🫀��️𝗙𝗶𝘀𝗶𝗼𝗹𝗼𝗴𝗶́𝗮 𝗰𝗮𝗿𝗱𝗶𝗼𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿 𝗮𝗽𝗹𝗶𝗰𝗮𝗱𝗮 𝗮𝗹 𝗽𝗮𝗰𝗶𝗲𝗻𝘁𝗲 𝗰𝗿𝗶́𝘁𝗶𝗰𝗼: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮𝗺𝗶𝗮 𝗲𝘀 𝗰𝗹𝗮𝘃𝗲 𝗽𝗮𝗿𝗮 𝗻𝗼 𝘁𝗿𝗮𝘁𝗮𝗿 “𝗮 𝗰𝗶𝗲𝗴𝗮𝘀”🚨
@CritCareMed
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
La relación 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚n y el modelo de 𝙚𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙫𝙖𝙧𝙞𝙖𝙗𝙡𝙚 𝙚𝙣 𝙚𝙡 𝙩𝙞𝙚𝙢𝙥𝙤: base para interpretar monitorización avanzada y entender el efecto real de los tratamientos en sepsis, shock cardiogénico y soporte mecánico.
#Hemodynamics #CriticalCare
🧠 𝙀𝙡 𝙘𝙤𝙧𝙖𝙯𝙤́𝙣 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙨𝙤𝙡𝙤 𝙥𝙤𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙤 𝙜𝙖𝙨𝙩𝙤: 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤-𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡
2 conceptos centrales:
📌 𝙀𝙚𝙨 = contractilidad ventricular
📌 𝙀𝙖 = carga arterial efectiva
Y su relación 𝙀𝙖/𝙀𝙚𝙨 determina en gran parte:
🫀 fracción de eyección
🩸 volumen sistólico
📉 presión telesistólica
👉 Cuando 𝙀𝙖/𝙀𝙚𝙨 𝙨𝙪𝙗𝙚, el ventrículo se “desacopla” y el rendimiento cae.
#VentriculoArterialCoupling #Ees #Ea
📈 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙚𝙭𝙥𝙡𝙞𝙘𝙖 𝙢𝙪𝙘𝙝𝙤 𝙢𝙚𝙟𝙤𝙧 𝙡𝙤 𝙦𝙪𝙚 𝙫𝙚𝙢𝙤𝙨 𝙖𝙡 𝙥𝙞𝙚 𝙙𝙚 𝙘𝙖𝙢𝙖
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 3 del artículo, el loop muestra cómo integrar:
🔹 𝙀𝘿𝙋𝙑𝙍 → rigidez/compliance diastólica
🔹 𝙀𝙎𝙋𝙑𝙍 → contractilidad sistólica
🔹 área del loop → 𝙨𝙩𝙧𝙤𝙠𝙚 𝙬𝙤𝙧𝙠
🔹 área presión-volumen total → relación con 𝙘𝙤𝙣𝙨𝙪𝙢𝙤 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤 𝙙𝙚 𝙊₂
👉 O sea: no solo importa cuánto bombea el corazón, sino 𝙖 𝙦𝙪𝙚́ 𝙘𝙤𝙨𝙩𝙤 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙣𝙚𝙧𝙜𝙚́𝙩𝙞𝙘𝙤 𝙡𝙤 𝙝𝙖𝙘𝙚.
#PressureVolumeLoop #CardiacWork #MyocardialOxygenConsumption
🦠 𝙀𝙣 𝙨𝙚𝙥𝙨𝙞𝙨, 𝙚𝙡 𝙢𝙞𝙨𝙢𝙤 𝙖𝙡𝙜𝙤𝙧𝙞𝙩𝙢𝙤 𝙣𝙤 𝙨𝙞𝙧𝙫𝙚 𝙥𝙖𝙧𝙖 𝙩𝙤𝙙𝙤𝙨
La sepsis altera múltiples componentes a la vez:
🩸 tono arterial
🫗 capacitancia venosa
🫀 función sistólica
🫀 función diastólica
Por eso una reanimación rígida puede fallar.
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 5, la vasoplejia reduce 𝙀𝙖 y 𝙋𝙚𝙨, aumenta la FE de forma “engañosa”, pero cae el 𝙎𝙑 por menor volumen estresado y retorno venoso.
#Sepsis #Vasoplegia #Shock
💉 𝙇𝙤𝙨 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨 𝙚 𝙞𝙣𝙤𝙩𝙧𝙤́𝙥𝙞𝙘𝙤𝙨 𝙣𝙤 “𝙨𝙪𝙗𝙚𝙣 𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣” 𝙩𝙤𝙙𝙤𝙨 𝙞𝙜𝙪𝙖𝙡: 𝙘𝙖𝙢𝙗𝙞𝙖𝙣 𝙡𝙖 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖 𝙙𝙚 𝙛𝙤𝙧𝙢𝙖 𝙙𝙞𝙨𝙩𝙞𝙣𝙩𝙖
🔴 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 → ↑ SVR, ↑ Ea, ↓ capacitancia venosa, ↑ volumen estresado
🟣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖 → ↑ Ea sin mejorar Ees
🔵 𝙙𝙤𝙗𝙪𝙩𝙖𝙢𝙞𝙣𝙖 → ↑ Ees, ↓ Ea relativo, ↑ SV
🟠 𝙮 → ↓ Ea, ↓ EDP, ↑ SV
👉 La misma PAM puede lograrse con efectos completamente diferentes sobre 𝙥𝙤𝙨𝙘𝙖𝙧𝙜𝙖, 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖, 𝙑𝙎 𝙮 𝙑𝙊₂ 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤.
