Real World Data. RWD. Both secular and medical politicians like to ignore RWD. Medicare and Medicaid expenditures and the federal budget. https://t.co/kiJi40LyP9
File under surveillance society. These are the same hospitals that sign NDAs with HMOs to not disclose any process or outcomes data on HMO patients. https://t.co/7OcA6LsSAd
National Post https://t.co/c4ifow45AS via @nationalpost
This goes in my "genocide project" file. There are always a lot of bureaucrats and some doctors who think they know who has a life worth living. Working on a book today, I found an article about health care cost issues from 1989 which quoted an AMA VP saying AIDS patients all die so why spend money treating their pneumonia. Dr. Peter Breggin documented that German doctors were practicing euthanasia of the disabled before and after Hitler. BTW, back in 1989 when I first read that article quoting the AMA VP, I called the AMA and my notes indicate that their response was that the official returned very few calls.
@AnnalsofIM Wonder why the ACP big wigs are suddenly so concerned about MA plans taking over Medicare. This has been a problem for 40 years. BTW name one academic department of internal medicine that is concerned about this. Zero. The professors could care less.
Deductible for echocardiogram is 4x the cash price. But why such a huge charge to insurance for the echocardiogram? Must be the facility fee added on. Hopefully would be much less expensive in a doctor’s office not owned by private equity. https://t.co/gPFmqUIWr9
Courageous attorney explains what is legally and politically important. If it could happen to her client it could happen to you, no matter how much money you have or contribute to the “right” politicians. https://t.co/mtQQhlZzb2
Outcome-Aligned Payments for Technology-Enabled Care https://t.co/CYWJpGtpGp
This is the biggest pile of a hot mess that has been published in a JAMA journal in a long time. Written by an MBA and an attorney no less. They couldn’t find a physician to sign off on this. Meanwhile and sits on almost 3 years of experience in treating Alzheimer’s and mild cognitive impairment data with zero publications.
https://t.co/8O4AdvOprk
Looks like a British national with hantavirus on a remote island gets better access to care than most members of the NHS. Wonder if the U.S. managed care companies running NHS general surgeries will parachute specialists in to relieve any waits for care?
If you think all we need to do in healthcare is let people shop for prices and they will fall, is ridiculous
The number of hospitals and insurance comps walking away from each other, particularly for Med Adv, tell us everything
That the entire HC system is designed to make it IMPOSSIBLE to price shop
Hospitals don't know their costs and can't set prices to insurance companies
Insurance companies do their best to manipulate transactions (latelq, underpay, deny, etc)
All of MA is an attempt by the carriers at arbitrage They bet that they can break the law, and never adhere to reporting regs and the worse that can happen is they might get fined
They bet that hospitals don't know their margins or profits on a per plan or carrier basis and they will make stupid decisions That is starting to change
Now they are using AI to manipulate prices and costs in real time, knowing providers use consultants for Rev mgt, making them unable to respond in months, let alone real time
They bet that by gaming MLR with subsidiaries, they can further break the law and not get caught
Bottom line , it's not an efficient market , due to zero transparency at the transaction level ,and the concept that individuals can shop based on price , when neither hospitals or insurance companies know what their actual costs and prices are , is insane
Carriers manipulate and obfuscate every number they can with the goal of making it impossible to know actual prices
Good luck shopping for prices on all bu the simplest, most obvious services
Totally agree. And it’s also why so many of your local physicians are struggling right now. They’re struggling because they don’t want to work for these behemoths, and yet, they really can’t always compete. These systems generate millions and millions of dollars, and pour a lot of that into marketing.
This is why building a brand using the online space is so valuable. If you rack up followers, they’ll come see you regardless if you work for the local money machine health system.
It’s also why I created @somedocs - so that the public could find the individual physicians that run a health interaction, rather than just get swayed by who the system tells you to see. I built it to provide the publicity and marketing that our peers so badly need, especially those that break off from those systems to practice privately.
https://t.co/4OG6o3FE5r
A study published today in Science may be the most important AI paper in clinical medicine this year. And it happened to land on the same day I submitted a letter to JAMA arguing that AI can already deliver clinically adequate care for defined tasks.
