@topmedtalk launches our “TopMedTalk Classics” series with a classic from 2018 still prescient today. Sir Bruce Keogh marked the NHS’s 70th birthday; a time framed by political volatility, financial constraint, rising demand & shifting public expectations
https://t.co/VumufRqGQX
When Mechanical Power Remains High Despite Conventional Lung-Protective Settings: A Physiology-Driven Bedside Framework
CCR Journal Watch
https://t.co/Sp06oA6IDG
🤒Fever is not the rule in sepsis.
And perhaps we have underestimated what the absence of fever actually means.
This important multicentre Australian cohort study analyzed more than 15,000 ICU patients with sepsis and found something striking:
Only 1 in 15 septic ICU patients arrived with a temperature ≥38.3°C.
Most septic patients were either normothermic or hypothermic.
Even more interesting: 21% arrived hypothermic (<36°C), and this group had the highest mortality, vasopressor requirement, mechanical ventilation use, and renal replacement therapy rates.
30 day mortality:
• Fever ≥38.3°C → 14%
• Normothermia 36–37.4°C → 12%
• Hypothermia <36°C → 17%
The paper introduces a fascinating concept: “fever deficit”
Defined as the cumulative degree-hours below 38.3°C during the first 72h of ICU admission.
Patients with hypothermia accumulated massive fever deficits: median 85 degree-hours over 72h.
The physiology behind this may be extremely important.
Fever is not simply a symptom. It is a coordinated host defense response:
• enhanced leukocyte function
• increased cytokine signaling
• improved microbial clearance
• reduced pathogen replication
• potentiation of antibiotic activity
Hypothermia in sepsis may represent:
• immune exhaustion
• failed thermoregulatory response
• depleted physiological reserve
• maladaptive host response
The authors even raise a provocative possibility:
Should we actively warm afebrile septic patients toward high-normal or supranormal temperatures?
Not just “avoid hypothermia”… but therapeutic hyperthermia.
That idea sounds radical at first glance, yet several observations support it:
• hypothermic sepsis consistently carries worse outcomes
• microbial growth increases at lower temperatures
• antibiotic efficacy may decrease in hypothermia
• febrile patients often survive more frequently than afebrile patients
One particularly important finding: temperatures normalized rapidly during the first 12-24h in ICU, but patients rarely became febrile afterward.
Meaning: our current ICU practice may unintentionally suppress or fail to restore a potentially protective physiological response.
This paper opens an important discussion in critical care:
In selected septic patients, should temperature become a therapeutic target similar to MAP, oxygenation, or perfusion?
Excellent paper challenging one of the oldest assumptions in ICU medicine, that fever in sepsis is primarily harmful.
Reference 📚
White KC et al. Sepsis in the absence of fever: Determining the criteria for and feasibility of future therapeutic temperature management trials. Critical Care and Resuscitation. 2025;27:100135. https://t.co/U7GJKjbWqT
Today's Paper of the Day is:
Advances in achieving lung and diaphragm-protective ventilation
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
In the POCUS era, estimating a patient's ejection fraction at the bedside feels trivial. Yet, most clinicians are not trained in POCUS and continue to rely on auscultation.
Cardiologists are among the most highly trained auscultators in medicine. Yet in a blinded study comparing a stethoscope to POCUS, they correctly identified only 35% of patients with reduced left ventricular ejection fraction.
POCUS identified 96%.
🫁COPD ventilation is not ARDS ventilation.
In acute COPD exacerbation, the enemy is often not alveolar collapse. It is expiratory flow limitation, dynamic hyperinflation, intrinsic PEEP, respiratory muscle overload, and CO₂ retention.
Recent PubMed indexed literature from 2023 to 2026 reinforces a practical message: in acute hypercapnic COPD exacerbation, NIV remains the first line ventilatory strategy when there is respiratory acidosis, increased work of breathing, and no immediate contraindication (Farmer et al., 2024; Mein & Ferrera, 2025). HFNC may be useful in selected patients, especially when NIV is not tolerated, but recent meta analysis suggests higher treatment failure and crossover to NIV, so it should not replace NIV as default support in acidotic AECOPD (Qin et al., 2025).
The invasive ventilation strategy is different from hypoxemic lung disease.
For the intubated COPD patient, the goal is not to normalize PaCO₂ quickly. The goal is to reduce dynamic hyperinflation.
That means:
Low respiratory rate
Long expiratory time
Modest tidal volume, usually around 6 to 8 mL/kg predicted body weight
Avoidance of excessive minute ventilation
Permissive hypercapnia when pH is acceptable
Monitoring plateau pressure, driving pressure, auto PEEP, expiratory flow, and hemodynamics
PEEP is the controversial part.