#Norepinephrine #Dobutamine #Vasopressin #Nitroprusside
🫀 𝙀𝙣 𝙨𝙝𝙤𝙘𝙠 𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙚́𝙣𝙞𝙘𝙤, 𝙨𝙪𝙗𝙞𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙣𝙤 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙨𝙞𝙜𝙣𝙞𝙛𝙞𝙘𝙖 𝙖𝙮𝙪𝙙𝙖𝙧 𝙖𝙡 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 7 compara 2 estrategias:
📍 𝙞𝙣𝙤𝙘𝙤𝙣𝙨𝙩𝙧𝙞𝙘𝙩𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧
vs
📍 𝙞𝙣𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧
Y deja una enseñanza potente: una estrategia que eleva mucho la presión puede empeorar 𝙀𝙖/𝙀𝙚𝙨, aumentar 𝙀𝘿𝙋 y subir el costo miocárdico.
👉 A veces una estrategia con más descarga ventricular y mejor VS puede ser fisiológicamente superior aunque la TA no “impresione” tanto.
#CardiogenicShock #Inodilator #Afterload
🚀 𝙀𝙡 𝙨𝙤��𝙤𝙧𝙩𝙚 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙘𝙤𝙣 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖, 𝙣𝙤 𝙨𝙤𝙡𝙤 𝙘𝙤𝙣 𝙛𝙡𝙪𝙟𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢𝘴 𝘱𝘢́𝘨𝘪𝘯𝘢𝘴 8–9 muestra algo clave:
⚠️ 𝙑𝘼-𝙀𝘾𝙈𝙊 puede aumentar 𝙀𝙖 y no descargar adecuadamente el VI
⚠️ el VI puede seguir con presión y volumen elevados, favoreciendo edema pulmonar y mayor consumo de O₂
✅ agregar descarga con 𝙇𝙑𝘼𝘿/𝙄𝙢𝙥𝙚𝙡𝙡𝙖 o usar estrategias farmacológicas de descarga puede reducir 𝙀𝘿𝙑, 𝙀𝘿𝙋 𝙮 𝙋𝙑𝘼
🔥 Take-home: este review recuerda que la hemodinamia avanzada no debe usarse para perseguir números aislados, sino para identificar el 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤 𝙘𝙖𝙧𝙙𝙞𝙤𝙫𝙖𝙨𝙘𝙪𝙡𝙖𝙧 𝙧𝙚𝙖𝙡 y elegir terapias que mejoren 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤, 𝙥𝙚𝙧𝙛𝙪𝙨𝙞𝙤́𝙣 𝙮 𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙖.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/b0RJ3TaB9I]
#ClubCrit #ShockCardiogénico #Sepsis #ECMO #Impella #Hemodynamics #CriticalCare #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada
ASE and @accpchest recently partnered on a project to develop two educational webinars to improve the understanding of cardiovascular ultrasound's application in pulmonary hypertension (PH). @chest
You can find them on our Right Heart Resources web page! https://t.co/aHA1IniTS3
🔔 ¿Seguimos esperando a que la creatinina sérica suba para diagnosticar una Lesión Renal Aguda?
Llegamos tarde.
La línea de tiempo conceptual presentada en el #ERA26 demuestra que la creatinina y la caída del volumen urinario son marcadores de disfunción clínica tard��a, no de daño temprano.
El estrés renal inicia mucho antes con la parada del ciclo celular, detectable inmediatamente tras el insulto mediante biomarcadores ultrasensibles como TIMP-2 e IGFBP7.
Cambiar nuestra mentalidad del diagnóstico funcional al molecular es imperativo para la nefroprotección crítica.
#Nefrología #MedicinaCrítica #ERA26 #AKI #NefroTwitter
#lesionrenalaguda #dañorenal #IRA #AKI
Siguiendo las recomendaciones de los expertos. 🙌🏼✨. Aunque el contexto difiere (adultos - pediátricos) las metas de reanimación o evacuación no están bien definidas en portadores de cardiopatías sometidos a cirugia paliativa. Paciente Canal AV + insuficiencia moderada valvular
🤓ICU POCUS should not be learned as “views.” It should be learned as progressive clinical responsibility.
Recent PubMed indexed guidance supports critical care ultrasonography as a bedside tool for septic shock, acute dyspnea or respiratory failure, volume management, and cardiogenic shock (Díaz-Gómez et al., 2025). A 2024 meta analysis also suggests POCUS guided resuscitation may reduce 28 day mortality, vasoactive drug duration, and renal replacement therapy use, although evidence quality remains variable (Basmaji et al., 2024).
A practical ICU curriculum could be divided into levels.
Before entering to ICU: know machine handling, probe selection, image optimization, lung sliding, pleural effusion, basic IVC, free fluid, bladder, DVT compression, FAST and ultrasound guided vascular access.
ICU resident: add structured lung ultrasound, focused cardiac ultrasound, LV/RV function, pericardial effusion, shock phenotyping, fluid tolerance, congestion, pneumothorax, diaphragm ultrasound, ONSD and procedural guidance.
ICU specialist: integrate heart lung vein ultrasound into decisions: fluids, vasopressors, inotropes, ventilation, PEEP, weaning, RV failure, tamponade, pulmonary embolism, TCD, ARDS, and cardiorenal congestion.
