Man I feel for Jared Verse
• A superstar on a Super Bowl contender
• Coached by one of the best coaches in the NFL
• In LA with an MVP quarterback
And now he’s going to Cleveland
Damn..
The Rams saw a divisional rival, who they were neck-and-neck with, WIN the Super Bowl...
And they went, "F*uck that. We're not letting that happen again."
Garrett, McDuffie, Watson.
#ASCO26#leusm#ALL@MDAndersonnews
Long-term follow-up of Hyper-CVAD + sequential blinatumomab ± low-dose fractionated inotuzumab ozogamicin (INO) in newly diagnosed Ph-negative B-ALL demonstrates encouraging outcomes.
🔹 CR: 100% (59/59 evaluable)
🔹 Flow MRD negativity (10⁻⁴): 95%
🔹 NGS MRD negativity (10⁻⁶): 76%
🔹 30-day mortality: 0%
Among patients treated with fractionated INO (n=37), outcomes were notable:
• 3-year EFS 92% vs 74% in the earlier non-INO cohort (p=0.03)
• 3-year OS 100% vs 82% (p=0.007)
While cross-cohort comparisons should be interpreted cautiously, these data support continued evaluation of antibody-based intensification strategies alongside chemotherapy and blinatumomab in frontline Ph-negative B-ALL.
Amable recordatorio:
NO EXISTE LA ESPECIALIDAD DE MEDICINA ESTÉTICA...
La Especialidad es DERMATOLOGIA o CIRUGIA PLASTICA Y ESTETICA..
La medicina estetica son cursillos y diplomados... o sea pinchis nada...
Important EHA2026 data in UHR LBCL 👇
In this large international retrospective cohort of 1,923 ultra–high-risk LBCL pts, HD-MTX did not reduce CNS relapse.
What makes this clinically relevant: baseline imbalance reflects real-world practice—HD-MTX was preferentially used in pts with renal/adrenal, testicular, ≥3 extranodal sites, and many also received IT MTX during chemo (~50% in HD-MTX arm).
Yet, despite this intensified “current CNS prophylaxis strategy,” CNS relapse remained similar:
Any CNSr: 9.3% vs 8.1%
Isolated CNSr: 5.9% vs 5.7%
This challenges the routine reflex of adding HD-MTX for CNS prophylaxis in UHR LBCL.
The next key question:
Will this still hold true in the Pola-R-CHP era? although POLARIX - did not show lower CNS relapse
#EHA2026 #Lymphoma #DLBCL #CNSRelapse #HDMTX #PolaRCHP #Hematology @Charanpreet_14@DrGPrakash@EHA_Hematology
For patients starting Lenalidomide, thromboprophylaxis should be guided by the IMWG and NCCN recommendations using validated risk scores such as IMPEDE VTE Score and SAVED Score.
🩸 All patients receiving lenalidomide-based therapy require VTE risk assessment.
🟢 Low Risk
➡️ No or minimal risk factors
➡️ Aspirin 81–100 mg PO daily
🟠 Intermediate/High Risk
➡️ Any of the following:
• Prior VTE
• Obesity
• Immobility
• Central venous catheter
• High-dose dexamethasone
• Anthracycline-containing therapy
• Use of erythropoiesis-stimulating agents
• Active infection
• Cardiac disease
• Recent surgery
• Known thrombophilia
➡️ Preferred prophylaxis:
• Apixaban 2.5 mg PO BID
• Rivaroxaban 10 mg PO daily
• Enoxaparin 40 mg SC daily
• Warfarin (INR 2–3) if other options are unsuitable
🔴 Very High Risk
➡️ Recent VTE or strong thrombophilia
➡️ Therapeutic anticoagulation may be required.
⏳ Duration
➡️ Continue while receiving lenalidomide-based therapy or until risk factors resolve.
⚠️ Hold prophylaxis if:
• Platelets <50 × 10⁹/L (individualize)
• Active bleeding
• Severe coagulopathy
💎 Clinical Pearl
Lenalidomide + dexamethasone substantially increases VTE risk; aspirin is acceptable only for truly low-risk patients.