External PEEP can help when the patient is spontaneously triggering, because it reduces the inspiratory threshold load caused by intrinsic PEEP. In this context, carefully applied external PEEP may improve synchrony, reduce work of breathing, and facilitate assisted ventilation (Jubran, 2024).
But in controlled ventilation without spontaneous effort, excessive external PEEP may worsen hyperinflation, raise plateau pressure, reduce venous return, increase RV afterload, and precipitate hypotension. Here, low PEEP or minimal PEEP may be safer unless oxygenation requires more support.
A practical bedside rule:
If the COPD patient is triggering and fighting auto PEEP, external PEEP may help.
If the COPD patient is passive, hypotensive, hyperinflated, and not oxygenation limited, high PEEP may harm.
The ventilator question is not:
“How much PEEP does COPD need?”
It is:
Is PEEP unloading the patient, or inflating the trap?
#COPD #CriticalCare #ICU #MechanicalVentilation #NIV #AutoPEEP #Hypercapnia #RespiratoryFailure #VentilatorManagement #IntensiveCare
References📚
*Farmer, M. J. S. Chest, 165(6), 1473–1483. https://t.co/ZgblBs1ZZK
*Jubran, A. Current Opinion in Critical Care, 30(1), 89–96. https://t.co/JKkchvgKDj
*Mein, S. A. CHEST Critical Care, 3(1), 100107. https://t.co/tO69w9ahnl
*Qin, J., Annals of Intensive Care, 15, 64. https://t.co/ay4Wgxbpai
Today's Paper of the Day is:
Invasive Mechanical Ventilation
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
B-lines are most often discussed in the context of pulmonary edema. But the spacing between them carries a different kind of information — one that reflects structural lung disease rather than fluid overload.
🫁PEEP in ARDS is no longer just a number. It is a phenotype test.
The last 3 years of PubMed indexed literature show a clear shift in ARDS ventilation: from oxygenation based PEEP tables toward individualized assessment of recruitability, overdistension, transpulmonary pressure, regional ventilation, and mechanical power.
The 2023 ESICM ARDS guideline strongly supports lung protective ventilation and recommends against prolonged recruitment maneuvers, but does not give a universal recommendation for one PEEP titration strategy (Grasselli et al., 2023). The 2024 ATS guideline, however, conditionally suggests higher PEEP without lung recruitment maneuvers in moderate to severe ARDS and strongly recommends against prolonged recruitment maneuvers (Qadir et al., 2024).
This disagreement is clinically important.
Why? Because PEEP can be protective or harmful depending on the lung.
In a recruitable lung, PEEP may reduce cyclic opening and closing, improve homogeneity, lower dynamic strain, and reduce ventilator induced lung injury. In a poorly recruitable lung, the same PEEP may mainly increase overdistension, dead space, right ventricular afterload, and mechanical power.
Recent PubMed indexed evidence supports this personalized approach.
Electrical impedance tomography guided PEEP titration improves compliance, reduces driving pressure, and lowers mechanical power compared with conventional strategies, although larger trials are still needed before routine outcome based recommendations can be made (Songsangvorn et al., 2024).
The recruitment to inflation ratio is attractive because it can be measured at the bedside, but recent CT validated data show important limitations. In a 2025 study, the R/I ratio had poor diagnostic performance for identifying high recruitability, especially in focal ARDS, although very low values may still help identify low recruiters (Richard et al., 2025).
Esophageal pressure remains physiologically elegant because it separates lung stress from chest wall pressure. This is especially relevant in obesity, abdominal hypertension, pleural effusion, and extrapulmonary ARDS. However, it requires technical expertise and should not be treated as a simple number.
The future of PEEP titration will probably not be one method, It will be an integrated bedside phenotype.
The key question is no longer: “What PEEP gives the best PaO₂?”
The better question is:
At this PEEP, is the lung being recruited, protected, or injured?
References📚
*Grasselli, G., Intensive Care Medicine, 49, 727–759. https://t.co/67nFMfpurf
*Qadir, N., American Journal of Respiratory and Critical Care Medicine, 209(1), 24–36. https://t.co/Cf5W5R79KU
*Songsangvorn, N.. Intensive Care Medicine, 50(5), 617–631. https://t.co/BsnCgclUEZ
*Pavlovsky, B., Annals of Intensive Care, 14, 1. https://t.co/p51IFsuMjn
*Richard, J. C., Critical Care, 29, 220. https://t.co/JZp9cxdsKn
🫀🤓Pressure does not move blood. Energy does.
This outstanding review challenges one of the most deeply rooted concepts in haemodynamic management: the idea that pressure variables are the primary drivers of circulation. Instead, the authors propose a physiology framework where the heart supplies energy, the vasculature defines constraints, and pressures merely reflect system state.