Specialized ICU: advanced echocardiography, TEE, strain, advanced TCD, complex valvular disease, mechanical circulatory support, ECMO cannulation and troubleshooting, and quality assurance.
The danger is not using ultrasound. The danger is using ultrasound without competence, supervision, documentation, and clinical integration.
Best practice documents emphasize structured training, competency assessment, image archiving, quality assurance, and local governance (Oto et al., 2024; Patrawalla et al., 2025).
The key question is not:
“Can you obtain the image?”
It is:
Can you acquire it, interpret it, and safely change management because of it?
#ICU #CriticalCare #POCUS #Ultrasound #FOCUS #LungUltrasound #Hemodynamics #Shock #MedicalEducation #PatientSafety
References 📚
Basmaji, J., et al. (2024). The impact of point-of-care ultrasound-guided resuscitation on clinical outcomes in critically ill patients: A systematic review and meta-analysis. Critical Care Medicine. https://t.co/HLHERp2BsJ
Díaz-Gómez, J. L., Sharif, S., Ablordeppey, E., et al. (2025). Society of Critical Care Medicine guidelines on adult critical care ultrasonography: Focused update 2024. Critical Care Medicine, 53(2), e447–e458. https://t.co/LLyXUCdqu4
Oto, B., et al. (2024). Best practices for point of care ultrasound. Ultrasound Journal, 16, 15. https://t.co/I2wkLgUpJl
Patrawalla, P., et al. (2025). Best practices for a competency-based curriculum in critical care ultrasonography. Chest. https://t.co/mtdLj6opqj
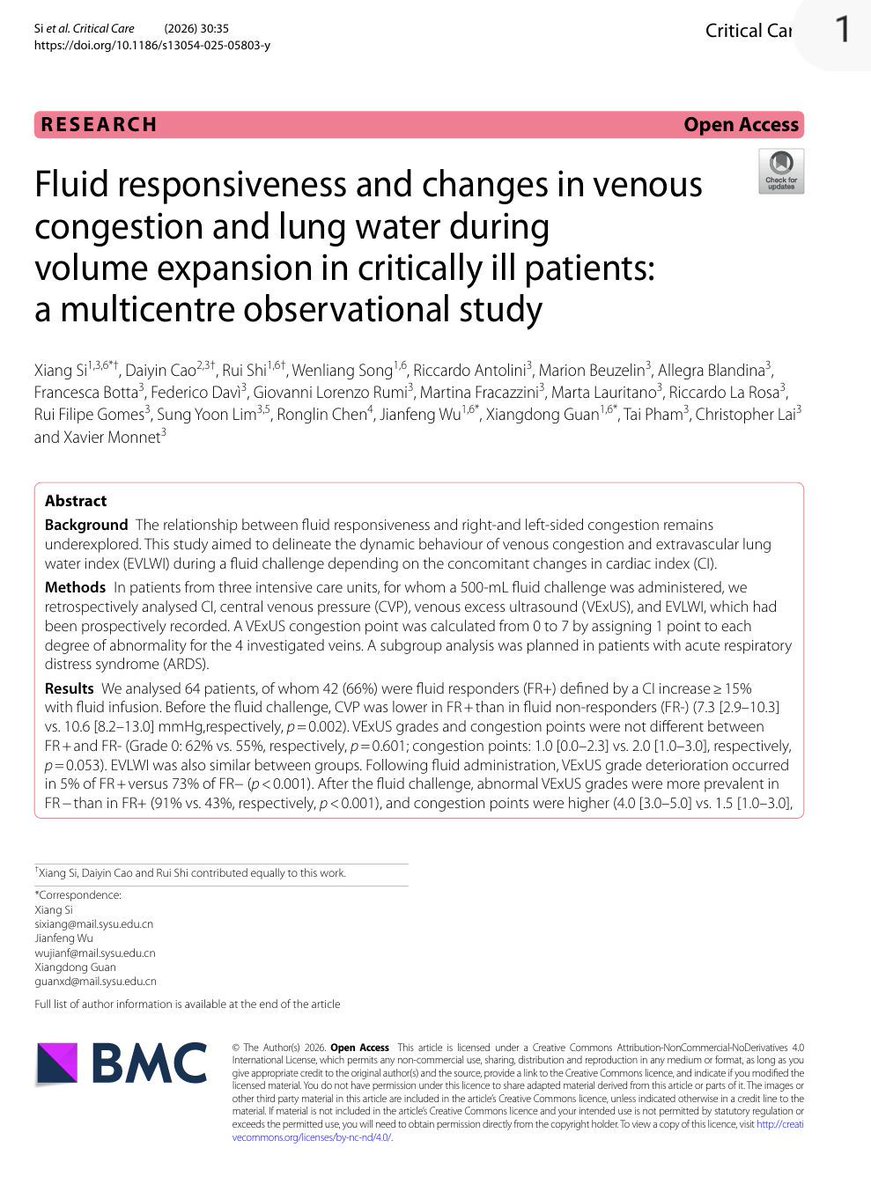
💧 Fluid Responsiveness ≠ Fluid Tolerance
For years, critical care clinicians have focused on a fundamental question:
Will this patient increase cardiac output if I give fluids?
A new multicentre study from France and China suggests we may need to ask a second question:
What price will the patient pay for that fluid?
In this observational study of 64 critically ill patients receiving a standardized 500 mL fluid challenge, investigators evaluated not only cardiac index (CI), but also venous congestion using VExUS and pulmonary congestion using extravascular lung water (EVLWI).
