@orthobullets It’s best to let us know any bowel/bladder/perineal symptoms
If none-
“Bone health” evaluations and Rx as indicated
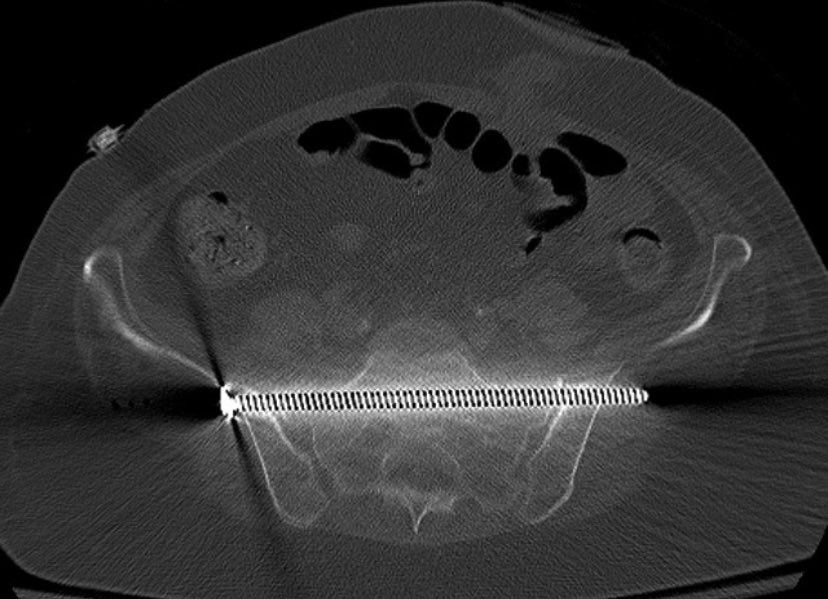
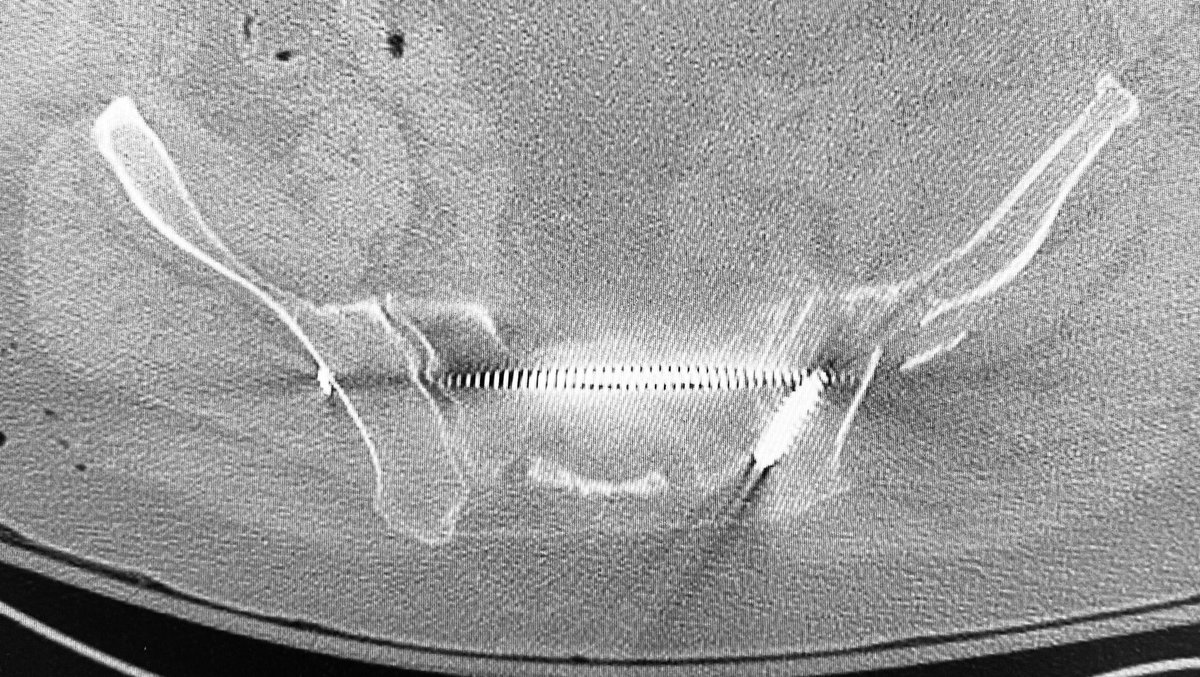
Stabilization of the injury with two trans iliac trans sacral screws
This senior patient developed acute wound swelling 7 days postop. We use the pelvic CT scan to seek info - is it subQ/deep/both? Did the rectusAbd and oblique repairs fail? Did the fixation fail? Are there air densities suggesting infection? This helps us to best prepare/treat.
The CurvaFix pelvic course was a big success yesterday - the 1:2 faculty:participant ratio at the specimens (and each station with its own expert fluoroscopy tech) made a huge educational difference. Strong work.
