Our new living guideline Therapy for Stage IV NSCLC With Driver Alterations emphasizes broad NGS & IHC (PD-L1, HER2, MET) prior to frontline therapy. Comprehensive profiling is linked to ⬆️ OS & cost-effectiveness in Stage IV NSCLC: https://t.co/Z9UhEY3zdi
#LungCancer#NSCLC
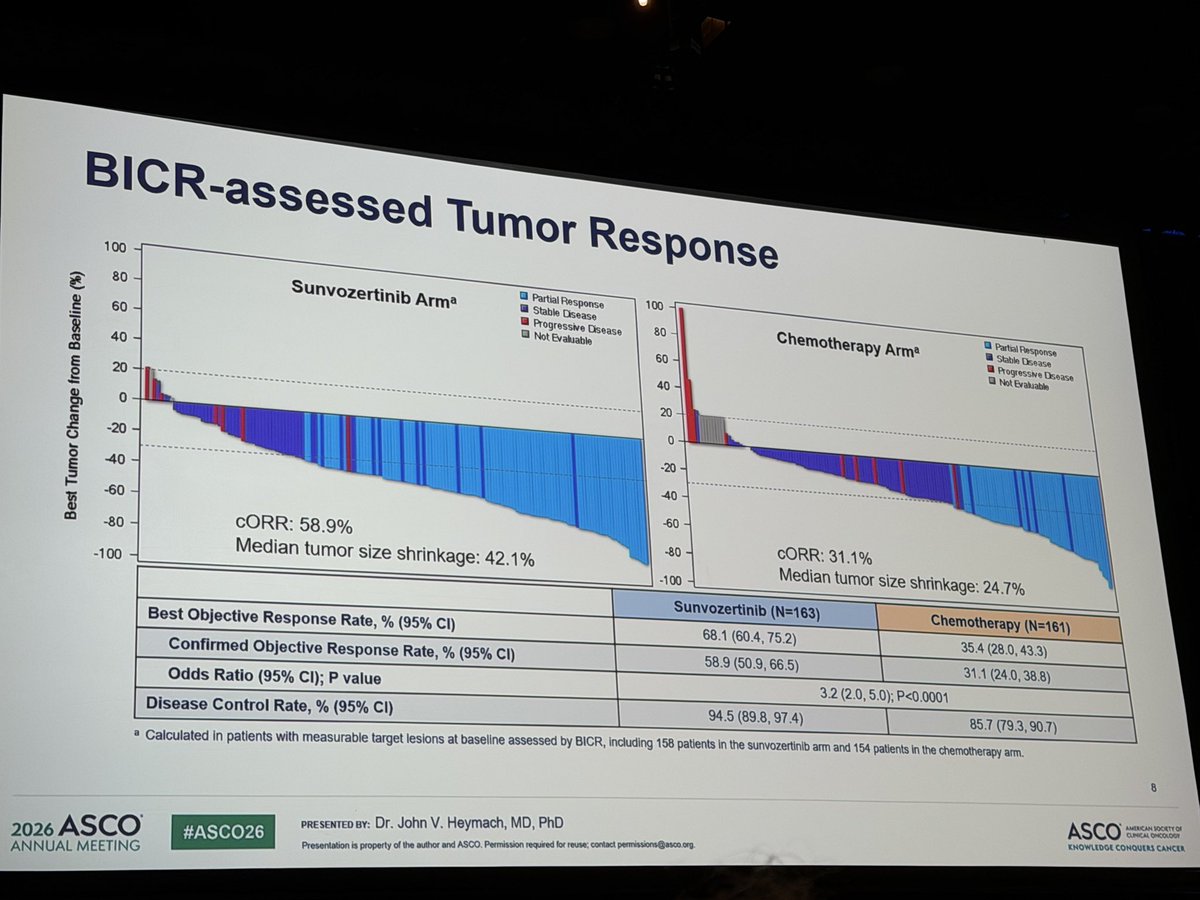
WU-KONG28: EGFR Ex20ins 1st line sunvo vs chemo; Meets PFR ORR DOR; Xover was allowed and 90% did in chemo arm; dose reductions in 40%, discontinuation 7%: #ASCO26
CHRYSALIS-2 cohort C: Ami Laz in atypical EGFR first line ; N49; ; 57% ORR; DoR 20.7m PFS 19.5m; mOS 