Several concepts deserve special attention for critical care clinicians:
• Mean systemic pressure does not “drive” flow
• Right atrial pressure is a dependent variable, not a therapeutic target
• Venous return depends on inflow acceptance and inlet impedance
• Raising pressure without improving flow may worsen congestion
• Shock should be interpreted as either impaired venous delivery or impaired cardiac acceptance
Clinically, this framework helps explain why:
• CVP-guided fluid loading often fails
• Vasopressors may normalize MAP without restoring perfusion
• Congestion can coexist with preserved arterial pressure
• Flow responsiveness matters more than static pressure targets
One of the strongest messages of the paper is simple but powerful:
“Pressure is not perfusion.”
For intensivists, anesthesiologists, and cardiogenic shock teams, this review is worth reading in full. It reconnects bedside haemodynamics with first-principles physiology.
Miller A, Anaesthesia. 2026. https://t.co/ejjvREUe7c
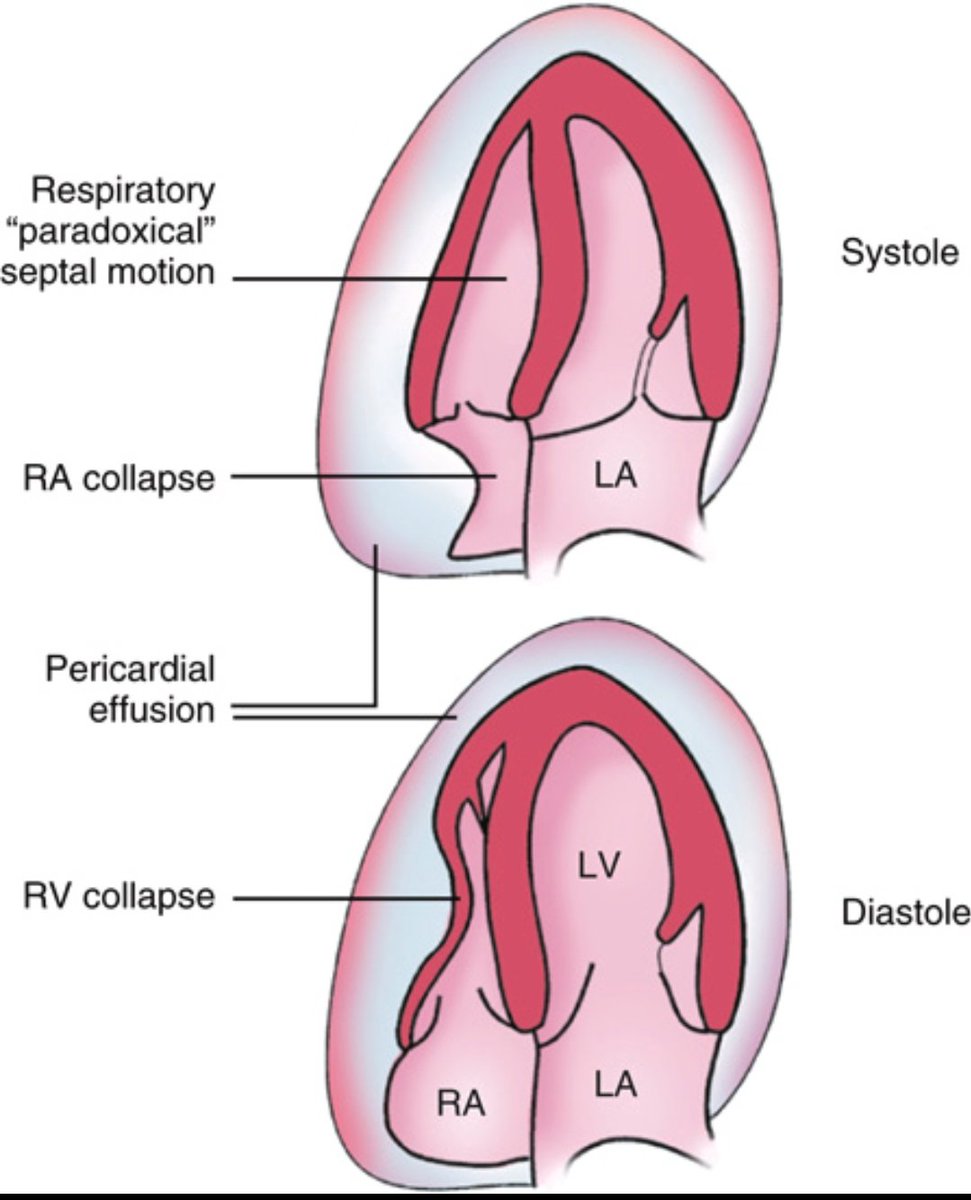
Cardiac Tamponade on 2D Echo
Key findings in tamponade physiology:
🫀 RA collapse in systole
🫀 RV collapse in diastole
🫀 Paradoxical septal motion due to ventricular interdependence
🫀 Pericardial effusion compressing the heart
Peter Stewart changed how we think about acid–base.