The findings are striking.
Before fluid administration, venous congestion could coexist with fluid responsiveness. In fact, many patients remained preload responsive despite already demonstrating evidence of systemic venous congestion.
However, what happened after fluid administration was even more important.
Among fluid responders:
✅ Cardiac index increased significantly
✅ Venous congestion remained largely stable
✅ Only 5% experienced worsening VExUS grade
✅ Lung water remained relatively unchanged
Among fluid non-responders:
❌ Cardiac output barely changed
❌ Venous congestion worsened dramatically
❌ VExUS deterioration occurred in 73%
❌ EVLWI increased significantly
❌ Congestion became evident across hepatic, portal, and renal venous territories
Perhaps the most important physiological message is this:
When the heart cannot convert preload into flow, the fluid has to go somewhere.
And where it goes is congestion.
The study also found a strong correlation between CVP and VExUS, suggesting that while advanced ultrasound provides valuable organ-level information, a carefully interpreted CVP may still remain a useful bedside marker of right-sided congestion.
The ARDS subgroup provides another important lesson.
Even fluid-responsive ARDS patients accumulated more extravascular lung water after fluid administration than non-ARDS patients, highlighting the role of pulmonary permeability in determining fluid tolerance.
This study reinforces a concept that is increasingly central to modern hemodynamic management:
The goal is not simply to identify fluid responsiveness.
The goal is to identify patients who are both:
✔ Fluid responsive
✔ Fluid tolerant
A fluid challenge that increases congestion without increasing flow is not resuscitation.
It is fluid accumulation.
The future of hemodynamic management may lie at the intersection of:
• Fluid responsiveness
• Venous congestion assessment
• Pulmonary permeability
• Organ-specific fluid tolerance
Because the best fluid is not the one that can be given.
It is the one that provides benefit without causing harm.
Reference , 📚
Si X, Critical Care. 2026;30:35.
#POCUS#MedTwitter#Nephpearls
Many #VExUS enthusiasts asked for a #tweetorial on image acquisition pearls. Did one b4 but time for an updated one 🧵
#1 Let's start with basics
Color Doppler identifies the flow + tells the direction (blue is away & red towards the probe [BART])
Dios nos acompañe en este trabajo de #PedsICU y sobre todo soporte la vida de estos niños y sus padres que sufren día con día. Aquí se vive la misericordia del señor.
La PVC cambió de ser un indicador de HIPOVOLEMIA, a ser marcador de CONGESTIÓN VENOSA, en especial asociada a LRA. Usar volumen según la PVC, puede inducir paradójicamente congestión venosa…
https://t.co/pMz1sV0uRg
Today's Paper of the Day is:
Advances in achieving lung and diaphragm-protective ventilation
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
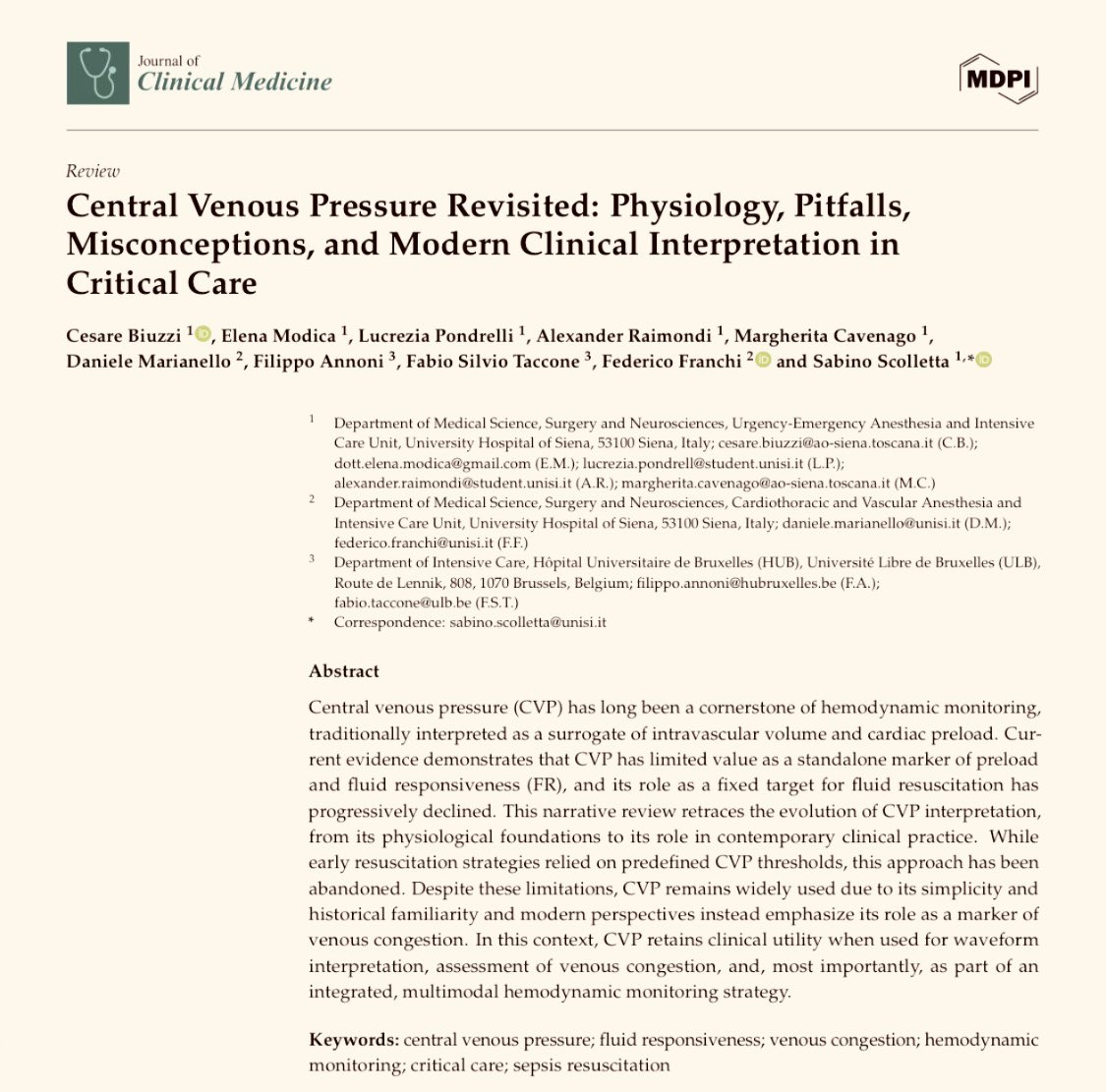
Central Venous Pressure Revisited: Physiology, Pitfalls, Misconceptions, and Modern Clinical Interpretation in Critical Care
CCR Journal Watch
https://t.co/Sp06oA6IDG
🫀POCUS is no longer just a bedside imaging tool.