📚 Key Guidelines
📌 National Comprehensive Cancer Network Multiple Myeloma Guidelines
📌 International Myeloma Working Group recommendations
📌 Sanfilippo KM et al. J Clin Oncol. 2019 (IMPEDE VTE)
#MultipleMyeloma #Lenalidomide #Revlimid #VTE #Thromboprophylaxis #IMPEDE #SAVED #Hematology
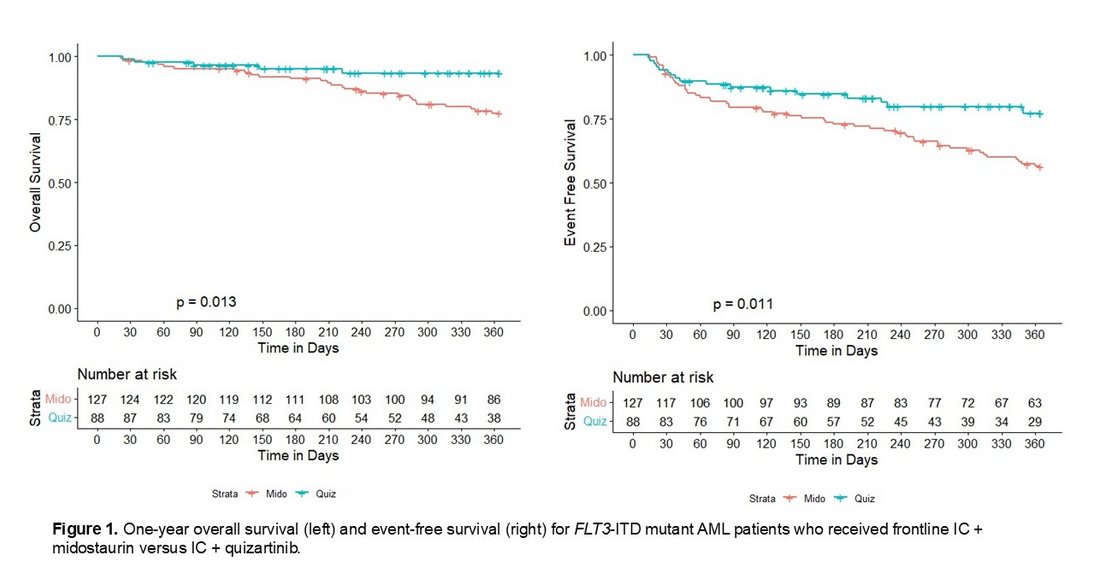
INTENSIVE CHEMOTHERAPY IN COMBINATION WITH QUIZARTINIB VERSUS MIDOSTAURIN FOR FLT3-ITD MUTATED ACUTE MYELOID LEUKEMIA: A MULTICENTER COHORT STUDY https://t.co/g8V9rTfCfo #AML#leusm#EHA26
We recently discussed t(11;14), t(4;14), and t(14;16).
Today—let’s simplify what matters most at the bedside:
👉 t(11;14) = “Leaky myeloma” 💧
👉 t(14;16) = “Sticky myeloma” 🧲
Yes… leaky vs sticky.
💧 t(11;14) — LEAKY
• CD56 negative → no adhesion
• Cells don’t stay in marrow → spill into blood
• PB involvement, EMD more common
🧠 Think:
No glue → no home → they wander
🎯 Biology: BCL-2 dependent
→ Target the protein (venetoclax)
🧲 t(14;16) — STICKY
• MAF → adhesion molecules + IL-6 signaling
• Early disease: locked in marrow niche
• Protected, hidden, therapy-resistant
🧠 Think:
Glued in place… safe for now
💥 Then evolution happens:
→ Lose niche dependence
→ Break out → aggressive EMD
🎯 The big difference:
• t(11;14) → escapes early
• t(14;16) → escapes late… and worse
⚡ Clinical translation:
• Leaky → target the vulnerability (BCL-2)
• Sticky → disrupt the environment + multi-agent therapy
🧠 If you remember one thing:
💧 If it leaks → shut the valve
🧲 If it sticks → break the niche
✍️ Dr Fun + G
#myeloma #hemetwitter