Dynamic air bronchograms (hyperechoic lines, moving within consolidated lung throughout resp cycle) are an ultrasonographic sign of pneumonia
• Artifact due to air in bronchioles surrounded by consolidated lung
• Up to 94% specificity in differentiating pneumonia vs atelectasis
A right heart thrombus is thin, mobile, and worm-like. It floats to-and-fro within the right-sided chambers.
A vegetation attaches to the valve, usually the proximal side. Its movement is usually chaotic and independent from that of the valve (though not in this case).
Replacing a G-tube is quick if not out too long and no trauma.
Yet, confirmation by gastrograffin x-ray takes forever.
Consider POCUS to confirm placement:
- Place probe adjacent to tube, see catheter and balloon
- Instill 50+ cc of saline, watch stomach expand with bubbles
Evidence suggests that POCUS is superior to the landmark technique for accurately identifying the Cricothyroid Membrane. This may be useful for marking the CTM prior to a difficult anticipated airway (i.e. an obese hypercarbic COPD or opioid intox patient).
How to measure AAA diameter correctly?
- measure outer wall to outer wall, at the widest diameter
- avoid underestimation by only measuring the lumen, always include thrombus / plaque
Dr. Lewis Nelson, NJMS chair of the Department of Emergency Medicine, discusses the dangers of the Gen Z social media trend, BORG, (Blackout Rage Gallon). #RutgersNJMS
https://t.co/90S2ROr9c0
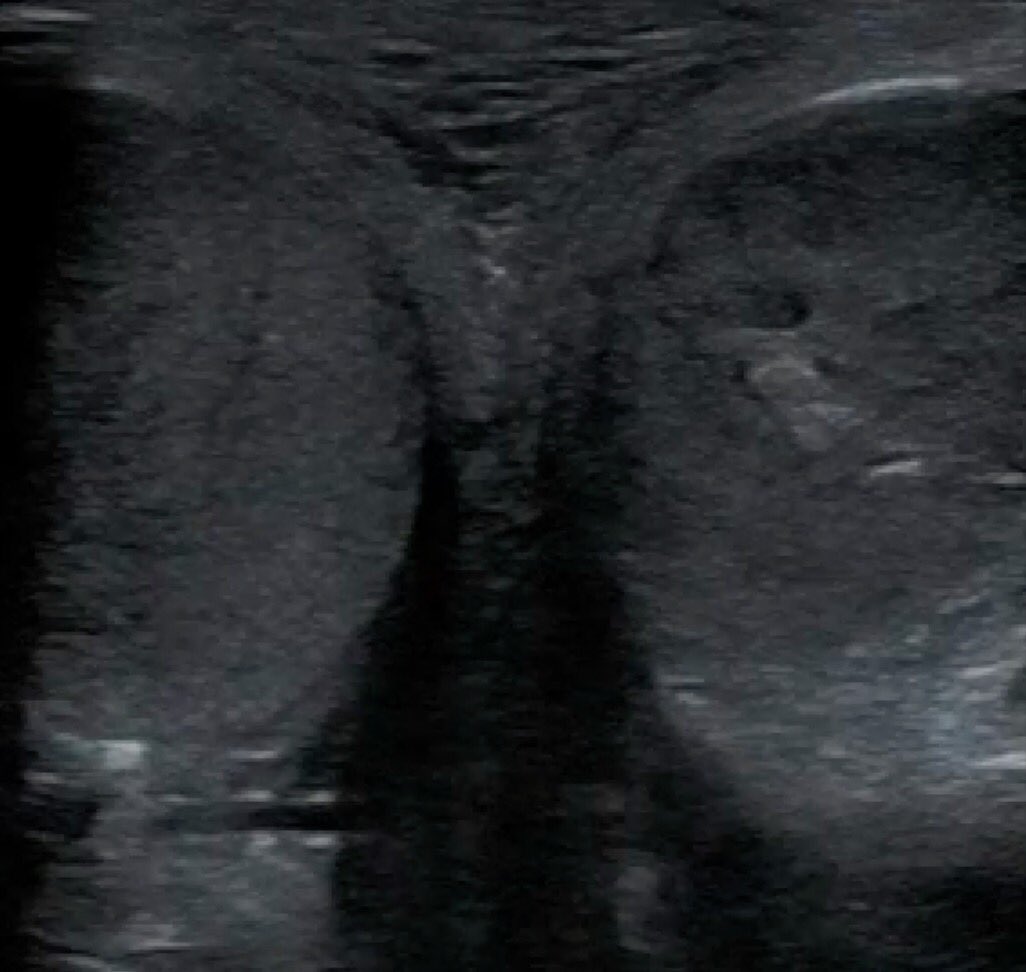
Scrotal sono to r/o torsion:
- linear high-frequency probe
- both testes side-by-side ('buddy shot')
- power doppler to assesses low-flow vessel flow, turn up gain until you see artifact
- edema and change in echogenicity (vs normal homogenous pattern) can take 6+ hrs to develop
US findings in acute appendicitis:
a) Dilated (>6 mm OD), non-compressible, aperistaltic blind ending structure
b) Appendicolith with shadowing
c) Wall Thickening (>2 mm)
Peri-appendiceal findings:
d) Hypoecholic fluid OR
e) Hyperechoic fat with ↑flow
The confirmation of an intra-uterine pregnancy (IUP) in a patient with a positive pregnancy test requires at minimum the visualization of gestational sac AND yolk sac (hyperechoic ring within the gestational sac) on POCUS. Even better to visualize fetal pole +/- fetal heartbeat.