It is becoming real time physiological intelligence.
This excellent 2026 review highlights how modern POCUS is expanding into:
• ultrasound guided regional anesthesia
• shock and cardiac arrest management
• AI assisted imaging
• advanced diagnostics
• governance and medicolegal practice
Some of the most provocative concepts: • “Occult VF” detectable only on echocardiography during cardiac arrest
• Ultrasound guided CPR compression positioning
• AI assisted lung ultrasound acquisition by nonexperts
• Handheld devices approaching cart based diagnostic performance
One important medicolegal message: several lawsuits involved failure to perform POCUS when clinically indicated.
The future of emergency and critical care medicine will likely depend on clinicians capable of integrating: physiology + imaging + AI + rapid bedside decision making.
POCUS is not anymore an “optional skill” but “core clinical infrastructure.”
Mani N, Rao S, Kim DJ. Point-of-care ultrasound in the modern era of emergency medicine: a narrative review of the recent literature. Curr Opin Crit Care. 2026. doi:10.1097/MCC.0000000000001358

![MarlonVFZR's tweet photo. 🫀��️𝗙𝗶𝘀𝗶𝗼𝗹𝗼𝗴𝗶́𝗮 𝗰𝗮𝗿𝗱𝗶𝗼𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿 𝗮𝗽𝗹𝗶𝗰𝗮𝗱𝗮 𝗮𝗹 𝗽𝗮𝗰𝗶𝗲𝗻𝘁𝗲 𝗰𝗿𝗶́𝘁𝗶𝗰𝗼: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮𝗺𝗶𝗮 𝗲𝘀 𝗰𝗹𝗮𝘃𝗲 𝗽𝗮𝗿𝗮 𝗻𝗼 𝘁𝗿𝗮𝘁𝗮𝗿 “𝗮 𝗰𝗶𝗲𝗴𝗮𝘀”🚨
@CritCareMed
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
La relación 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚n y el modelo de 𝙚𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙫𝙖𝙧𝙞𝙖𝙗𝙡𝙚 𝙚𝙣 𝙚𝙡 𝙩𝙞𝙚𝙢𝙥𝙤: base para interpretar monitorización avanzada y entender el efecto real de los tratamientos en sepsis, shock cardiogénico y soporte mecánico.
#Hemodynamics #CriticalCare
🧠 𝙀𝙡 𝙘𝙤𝙧𝙖𝙯𝙤́𝙣 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙨𝙤𝙡𝙤 𝙥𝙤𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙤 𝙜𝙖𝙨𝙩𝙤: 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤-𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡
2 conceptos centrales:
📌 𝙀𝙚𝙨 = contractilidad ventricular
📌 𝙀𝙖 = carga arterial efectiva
Y su relación 𝙀𝙖/𝙀𝙚𝙨 determina en gran parte:
🫀 fracción de eyección
🩸 volumen sistólico
📉 presión telesistólica
👉 Cuando 𝙀𝙖/𝙀𝙚𝙨 𝙨𝙪𝙗𝙚, el ventrículo se “desacopla” y el rendimiento cae.
#VentriculoArterialCoupling #Ees #Ea
📈 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙚𝙭𝙥𝙡𝙞𝙘𝙖 𝙢𝙪𝙘𝙝𝙤 𝙢𝙚𝙟𝙤𝙧 𝙡𝙤 𝙦𝙪𝙚 𝙫𝙚𝙢𝙤𝙨 𝙖𝙡 𝙥𝙞𝙚 𝙙𝙚 𝙘𝙖𝙢𝙖
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 3 del artículo, el loop muestra cómo integrar:
🔹 𝙀𝘿𝙋𝙑𝙍 → rigidez/compliance diastólica
🔹 𝙀𝙎𝙋𝙑𝙍 → contractilidad sistólica
🔹 área del loop → 𝙨𝙩𝙧𝙤𝙠𝙚 𝙬𝙤𝙧𝙠
🔹 área presión-volumen total → relación con 𝙘𝙤𝙣𝙨𝙪𝙢𝙤 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤 𝙙𝙚 𝙊₂
👉 O sea: no solo importa cuánto bombea el corazón, sino 𝙖 𝙦𝙪𝙚́ 𝙘𝙤𝙨𝙩𝙤 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙣𝙚𝙧𝙜𝙚́𝙩𝙞𝙘𝙤 𝙡𝙤 𝙝𝙖𝙘𝙚.
