Rest doesn't protect the arthritic knee... activity nourishes it and has been proven to result in significant pain relief. And... high-intensity running shows the greatest pain relief. Not intuitive at all...
Don't rest your arthritic knee; you're not protecting anything, and you're throwing your general health under the bus.
If you don't tolerate any load... well-- then it might be time to talk to your surgeon.
Your knee is a living, biologically active organ. Cartilage is maintained by cells that respond to their chemical environment, and the primary driver of OA progression is not mechanical grinding.
It is chronic, low-grade inflammation that poisons the environment in which those cells are living.
So we need to stop thinking mechanically and start thinking more biologically. Our cartilage responds favorably to the same stimuli that improve our overall health and wellness.
This is precisely why high intensity exercise in moderate OA (grade 3 of 4) decreases pain and actually increases cartilage thickness.
@PalomaValenciaL Yo quisiera ser médico solo de pacientes sanos. Pero debo atender también a enfermos graves que por su forma de vida están como están. Así los abogados deben servir a quienes son culpables, porque también merecen justicia.
🩺 “Signal does not equal proof.”
Anesthesiologists are closely watching reports from Chile involving rare pediatric neurologic complications after anesthesia and a possible mitochondrial DNA connection: https://t.co/xscLg2tXQv #Pediatrics
Pain isn’t actually “mild” if it never stops. Persistence can turn a small pain into a nightmare. Duration MULTIPLIES the intensity! But we try to quantify #chronicpain intensity without duration? 🤦🏻♂️
https://t.co/H6ORyGlIRB
@GustavoBolivar Eso y más ya se sabía y por eso los elegimos a ustedes. Y qué hicieron? Repetir a diario lo sabido y no hacer nada. Con esto, acabaron con lo poco que teníamos, no acabaron la corrupción ni mejoraron el sistema. Vergüenza de ustedes y arrepentimiento de nosotros.
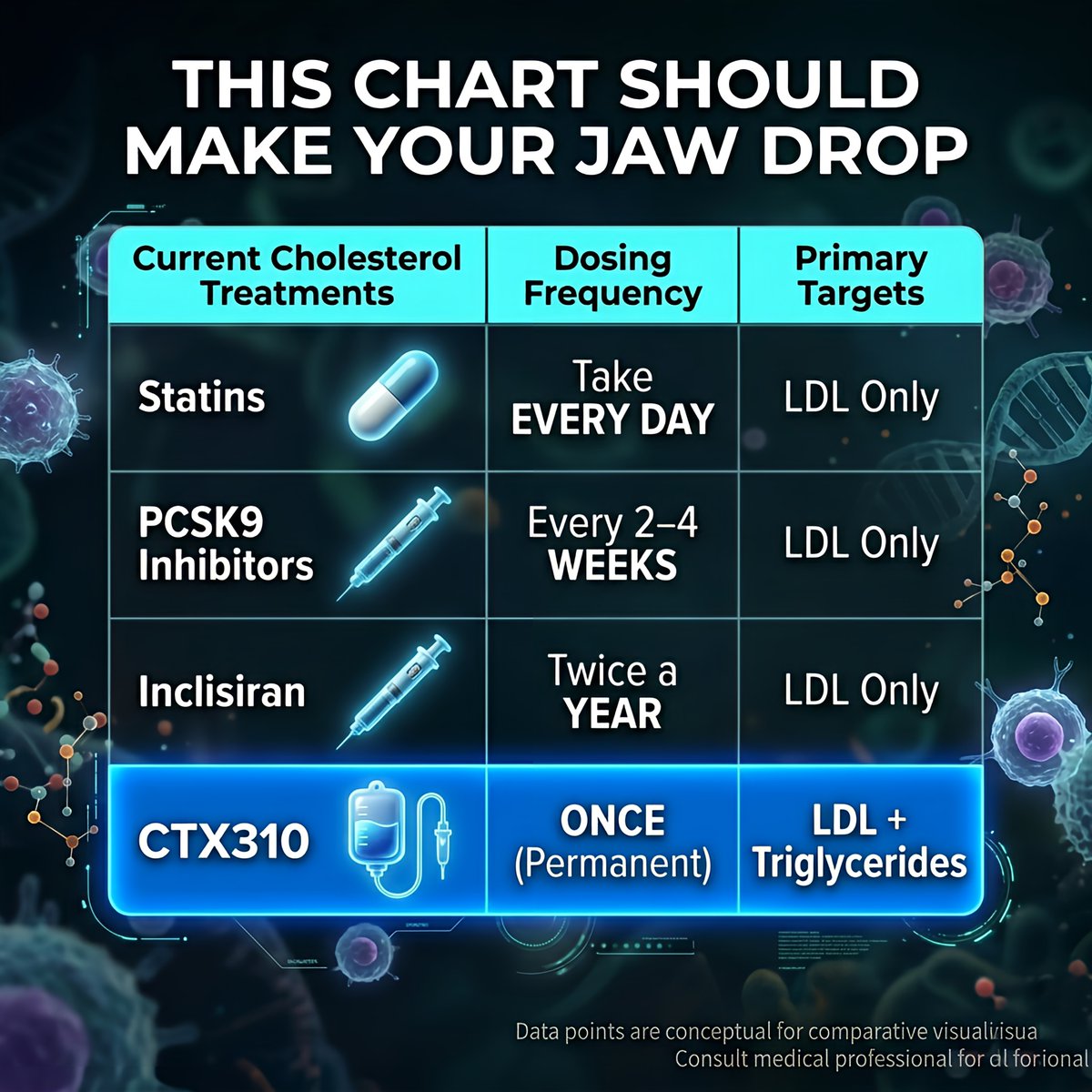
Let me put this in perspective.