He reduced it to 3 independent variables:
Strong Ion Difference (SID)
Total weak acids (Atot: albumin, phosphate)
PCO₂.
Everything we care about — pH, bicarbonate, base excess — just responds to changes in those three.
Why this matters for fluids:
0.9% saline has SID ≈ 0 and a very high chloride. Large volumes drive hyperchloremic metabolic acidosis.
“Balanced” crystalloids keep SID closer to plasma and use metabolizable anions (lactate, acetate, gluconate) instead of so much chloride.
And potassium?
Saline can worsen K⁺ by causing acidosis and pushing K⁺ out of cells.
Balanced fluids often lead to less hyperkalemia despite a small K⁺ content in the bag.
So when you’re on call and hitting “fluid bolus”:
Don’t ask “What’s the pH of this bag?”
Ask “What does this do to SID?”
👉 Want to go deeper into fluids, SID and real‑life cases?
Join our International Fluid Academy online courses and community: https://t.co/j2WZrHw4yq
🫄🏻Airway management in critically ill patients with obesity is not simply a “difficult airway” problem.
The classic airway mindset often focuses on:
• Mallampati score
• neck circumference
• glottic view
• laryngoscopy technique
Patients with obesity experience:
📉 reduced functional residual capacity (FRC)
📈 increased oxygen consumption
📉 shorter safe apnea time
📈 increased work of breathing
📈 higher rates of peri-intubation hypoxemia and cardiovascular collapse
This explains why desaturation during intubation in obesity can become catastrophic within seconds.
The authors strongly support:
✅ noninvasive ventilation based preoxygenation
✅ positive pressure before laryngoscopy
✅ avoiding prolonged apnea
✅ ramped or upright positioning during preoxygenation
The PREOXI trial findings cited in the review are particularly striking: 🫁 NIV preoxygenation reduced hypoxemia dramatically in critically ill patients with obesity compared with standard oxygen strategies.
Another key concept: 📌 positioning is a physiological intervention.
This is not merely ergonomic optimization.
It directly influences:
🫁 diaphragmatic mechanics
🫁 ventilation perfusion matching
🫁 oxygen reserve
🫀 venous return and RV loading conditions
The hemodynamic discussion is equally important.
Critically ill patients with obesity frequently exhibit:
⚠️ right ventricular vulnerability
⚠️ elevated intrathoracic pressures
⚠️ chronic hypoxic pulmonary vasoconstriction
⚠️ preload dependence
This creates a dangerous peri-intubation transition: from spontaneous negative pressure breathing → to positive pressure ventilation.
In unstable patients, that transition alone can precipitate:
🫀 severe hypotension
🫀 RV failure
🫀 cardiovascular collapse
The review therefore emphasizes:
📌 preload assessment
📌 cautious PEEP titration
📌 early vasopressor consideration
📌 careful induction drug selection
Interestingly, propofol emerged as a major modifiable predictor of cardiovascular collapse in prior ICU airway datasets discussed in the paper.
Another strong recommendation: 🎥 videolaryngoscopy should become routine in critically ill patients with obesity.
Not because it looks modern. Because: ✅ first pass success matters.
Every additional attempt:
• worsens hypoxemia
• increases sympathetic stress
• raises aspiration risk
• increases cardiac arrest probability
The review consistently supports:
📌 videolaryngoscopy
📌 stylet or bougie adjuncts
📌 experienced operators
📌 preparation for awake intubation in selected cases
Perhaps the most important lesson from this review:
The obese critically ill airway is not “just harder.”
It is physiologically fragile.
📖 Russotto V et al. Airway management in critically ill patients with obesity. Intensive Care Medicine, 2026. https://t.co/X5l7l4vL5N
Fascinating video featuring some giants of Critical Care Echo, discussing the role of critical care ultrasound in sepsis.
Thanks @echonepean for recording this- and join us in September in London to learn more…
https://t.co/JRdG6WOdQ6
@topmedtalk's @wfsaorg World Congress of Anaesthesiologists (WCA) coverage in Marrakesh continues.
@acumpstey & @katy_skier discuss the management of high-risk surgical patients with anesthesiologists Debra Leung & Duminda Wijeysundera.
https://t.co/MyXUArTlH4
Lung auscultation has been the standard tool for bedside pulmonary diagnosis for 200 years.
What's rarely discussed in clinical training is how poorly it actually performs when tested empirically.
A thread on the evidence.