#PressureVolumeLoop #CardiacWork #MyocardialOxygenConsumption
🦠 𝙀𝙣 𝙨𝙚𝙥𝙨𝙞𝙨, 𝙚𝙡 𝙢𝙞𝙨𝙢𝙤 𝙖𝙡𝙜𝙤𝙧𝙞𝙩𝙢𝙤 𝙣𝙤 𝙨𝙞𝙧𝙫𝙚 𝙥𝙖𝙧𝙖 𝙩𝙤𝙙𝙤𝙨
La sepsis altera múltiples componentes a la vez:
🩸 tono arterial
🫗 capacitancia venosa
🫀 función sistólica
🫀 función diastólica
Por eso una reanimación rígida puede fallar.
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 5, la vasoplejia reduce 𝙀𝙖 y 𝙋𝙚𝙨, aumenta la FE de forma “engañosa”, pero cae el 𝙎𝙑 por menor volumen estresado y retorno venoso.
#Sepsis #Vasoplegia #Shock
💉 𝙇𝙤𝙨 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨 𝙚 𝙞𝙣𝙤𝙩𝙧𝙤́𝙥𝙞𝙘𝙤𝙨 𝙣𝙤 “𝙨𝙪𝙗𝙚𝙣 𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣” 𝙩𝙤𝙙𝙤𝙨 𝙞𝙜𝙪𝙖𝙡: 𝙘𝙖𝙢𝙗𝙞𝙖𝙣 𝙡𝙖 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖 𝙙𝙚 𝙛𝙤𝙧𝙢𝙖 𝙙𝙞𝙨𝙩𝙞𝙣𝙩𝙖
🔴 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 → ↑ SVR, ↑ Ea, ↓ capacitancia venosa, ↑ volumen estresado
🟣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖 → ↑ Ea sin mejorar Ees
🔵 𝙙𝙤𝙗𝙪𝙩𝙖𝙢𝙞𝙣𝙖 → ↑ Ees, ↓ Ea relativo, ↑ SV
🟠 𝙮 → ↓ Ea, ↓ EDP, ↑ SV
👉 La misma PAM puede lograrse con efectos completamente diferentes sobre 𝙥𝙤𝙨𝙘𝙖𝙧𝙜𝙖, 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖, 𝙑𝙎 𝙮 𝙑𝙊₂ 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤.
#Norepinephrine #Dobutamine #Vasopressin #Nitroprusside
🫀 𝙀𝙣 𝙨𝙝𝙤𝙘𝙠 𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙚́𝙣𝙞𝙘𝙤, 𝙨𝙪𝙗𝙞𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙣𝙤 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙨𝙞𝙜𝙣𝙞𝙛𝙞𝙘𝙖 𝙖𝙮𝙪𝙙𝙖𝙧 𝙖𝙡 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 7 compara 2 estrategias:
📍 𝙞𝙣𝙤𝙘𝙤𝙣𝙨𝙩𝙧𝙞𝙘𝙩𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧
vs
📍 𝙞𝙣𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧
Y deja una enseñanza potente: una estrategia que eleva mucho la presión puede empeorar 𝙀𝙖/𝙀𝙚𝙨, aumentar 𝙀𝘿𝙋 y subir el costo miocárdico.
👉 A veces una estrategia con más descarga ventricular y mejor VS puede ser fisiológicamente superior aunque la TA no “impresione” tanto.
#CardiogenicShock #Inodilator #Afterload
🚀 𝙀𝙡 𝙨𝙤��𝙤𝙧𝙩𝙚 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙘𝙤𝙣 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖, 𝙣𝙤 𝙨𝙤𝙡𝙤 𝙘𝙤𝙣 𝙛𝙡𝙪𝙟𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢𝘴 𝘱𝘢́𝘨𝘪𝘯𝘢𝘴 8–9 muestra algo clave:
⚠️ 𝙑𝘼-𝙀𝘾𝙈𝙊 puede aumentar 𝙀𝙖 y no descargar adecuadamente el VI
⚠️ el VI puede seguir con presión y volumen elevados, favoreciendo edema pulmonar y mayor consumo de O₂
✅ agregar descarga con 𝙇𝙑𝘼𝘿/𝙄𝙢𝙥𝙚𝙡𝙡𝙖 o usar estrategias farmacológicas de descarga puede reducir 𝙀𝘿𝙑, 𝙀𝘿𝙋 𝙮 𝙋𝙑𝘼
