🎉 Match Day is in the books. Matched into federal EM? Welcome to the team. 🫡🔥 GSACEP has a congratulatory packet with your name on it. Fill out the quick survey and we will get it to you. 📦💪
🔗 https://t.co/MNXjeySR2i
#GSACEP#MatchDay2026#ACEPNation#MilitaryMedicine
HOW TO LISTEN AND WATCH
The episode featuring Dr. Sean Stuart is available on YouTube and all major podcast platforms.
YouTube: https://t.co/AorKFWF63M
Apple: https://t.co/p24LA17IqG
Spotify: https://t.co/ihlghUbJlq
I had just finished running the 3-day Government Services Symposium and was literally moving between wrap-up conversations and the next phase when I heard, “Dr. Stuart, I just need you for one minute.” A few minutes later I was back to running around...
Appreciate the WarDocs team for the opprotunity and for what they do.
Episode Title: Navigating Military Emergency Medicine: Leadership, Challenges, and Opportunities with Navy CDR Sean Stuart, DO, MA, FAWM
Blog: https://t.co/6cQLzC94c4
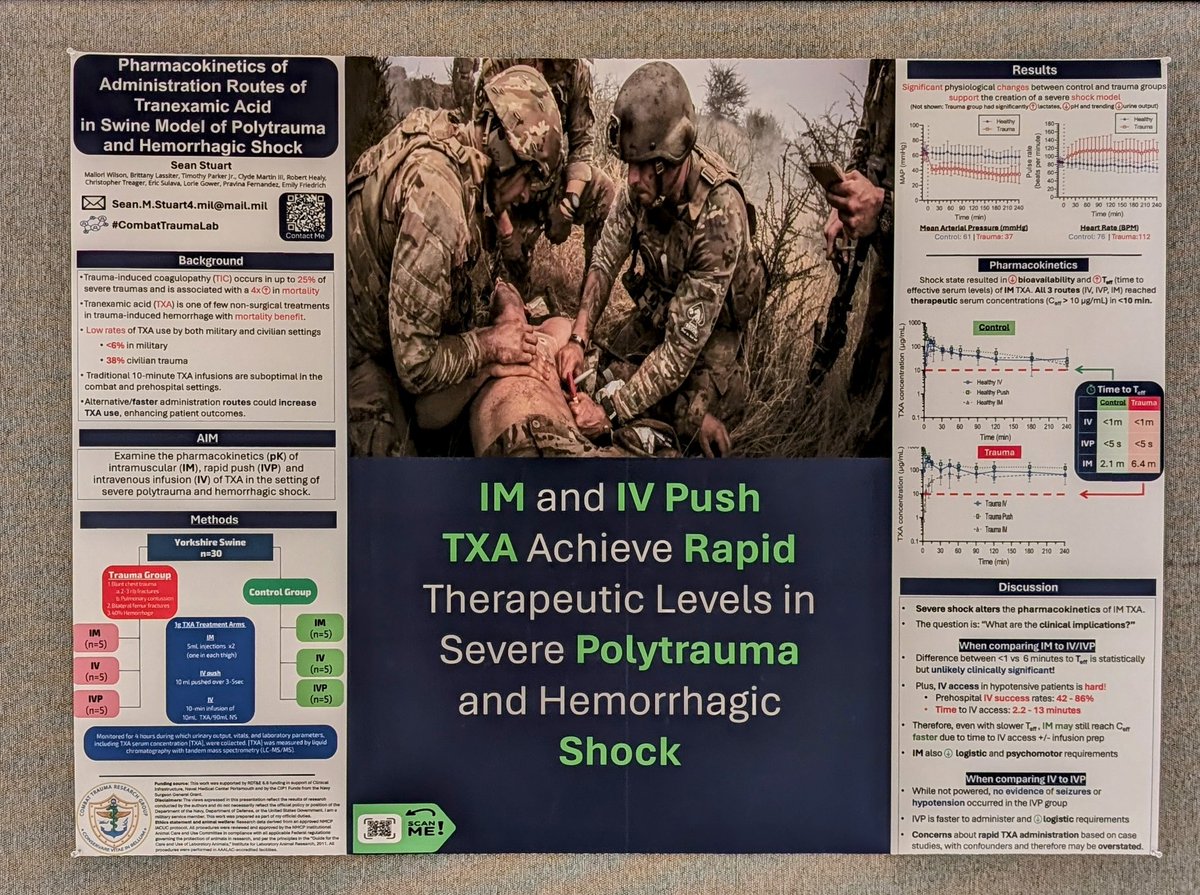
Pharmacokinetics of Tranexamic Acid (TXA) Delivered by Expeditious Routes in a Swine Model of Polytrauma and Hemorrhagic Shock. Prehosp Emerg Care. 2024.
doi: 10.1080/10903127.2024.2342025
⚓Fun fact: Damage control is a term coined by the Navy.
It's important to understand that DCR isn't a single magic bullet. It's a comprehensive strategy, an overarching theme guiding the treatment of critically injured patients.
Needle Decompression & Chest Tube Insertion: A Technique Quick Tip
Always go OVER the rib to access the thoracic cavity.
🚫 Avoids the neurovascular bundle located under each rib.
🦴 Palpate for the ribs before sticking. It's 💯% fine to hit the rib then go over.
📉 Though uncommon, it demands vigilance due to its high mortality rate if untreated.
🧐 Especially after major blasts or trauma, keep a keen eye out. Symptoms might be subtle until they're not.
❓How did your last tension PTX present?
❓ What prompted you to intervene?
📚 Prehospital Extended FAST Exams Improve Clinical Decision Making by Helicopter EMS Crews: A Retrospective Case Series. Prehospital Emergency Care- Feb 2024
❓What do you think of the study?
❓Does U/S have a role prehospital?
Intraosseous (IO) can be great. But many myths exist in regards to what you can use them for. IO are fine for:
1. Blood
2. Fluids
3. Basically just about any medication
4. Lab Draws: Note WBC, K, Na and Ca can be slightly off, butmost other values work just fine.
A brief overview of "Moving the needle on time to resuscitation: An EAST prospective multicenter study of vascular access in hypotensive injured patients using trauma video review."
PMID: 37012624
Does this change your practice?
Remember:
🚫 Not all pneumothorax develops tension physiology
🚫 Not all penetrating trauma have a PTX
🚫 Needle will not fix most causes of shortness of breath/ dyspnea/hypoxia
Needle decompression is a 1 trick 🎠, use it only when needed to prevent doing more harm then good.
Whole Blood – the original lifesaver in our blood product lineup!
It contains every element of blood, making it a balanced option.
Because its "all-in-one" it means we can more rapidly get "all the things" in.
We give less "fillers" (ie citrate anticoagulant and substrate)
⌛Burn shock typically develops over a longer period, think 6-8 hours post-injury.
Therefore, if you see immediate hypotension in a burn victim, it should prompt consideration and evaluation for other potential causes.
📓Protocols vary, but plasma is usually used in conjunction with pRBC as primary volume resuscitation fluids. ❗ RBC: plasma ratios closer to 1:1 = better outcomes.
🤔 If your trauma patient is getting > ~2 units of RBCs, you may want to consider if they may benefit from plasma.
🩸ABO and Rh blood type system are major classifications of human blood based on the presence or absence of specific glycoproteins molecules on the surface of red blood cells. These act as antigens, triggering an immune response if incompatible blood types are mixed.