Current cholesterol treatments:
💊 Statins → Take EVERY DAY
💉 PCSK9 injections → Every 2–4 WEEKS
💉 Inclisiran → Twice a YEAR
CTX310: 💉 Once.
Possibly FOREVER.
And it's the ONLY treatment that simultaneously drops both LDL AND triglycerides in one shot.
Nothing else does that.
Tengo 38 años.
Cuando era joven, adoraba la política, me volví woke (quebrado) y creí en el mito de la igualdad.
Luego descubrí a Thomas Sowell, y él cambió mi vida para siempre.
12 lecciones del filósofo más controvertido e ignorado de Estados Unidos:
La #suzetrigina es un nuevo #analgésico no opioide que bloquea selectivamente el canal de sodio Nav1.8.
Clínicamente actúa principalmente en la periferia, sobre nociceptores, ayudando a reducir el inicio y la transmisión del #dolor.
#Analgesia#Anestesia
🫁 Lung Ultrasound 2.0, From Art to Science
The new international consensus on lung ultrasound marks a clear transition:
👉 From qualitative interpretation
➡️ To standardized, reproducible, and quantitative medicine
⚠️ What is truly NEW in this update
🔴 1. Standardization is now mandatory, not optional
LUS is highly operator- and machine-dependent
👉 The same patient can generate different findings depending on settings
New recommendation:
• Always report probe, frequency, MI, depth, protocol
• Move toward reproducible imaging frameworks
🧠 2. B-lines are no longer “simple artifacts”
They are:
• Frequency-dependent
• Physically complex
• Linked to lung microstructure
👉 Counting B-lines is semi-quantitative at best
➡️ Future: quantitative ultrasound spectroscopy
🤖 3. AI enters LUS, but with caution
AI is emerging in:
• Image segmentation
• Severity scoring
• Pattern recognition
BUT:
👉 Strong warning against overinterpretation and poor methodology
Key requirement:
• Proper dataset splitting
• Standardized acquisition
• Clinical validation
⚙️ 4. Multidisciplinary shift
This is not just a clinical update
👉 Engineers + physicists are now part of the consensus
Why?
• Ultrasound physics matters
• Signal processing matters
• Image formation matters
➡️ LUS is now a true bioengineering field
📊 5. From subjective to objective metrics
Major gap identified:
• Pleural line abnormalities
• Subpleural consolidations
• Artifact interpretation
👉 Need for:
• Measurable parameters (mm, not “small/large”)
• Quantitative imaging endpoints
🛑 6. Safety is finally addressed
New concern:
👉 Potential pulmonary capillary hemorrhage (animal data)
Recommendation:
• Apply ALARA principle
• Monitor Mechanical Index (MI)
• Limit exposure time
➡️ LUS is safe, but not risk-free
📚 7. Education becomes a core pillar
Clear statement:
👉 LUS must be formally taught and standardized
Including:
• Medical curriculum integration
• Structured training
• Remote mentoring
🎯 Take-home message
Lung ultrasound is evolving from:
❌ Operator-dependent bedside tool
✅ Standardized, physics-driven, AI-supported diagnostic modality
⚖️ My reflection
We are entering a phase where:
👉 Understanding how ultrasound interacts with lung tissue
is as important as interpreting the image itself
This is where critical care, cardiology, and engineering finally meet
📖 Libertario D et al J Ultrasound Med 2023
doi:10.1002/jum.16088
#LungUltrasound #CriticalCare #POCUS #MedicalAI #ICU #Ultrasound #PrecisionMedicine #ACVC
Optimising positive end-expiratory pressure in acute respiratory distress syndrome: a narrative review of approaches to titration
CCR Journal Watch
https://t.co/Sp06oA6IDG
Interpretación rápida #VEXUS 🔍
👉🏼Vena hepática
👉🏼Vena porta
👉🏼Flujo intrarrenal
👉 A mayor pulsatilidad y alteración del patrón → tendencia a mayor congestión venosa, siguiendo puntuación VEXUS.
#PediatricaSEDAR 👶📚
Artículo de revisión: El futuro del manejo de la vía aérea pediátrica.
Una lectura imprescindible para estar al día en los avances y retos en este campo.
🔗 https://t.co/2wOHqGrNrY
A study in NEJM demonstrated no difference in 28-day mortality between patients undergoing emergency tracheal intubation with ketamine versus etomidate, indicating that both may be safe options in acute scenarios. Read a summary in the May 2026 SM&A: https://t.co/EHnTTpLwrH