🔥 Take-home: este review recuerda que la hemodinamia avanzada no debe usarse para perseguir números aislados, sino para identificar el 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤 𝙘𝙖𝙧𝙙𝙞𝙤𝙫𝙖𝙨𝙘𝙪𝙡𝙖𝙧 𝙧𝙚𝙖𝙡 y elegir terapias que mejoren 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤, 𝙥𝙚𝙧𝙛𝙪𝙨𝙞𝙤́𝙣 𝙮 𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙖.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/b0RJ3TaB9I]
#ClubCrit #ShockCardiogénico #Sepsis #ECMO #Impella #Hemodynamics #CriticalCare #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HKX63pHWEAA2_2p.jpg)




















![MarlonVFZR's tweet photo. 🫀��️𝗙𝗶𝘀𝗶𝗼𝗹𝗼𝗴𝗶́𝗮 𝗰𝗮𝗿𝗱𝗶𝗼𝘃𝗮𝘀𝗰𝘂𝗹𝗮𝗿 𝗮𝗽𝗹𝗶𝗰𝗮𝗱𝗮 𝗮𝗹 𝗽𝗮𝗰𝗶𝗲𝗻𝘁𝗲 𝗰𝗿𝗶́𝘁𝗶𝗰𝗼: 𝗲𝗻𝘁𝗲𝗻𝗱𝗲𝗿 𝗹𝗮 𝗵𝗲𝗺𝗼𝗱𝗶𝗻𝗮𝗺𝗶𝗮 𝗲𝘀 𝗰𝗹𝗮𝘃𝗲 𝗽𝗮𝗿𝗮 𝗻𝗼 𝘁𝗿𝗮𝘁𝗮𝗿 “𝗮 𝗰𝗶𝗲𝗴𝗮𝘀”🚨
@CritCareMed
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
https://t.co/89ht2mBRSA
⬇️⬇️⬇️⬇️
🧵👇
La relación 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚n y el modelo de 𝙚𝙡𝙖𝙨𝙩𝙖𝙣𝙘𝙞𝙖 𝙫𝙖𝙧𝙞𝙖𝙗𝙡𝙚 𝙚𝙣 𝙚𝙡 𝙩𝙞𝙚𝙢𝙥𝙤: base para interpretar monitorización avanzada y entender el efecto real de los tratamientos en sepsis, shock cardiogénico y soporte mecánico.
#Hemodynamics #CriticalCare
🧠 𝙀𝙡 𝙘𝙤𝙧𝙖𝙯𝙤́𝙣 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙨𝙤𝙡𝙤 𝙥𝙤𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙤 𝙜𝙖𝙨𝙩𝙤: 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤-𝙖𝙧𝙩𝙚𝙧𝙞𝙖𝙡
2 conceptos centrales:
📌 𝙀𝙚𝙨 = contractilidad ventricular
📌 𝙀𝙖 = carga arterial efectiva
Y su relación 𝙀𝙖/𝙀𝙚𝙨 determina en gran parte:
🫀 fracción de eyección
🩸 volumen sistólico
📉 presión telesistólica
👉 Cuando 𝙀𝙖/𝙀𝙚𝙨 𝙨𝙪𝙗𝙚, el ventrículo se “desacopla” y el rendimiento cae.
#VentriculoArterialCoupling #Ees #Ea
📈 𝙇𝙖 𝙘𝙪𝙧𝙫𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣-𝙫𝙤𝙡𝙪𝙢𝙚𝙣 𝙚𝙭𝙥𝙡𝙞𝙘𝙖 𝙢𝙪𝙘𝙝𝙤 𝙢𝙚𝙟𝙤𝙧 𝙡𝙤 𝙦𝙪𝙚 𝙫𝙚𝙢𝙤𝙨 𝙖𝙡 𝙥𝙞𝙚 𝙙𝙚 𝙘𝙖𝙢𝙖
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 3 del artículo, el loop muestra cómo integrar:
🔹 𝙀𝘿𝙋𝙑𝙍 → rigidez/compliance diastólica
🔹 𝙀𝙎𝙋𝙑𝙍 → contractilidad sistólica
🔹 área del loop → 𝙨𝙩𝙧𝙤𝙠𝙚 𝙬𝙤𝙧𝙠
🔹 área presión-volumen total → relación con 𝙘𝙤𝙣𝙨𝙪𝙢𝙤 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤 𝙙𝙚 𝙊₂
👉 O sea: no solo importa cuánto bombea el corazón, sino 𝙖 𝙦𝙪𝙚́ 𝙘𝙤𝙨𝙩𝙤 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙮 𝙚𝙣𝙚𝙧𝙜𝙚́𝙩𝙞𝙘𝙤 𝙡𝙤 𝙝𝙖𝙘𝙚.
#PressureVolumeLoop #CardiacWork #MyocardialOxygenConsumption
🦠 𝙀𝙣 𝙨𝙚𝙥𝙨𝙞𝙨, 𝙚𝙡 𝙢𝙞𝙨𝙢𝙤 𝙖𝙡𝙜𝙤𝙧𝙞𝙩𝙢𝙤 𝙣𝙤 𝙨𝙞𝙧𝙫𝙚 𝙥𝙖𝙧𝙖 𝙩𝙤𝙙𝙤𝙨
La sepsis altera múltiples componentes a la vez:
🩸 tono arterial
🫗 capacitancia venosa
🫀 función sistólica
🫀 función diastólica
Por eso una reanimación rígida puede fallar.
En la 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 5, la vasoplejia reduce 𝙀𝙖 y 𝙋𝙚𝙨, aumenta la FE de forma “engañosa”, pero cae el 𝙎𝙑 por menor volumen estresado y retorno venoso.