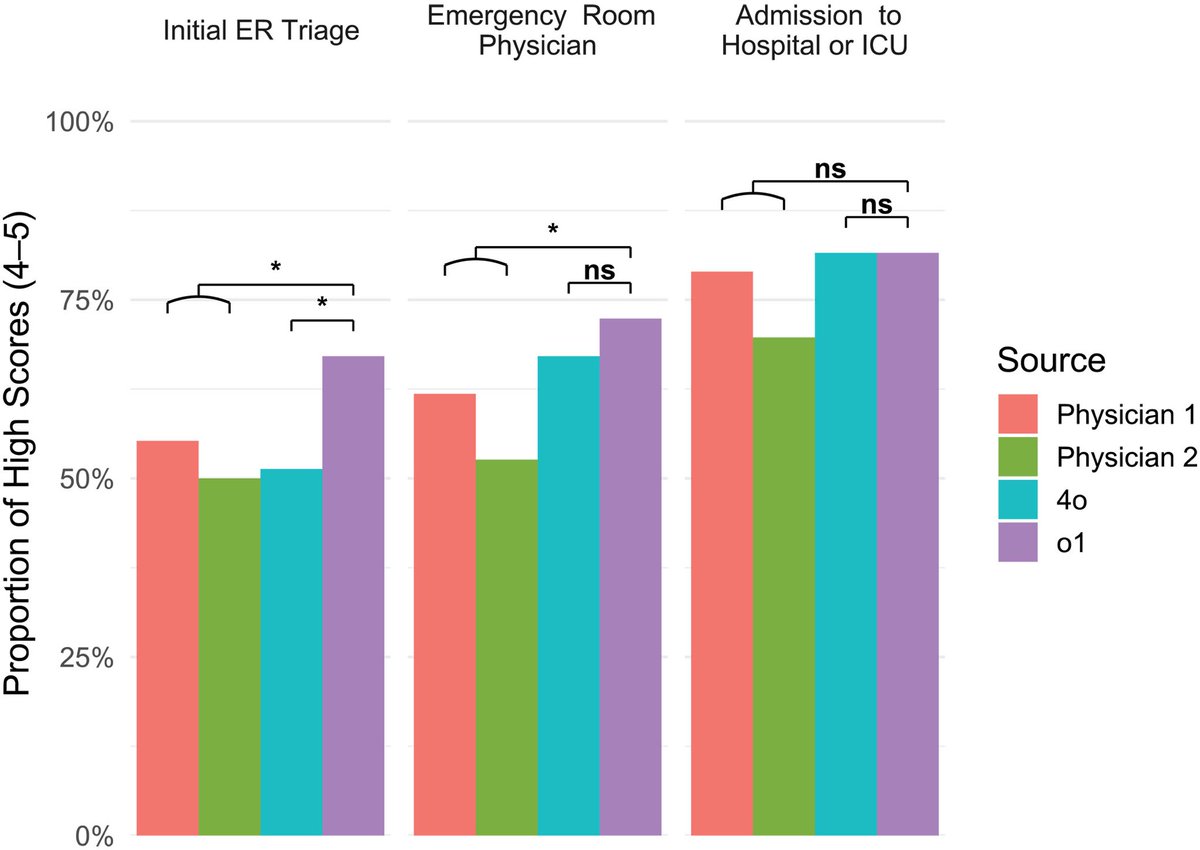
Researchers at Harvard Medical School and Beth Israel Deaconess Medical Center ran six experiments pitting OpenAI's o1 reasoning model against hundreds of physicians across the full spectrum of clinical reasoning: differential diagnosis, management planning, probabilistic reasoning, and clinical documentation. Then they did something most AI studies don't. They tested it on 76 real, unstructured emergency department cases pulled directly from the medical record at a major academic medical center.
The results across all six experiments: the AI outperformed physicians.
On the real ER cases — the messiest, most clinically relevant test — the AI identified the correct or very close diagnosis in 67.1% of cases at initial triage, 72.4% at ER physician evaluation, and 81.6% at hospital admission. The two attending physicians scored 55.3% and 50.0% at triage, 61.8% and 52.6% at ER evaluation, and 78.9% and 69.7% at admission. The gap was widest at initial triage.
On management reasoning using expert-scored clinical vignettes, the AI scored a median of 89%. Physicians with conventional resources scored 34%. That is not a typo.
The physician evaluators were blinded and could not distinguish AI-generated differentials from human ones. One evaluator guessed correctly 15% of the time. The other guessed correctly 3% of the time.
I'm an emergency physician. I work in a rural Texas ED. These are my cases. These are my decision points. And I can tell you that the triage finding is the one that matters most. Triage is where the least information meets the highest stakes — where the wrong call means a patient sits in the waiting room while their sepsis progresses or their STEMI evolves. The AI was 12 to 17 percentage points better than experienced attendings at exactly that moment.
The authors are careful to note this is text-based reasoning only; the AI doesn't see the patient's distress, doesn't hear breath sounds, doesn't read the room. Those are real limitations today. But the cognitive reasoning component of emergency medicine — pattern recognition under uncertainty with incomplete data — is precisely what this model is demonstrating it can do.
This was published in Science. Not a preprint. Not a company blog post. Peer-reviewed, in one of the two most prestigious scientific journals in the world.
The profession needs to stop debating whether AI will be good enough. It needs to start planning for the fact that, for an expanding set of clinical reasoning tasks, it already is.
And yes, this was written with AI. Sorry!!
Houston airport is covered in billboards for nonprofit health systems.
Handsome leaders.
White coats.
Academic prestige.
“Better health.”
Cute.
These are the same institutions that beg the legislature every year for taxpayer dollars while fighting competition, acquiring physicians, inflating prices, and pretending the word “nonprofit” means “public good.”
America does not need more healthcare slogans.
It needs fewer grifter institutions living off taxpayers while making care less affordable.
Shifting even more risk to the sick or worried well. That and a new test to get nursing care from the lowest bidders. Stay healthy. https://t.co/afh5sSMwfx
Medicare affects many aspects of physician care- especially payment.
I just sent this formal letter to the new HHS/CMS Healthcare Advisory Committee ([email protected]), Secretary Robert F. Kennedy Jr., and Administrator Oz.
After 30+ years as an independent neurologist, I had to speak up. Click on link below to see letter:
https://t.co/vGmzOVK3KJ
Accelerating Workforce Well-Being—Lessons From Safety https://t.co/WqxPmXFkWT
Searched on "managed" and "payer." No hits. Designing better systems of care will not cure the evil effects of payers and administrators who tell doctors how to practice to enhance shareholder profits. The professors still don't want to deal with the lethal process that has infected American Medicine for over 40 years. Now people can't find a doctor especially one they can trust.