Head of Macro
L/S Hedge Fund. Blue Duck Capital, LLC is soliciting no action or endorsement based upon tweets, retweets, likes. Do your own due diligence.
The sell side analysis of the implications of the Hikma ruling for $LQDA misses the mark.
Sell side is calling it bullish but calling it bullish for the wrong reasons - e.g. that it takes away the possibility of a drug removal. While that may be true, that is not the important read through.
Hikma is bullish because it has a direct bearing on the dependent claims analysis. Everyone has been focused on Claims 1 and 14, and ignored the dependent claims.
The dependent claims are murky and Andrews was always troubled by them. He could use Bayer to say that they don't have patentable weight, and are therefore not valid but the cleaner arrow was always going to be Hikma - which if it got over turned would allow him to say that there is no induced infringement either.
This Hikma ruling in effect says that if it is not on the label, then it is not the company's problem. The capabilities outlined in the dependent claims are not in $LQDA's label ergo it is impossible per Hikma for $LQDA to infringe those claims.
That new precedent knocks out every dependent claim very cleanly now.
The timeline of this case as much as it vexed folks makes more sense now.
Andrews hears the case in June and recognizes both that a launch is underway and he might have to rule against the party launching - which is why he asks for expedited briefing and speaks to the mess it would be if he finds against $LQDA.
After the initial briefing, he sees that he has a route to find for $LQDA on Claim 14 and Claim 1, which is the case, but he still has these outstanding dependent claims.
That fall, the solicitor general asks that the SC take up Hikma (this being Andrew's prior case and one that $UTHR cited in their brief is likely one he is following). He knows that if the SC takes it up and reverses the Federal Circuit court, he has a clean shot on the murkier dependent claims and a much more thorough opinion. He also knows that his ruling at this point is not going to affect the commercial realities and equities and so he is not rushed. Might as well wait for this ruling to come out. So he takes his time and now we finally have this ruling and so he has all the pieces he needs.
You should. I think, if you see this in the context of Bayer. Would make sense that he would wait for Hikma.
Fed. Cir's language on Bayer was very vague and if that got overturned by SCOTUS ruling *for* Amarin, then that would've been a different mess.
On the other hand if SCOTUS elaborated and provided a backstop upholding Fed. Cir in Bayer, that would lead to a different outcome & this is what happened today.
You should. I think, if you see this in the context of Bayer. Would make sense that he would wait for Hikma.
Fed. Cir's language on Bayer was very vague and if that got overturned by SCOTUS ruling *for* Amarin, then that would've been a different mess.
On the other hand if SCOTUS elaborated and provided a backstop upholding Fed. Cir in Bayer, that would lead to a different outcome & this is what happened today.
Overheard someone saying Hikma is good but $LQDA still needs to prove obviousness.
DTX3 - On UTHR's May 2018 earnings call, Martine said, in response to a question about using Tyvaso for PH-ILD, that she was aware Dr. Waxman and other doctors used Tyvaso off-label to treat PH-ILD patients, and they told $UTHR that "this drug works" — even better in Group 3 PH (PH-ILD) than in PAH, specifically in improving exercise capacity.
This compounds actually. UTHR's own NEJM paper (the INCREASE publication) identifies Faria-Urbina and Agarwal as "pilot studies" that provided a reasonable expectation of success to run INCREASE.
UTHR's start witness also testified no company runs a Phase 3 trial like INCREASE without proof-of-concept pilot studies. So UTHR's own witness and own documents establish that the prior art gave both motivation and a reasonable expectation. Liquidia's opening brief opens with exactly this btw: "This drug works." — UTHR's CEO, 2018.
Thank you Dr. Rothblatt & Dr. Nathan for your service.
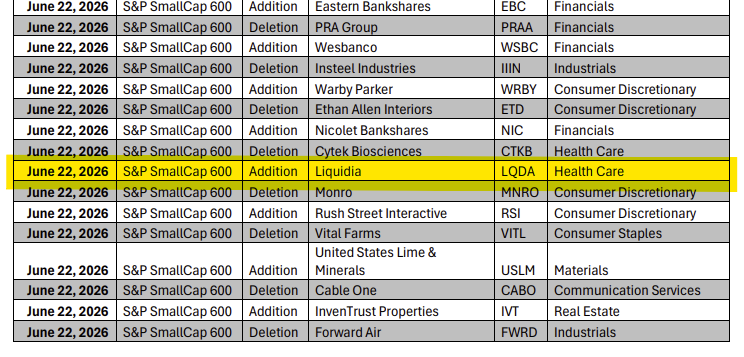
$LQDA Hikma wins SCOTUS trial. Andrews now has what he needs to end this long and painful 327 cloud over our heads.