#Sepsis #Vasoplegia #Shock
💉 𝙇𝙤𝙨 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧𝙚𝙨 𝙚 𝙞𝙣𝙤𝙩𝙧𝙤́𝙥𝙞𝙘𝙤𝙨 𝙣𝙤 “𝙨𝙪𝙗𝙚𝙣 𝙡𝙖 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣” 𝙩𝙤𝙙𝙤𝙨 𝙞𝙜𝙪𝙖𝙡: 𝙘𝙖𝙢𝙗𝙞𝙖𝙣 𝙡𝙖 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖 𝙙𝙚 𝙛𝙤𝙧𝙢𝙖 𝙙𝙞𝙨𝙩𝙞𝙣𝙩𝙖
🔴 𝙣𝙤𝙧𝙚𝙥𝙞𝙣𝙚𝙛𝙧𝙞𝙣𝙖 → ↑ SVR, ↑ Ea, ↓ capacitancia venosa, ↑ volumen estresado
🟣 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙞𝙣𝙖 → ↑ Ea sin mejorar Ees
🔵 𝙙𝙤𝙗𝙪𝙩𝙖𝙢𝙞𝙣𝙖 → ↑ Ees, ↓ Ea relativo, ↑ SV
🟠 𝙮 → ↓ Ea, ↓ EDP, ↑ SV
👉 La misma PAM puede lograrse con efectos completamente diferentes sobre 𝙥𝙤𝙨𝙘𝙖𝙧𝙜𝙖, 𝙥𝙧𝙚𝙘𝙖𝙧𝙜𝙖, 𝙑𝙎 𝙮 𝙑𝙊₂ 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙤.
#Norepinephrine #Dobutamine #Vasopressin #Nitroprusside
🫀 𝙀𝙣 𝙨𝙝𝙤𝙘𝙠 𝙘𝙖𝙧𝙙𝙞𝙤𝙜𝙚́𝙣𝙞𝙘𝙤, 𝙨𝙪𝙗𝙞𝙧 𝙥𝙧𝙚𝙨𝙞𝙤́𝙣 𝙣𝙤 𝙨𝙞𝙚𝙢𝙥𝙧𝙚 𝙨𝙞𝙜𝙣𝙞𝙛𝙞𝙘𝙖 𝙖𝙮𝙪𝙙𝙖𝙧 𝙖𝙡 𝙫𝙚𝙣𝙩𝙧𝙞́𝙘𝙪𝙡𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢 𝘱𝘢́𝘨𝘪𝘯𝘢 7 compara 2 estrategias:
📍 𝙞𝙣𝙤𝙘𝙤𝙣𝙨𝙩𝙧𝙞𝙘𝙩𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙥𝙧𝙚𝙨𝙤𝙧
vs
📍 𝙞𝙣𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧 + 𝙫𝙖𝙨𝙤𝙙𝙞𝙡𝙖𝙩𝙖𝙙𝙤𝙧
Y deja una enseñanza potente: una estrategia que eleva mucho la presión puede empeorar 𝙀𝙖/𝙀𝙚𝙨, aumentar 𝙀𝘿𝙋 y subir el costo miocárdico.
👉 A veces una estrategia con más descarga ventricular y mejor VS puede ser fisiológicamente superior aunque la TA no “impresione” tanto.
#CardiogenicShock #Inodilator #Afterload
🚀 𝙀𝙡 𝙨𝙤��𝙤𝙧𝙩𝙚 𝙢𝙚𝙘𝙖́𝙣𝙞𝙘𝙤 𝙩𝙖𝙢𝙗𝙞𝙚́𝙣 𝙙𝙚𝙗𝙚 𝙖𝙣𝙖𝙡𝙞𝙯𝙖𝙧𝙨𝙚 𝙘𝙤𝙣 𝙛𝙞𝙨𝙞𝙤𝙡𝙤𝙜𝙞́𝙖, 𝙣𝙤 𝙨𝙤𝙡𝙤 𝙘𝙤𝙣 𝙛𝙡𝙪𝙟𝙤
La 𝘧𝘪𝘨𝘶𝘳𝘢 𝘥𝘦 𝘭𝘢𝘴 𝘱𝘢́𝘨𝘪𝘯𝘢𝘴 8–9 muestra algo clave:
⚠️ 𝙑𝘼-𝙀𝘾𝙈𝙊 puede aumentar 𝙀𝙖 y no descargar adecuadamente el VI
⚠️ el VI puede seguir con presión y volumen elevados, favoreciendo edema pulmonar y mayor consumo de O₂
✅ agregar descarga con 𝙇𝙑𝘼𝘿/𝙄𝙢𝙥𝙚𝙡𝙡𝙖 o usar estrategias farmacológicas de descarga puede reducir 𝙀𝘿𝙑, 𝙀𝘿𝙋 𝙮 𝙋𝙑𝘼
🔥 Take-home: este review recuerda que la hemodinamia avanzada no debe usarse para perseguir números aislados, sino para identificar el 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤 𝙘𝙖𝙧𝙙𝙞𝙤𝙫𝙖𝙨𝙘𝙪𝙡𝙖𝙧 𝙧𝙚𝙖𝙡 y elegir terapias que mejoren 𝙖𝙘𝙤𝙥𝙡𝙖𝙢𝙞𝙚𝙣𝙩𝙤, 𝙥𝙚𝙧𝙛𝙪𝙨𝙞𝙤́𝙣 𝙮 𝙚𝙛𝙞𝙘𝙞𝙚𝙣𝙘𝙞𝙖 𝙢𝙞𝙤𝙘𝙖́𝙧𝙙𝙞𝙘𝙖.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en 𝕏 @MarlonVFZR y en el blog 👉 [https://t.co/b0RJ3TaB9I]
#ClubCrit #ShockCardiogénico #Sepsis #ECMO #Impella #Hemodynamics #CriticalCare #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada](https://pbs.twimg.com/media/HKX63qOXIAA7-Go.jpg)