Curtain sign: sonographic lung tissue (i.e. A-, B-lines) moving inferiorly over the diaphragm w/ inspiration, and superiorly just above the diaphragm w/ expiration. Like a "curtain" opening and closing. When present at the lung base, there is no (significant) pleural effusion.
A hip effusion is diagnosed by a fluid stripe greater than 5 mm along the femoral neck or a greater than 2 mm fluid stripe asymmetry when compared to the contralateral hip.
@SAlerhand@IOstrovsky99@annettemdinnyc@drmuellerreport
When there’s NO lower extremity DVT at a given location, vein will fully compress with pressure.
When there IS a DVT, vein will NOT fully compress (attached).
Doppler is not necessary.
An acute clot (attached) usually appears anechoic.
An older clot usually appears echogenic.
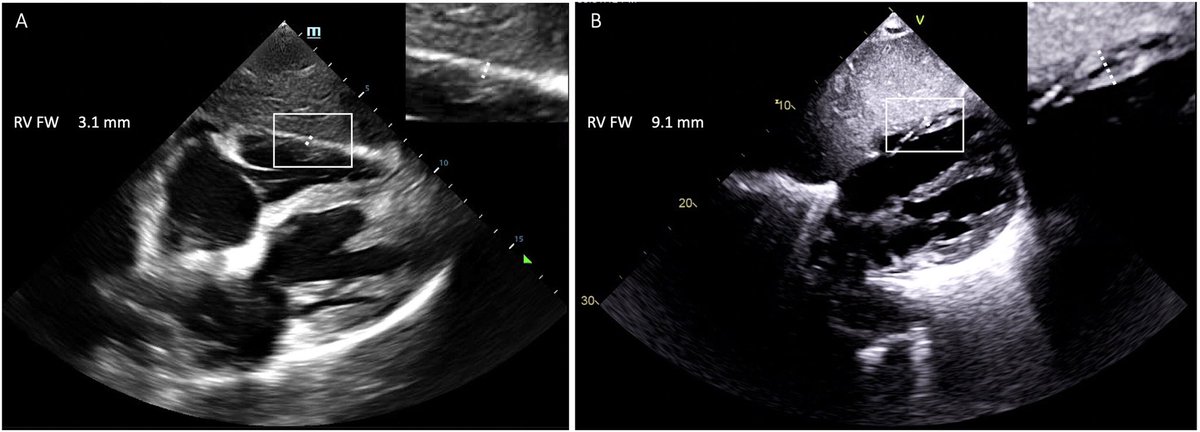
RV hypertrophy suggests chronic RV dysfunction - best assessed from zoom-in SX view.
Chronic dysfunction:
1Qual: RV free wall appears as thick as LV posterior wall (assuming not thinned out by prior MI), and has muscular trabeculations.
2Quant: RV free wall thickness > 5 mm
Pseudoaneurysm (PA): artery leaks pulsatile blood into surrounding tissue, eg 2/2 catheterization or penetrating trauma.
POCUS ying-yang sign: one color is blood flow from artery into PA, other color is blood within the PA that circles back around. Clots in tissue are echogenic.
Unpopular opinion but if a trainee asks you a simple medical question that you can answer in 2 min during rounds plz don’t ask them to look it up themselves when you have the needed information at your immediate disposal. It’s both discouraging and inefficient. Agree? Disagree?