41m👍🏽; Mutational subtype and compound status didn’t predict benefit in subgroups. The mOS probably defines the new gold standard #ASCO26
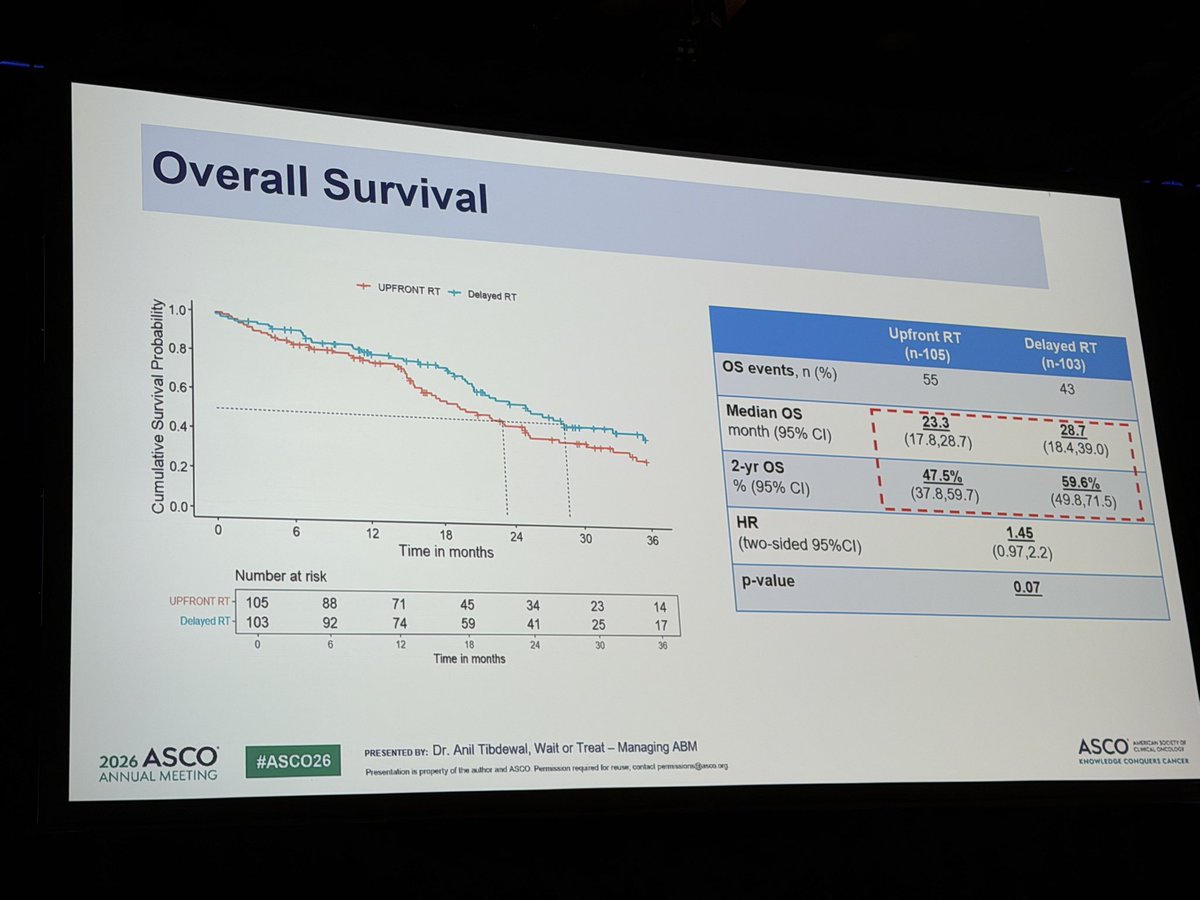
Should asymptomatic brain mets await systemic response in front line within EGFR/ALK context? I think yes. Despite reducing icPD, delayed brain RT OS looked better and radiation necrosis didn’t occur vs 6% #ASCO26
AcceleRET-LUNG: 1st line pralsetinib vs chemo;n233; 34% in chemo arm X’ed over. mPFS 9vs 18.7m HR 0.59, effect preserved in all subgroups; opportunistic infections an issue. #ASCO26