Preoperative planning considers all factors - body size, bone quality, prior ops, injury details of bone and soft tissues, overall clinical condition, and much more. Integrating and sequencing reductions and implants are crucial for a successful result. Plan excessively -
Houston Orthopedic Trauma Symposium 2026 annual fellowship meeting - day 2 - with Dr. Matt Graves as our visiting professor setting the gold standard - another incredible educational experience
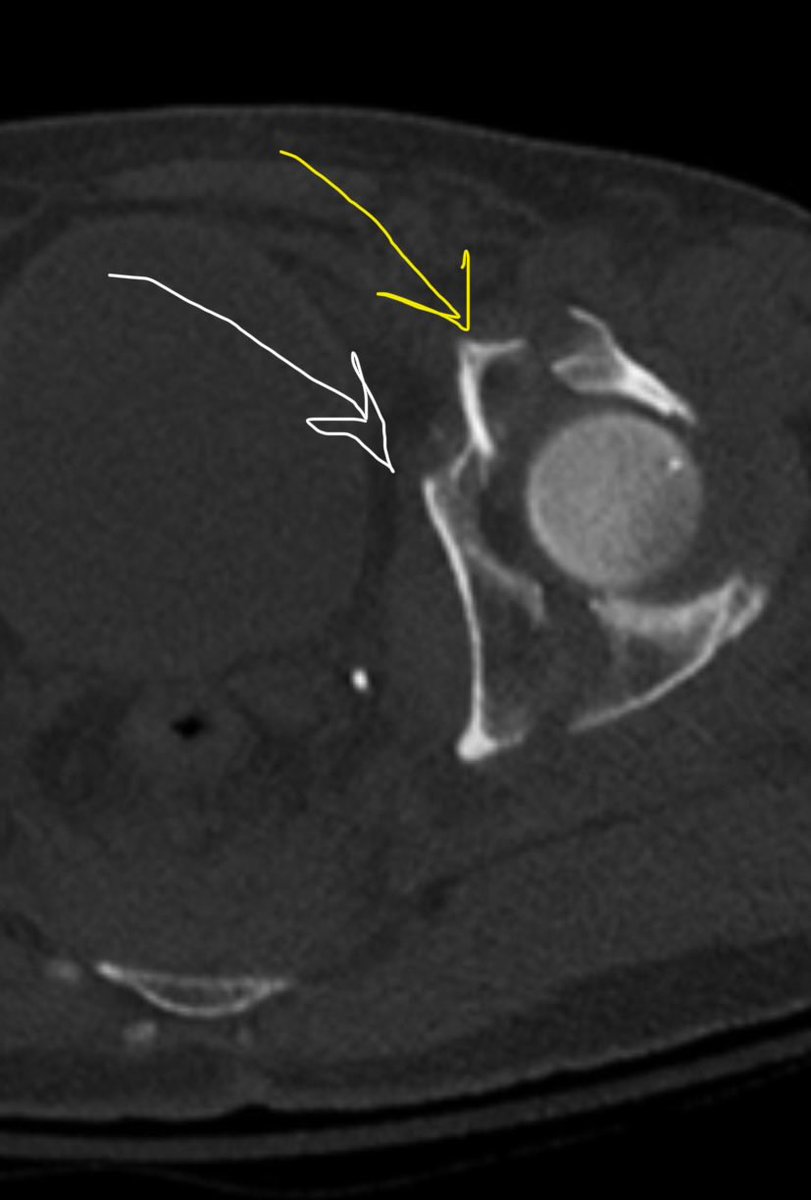
Detailed plans identify frustrating fracture characteristics - like this region - the quad surface fragment impalement must first occur and then be rotated to reduce into its “fracture mate” - like slipping your foot into a tight shoe - this usually requires direct access
The right S1 root was “decompressed” surgically and LPF was added. After this surgery, the radicular pain resolved and the weakness numbness reflex abnormalities were all significantly improved. He had an uneventful rehab and recovery with nerve symptoms/signs resolved.
This young adult has an unstable pelvic ring injury after MVA - he has pelvic pain plus right leg radicular pain, numbness, weakness, and reflex abnormalities specific to the S1 nerve root injury.
The ramus fractures were reduced and stabilized. An iliosacral screw stabilized the sacral fracture. The right S1 nerve root signs and symptoms persisted postop.
6a weekly session - first we go deep detailed on complex sacral fractures with bladder trauma - then we celebrate/bid a Dios to our visiting resident Dr McHorse from Dell UTAustinOrtho - we will miss you!! We learn best together!
Every detail is important to the patient. Screws that penetrate far beyond the cortical surface can be symptomatic. We can avoid this problem with accurate intraop imaging tangential to the landing and exit iliac cortical surfaces. Do you know your implants-how many threads/5mms?
@Davembmd Take great care of your patients and quit worrying about everything else - then if your system is broken, you have 2 options: be a part of the solutions quickly, or eject! Remember to frequently do your own satisfaction score - if it’s not to your liking, you can fix it.