPA) works. More VPA = more benefit.
🔹 High risk → VPA should be ≤60 min/week (~20% of MVPA).
🔹 Very high risk → Optimal VPA ≈ 42 min/week (~14% of MVPA). Beyond that, benefits decline.
In high-risk groups, excessive VPA may attenuate benefit—likely due to hemodynamic stress, endothelial dysfunction, and oxidative burden.
🎯 Take-Home Messages
1️⃣ Physical activity remains powerfully protective across all risk strata.
2️⃣ Higher-risk patients gain the largest relative benefit.
3️⃣ Vigorous exercise has a ceiling effect in high-risk individuals.
4️⃣ Exercise prescriptions should integrate formal risk stratification (e.g., SCORE2).
Precision prevention now extends to lifestyle medicine.
One size does not fit all.
@Paul_Wischmeyer Hypertensive encephalopathy probably. IV Clonidine +IV Metoprolol . Aim to lower SBP to 160, Check history for amphetamines, cocaine. Check for papilledema.
1/6
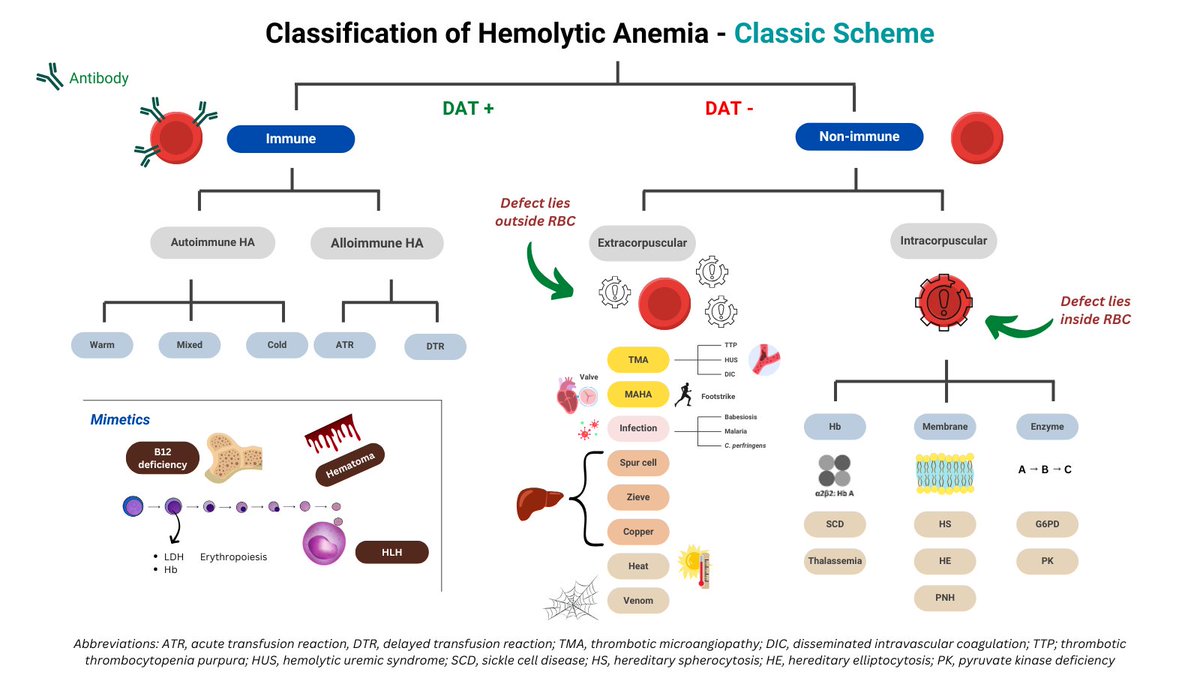
RETHINKING HEMOLYSIS CLASSIFICATION
I recently saw an incredibly rare but fascinating case of T-cell large granular lymphocytic (T-LGL)–mediated, DAT-negative hemolysis.
It prompted me to rethink how we classify hemolytic anemia and revise the schematic accordingly.