I expect Andrews to move fast just like when PTAB killed 793.
After listening to $LQDA Jefferies conference today, I'm not selling a single share under $100. Will wait for Q2 to confirm script growth rate.
'327 doesn't concern me. Andrews is waiting on Hikma which will be decided by June 30th. Expecting Andrews opinion in July. Q2 in August and new trial details in Q3.
RJ hinted at partnership interests. Too much upside. His bar is probably $15B for someone like Merck.
$5 in EPS on $1B in sales.
Exciting turnaround underway at $AIRS. Think this new management team has really got things cooking.
We are long the stock but may sell at any time. We may not share future positioning. This is not advice, we could be wrong, and please do your own research to arrive at your own conclusions.
Ph2 was more of a proof of concept. Ph3 would be confirmation in larger pop. Ph3 also expands eligibility from Stage IIIB-IV to Stage IIB-IV, which broadens the potential commercial label but adds lower risk patients where treatment effect tends to be smaller.
INT could theoretically prevent ctDNA- patients from converting to ctDNA+ over time. But the published analysis uses baseline ctDNA status only, so the trial doesn't actually answer this question.
KEYNOTE-942 didn't pre-specify conversion as an endpoint. INTerpath-001 is collecting serial ctDNA, so we might get an answer in the Phase 3 readout if they report it.
The trial hasn't shown a statistically significant survival benefit fyi. OS HR is 0.471 but the 95% CI is 0.165-1.345 based on only 14 deaths total (7 vs 7). The point estimate favors INT, but the data is statistically consistent with everything from major mortality benefit to a 34% increase in mortality.
The paper itself characterizes this as "favorable trend in overall survival" & not "demonstrated survival benefit." Which is an important distinction, especially since most cancer drugs that look favorable on RFS but don't show OS separation eventually run into payer pushback.
Even if Ph3 confirms RFS benefit, without a clear OS signal and without ctDNA+ subgroup evidence, the drug faces an uphill battle with NCCN Category 1 designation and payer coverage at it's cost.
$MRNA shareholders really need to be asking questions here. From yesterday's ASCO paper.
"Treatment-related adverse events occurred in 104/104 patients (100%) in the intismeran plus pembrolizumab arm and 42/50 (84%) in the pembrolizumab arm"
Every single patient on combo had a treatment-related AE.
"Direct functional linkage between post-treatment T-cell clonotypes and specific intismeran-encoded neoantigens remains to be established."
5-yr OS: HR 0.471, CI 0.165-1.345. So INT reducing death risk by 84% is as equally true as INT increasing death risk by 34%.
Among the myriad of imbalances in the trial, the ctDNA imbalance is particularly telling.
Combo: 13 ctDNA+ (12.1%). Pembro: 2 ctDNA+ (4.0%).
With only TWO ctDNA-positive patients in the entire control arm, the ctDNA-positive subgroup HR is mathematically "not estimable."
So the highest risk subgroup, the patients who biologically need adjuvant therapy most, cannot be analyzed against a control. After 5 years and three publications, we still don't know if INT works in patients with detectable residual disease.
The pembro arm has 30% "not evaluable" ctDNA vs 16.8% in combo. 13 percentage points of unknown ctDNA status in the control arm.
In an expensive Phase 2 trial run by two of the largest pharma companies in the world, you would expect cleaner biomarker characterization.
Is this simply a coincidence? You be the judge of that.
@HowieDennison Mechanistically, sure. Still doesn't change the broader argument. 14-death OS, ctDNA+ subgroup non-estimable, n=2 in pembro control, 30% vs 16.8% NE asymmetry, mechanism unproven.
List goes on.
Yes, thanks for engaging. The statistical claim that KEYNOTE-942 cannot reliably estimate efficacy in ctDNA+ patients is established.
My forecast is informed by the math (working backwards from overall HR 0.51 and published ctDNA-negative HR 0.21 suggests ctDNA+ HR likely 1.0-1.3), the biology (ctDNA+ patients have higher tumor burden and more immunosuppressive features that should limit vaccine response), and the precedent of cancer vaccines underperforming in MRD-positive populations.
Either way, the Ph3 readout is the falsification point. They seem to have a lot going against them in Ph3 which once again, makes sense in light of mgmt comments at Barclays wrt 0.80 HR.