$IBRX 🚨 Massive ANKTIVA Victory! 🚨
Huge congratulations to Brandon on this amazing news! 🙌
Brandon is at @DrPatrickSoonShiong’s clinic receiving #ANKTIVA, and his PET scan from last week delivered incredible results:
✅ No signs of metastasis
✅ No growth in tumor size
✅ Hardly any tumor activity left… meaning it’s dying!
In his own words: “I would not be alive right now had it not been for Dr. Pat and @ImmunityBio.”
This is exactly why we fight for faster access and more patients to get this game-changing immunotherapy. Stories like Brandon’s are the future of cancer care!
Thank you @DrPatrick and @richadcock including the entire ImmunityBio team. Keep delivering hope! @LoriMills4CA42
For those of use who were wondering why Anktiva wont cause the same.
Anktiva (nogapendekin alfa inbakicept-pmln, also known as N-803) is an IL-15 receptor superagonist approved (with BCG) for BCG-unresponsive non-muscle invasive bladder cancer (NMIBC). It is administered intravesically (directly into the bladder). It does not typically cause a significant cytokine storm (cytokine release syndrome, or CRS) like CAR T-cell therapy for several key reasons. https://t.co/ieFhR7cm6j
1. Localized Delivery Limits Systemic Effects
Anktiva is instilled directly into the bladder via catheter, rather than given intravenously or systemically. This confines its primary action (and immune activation) to the local tumor microenvironment in the bladder. Minimal systemic absorption occurs, reducing the chance of widespread cytokine release that drives CRS in therapies like CAR T, where billions of activated cells circulate throughout the body. https://t.co/1rvcSgWPp7
2. Different Mechanism: Targeted IL-15 Stimulation vs. Massive T-Cell Activation
• CAR T therapy involves infusing large numbers of engineered T cells that rapidly proliferate and engage tumor antigens systemically. This triggers a massive release of cytokines (e.g., IFN-γ, TNF-α, IL-6) from the CAR T cells themselves, plus activation of bystander cells like macrophages in a positive feedback loop—especially with high tumor burden.
• Anktiva is a fusion protein complex (IL-15 mutant + IL-15Rα + IgG1 Fc) that acts as an IL-15 superagonist. It mimics dendritic cell presentation to selectively promote proliferation and activation of NK cells, CD8+ killer T cells, and memory T cells (while avoiding strong stimulation of immunosuppressive Tregs). IL-15 signaling supports effector and memory responses with less broad, uncontrolled inflammation than IL-2 or direct massive T-cell receptor engagement. https://t.co/ieFhR7cm6j
IL-15 generally has a more favorable safety profile than high-dose IL-2 (which is notorious for capillary leak and toxicity). It drives targeted immune memory and tumor killing without the same degree of systemic hyperactivation. https://t.co/KU24wWvaXy
3. Clinical Evidence Shows Low Systemic Toxicity
In trials and real-world use:
• Common side effects are mostly local (e.g., painful/frequent urination, blood in urine, bladder irritation, UTI) or mild systemic (chills, fever, fatigue, musculoskeletal pain).
• No significant CRS or cytokine storm is reported as a notable adverse event. Even in systemic or combination studies (e.g., with checkpoint inhibitors), the adverse event profile was consistent with the backbone therapy, with no CRS observed and low rates of severe events. https://t.co/ieFhR7cm6j
• Grade 3/4 events are uncommon (0–3% in some maintenance settings), and treatment is generally outpatient and well-tolerated.
Summary of Key Differences
• CAR T: Systemic, antigen-driven massive T-cell expansion + feedback loop with macrophages/endothelium → high risk of CRS (often >50–75% of patients).
• Anktiva: Localized intravesical IL-15 superagonist → controlled activation of NK/CD8 cells with minimal systemic spillover and no strong Treg or broad inflammatory cascade.
This design allows Anktiva to restore immune response (including to BCG) and generate durable complete responses in the bladder while keeping toxicity manageable. As with any immunotherapy, individual responses vary, and patients are monitored, but CRS is not a characteristic concern.
$IBRX thesis: cheaper, scalable, longer-lasting NK cells with patent protection.
if m-ceNK works at scale, this becomes bigger than one drug.
@grok how different are m-ceNK cells from standard NK therapy?
$IBRX 3!Days after the Approval of Anktiva, Patrick gave this lecture, as an Alum in Soorh Africa. I doubled down, and have waitied for the market to acknowledge the brilliance and commercial reality of IBRX- enjoy to those who never seen this- Going to 💯 and beyond. 🐫🦈🐘🦈 https://t.co/GQE7AmcCoG. Happy 250! We will hot that too and beyond.
@Oshin76@truedat999@Christine_een I think he might sell a piece if it was a strategic investor like the Saudi Investment Fund. That would set a valuation, crush the shorts, and eliminate the concern about liquidity. For the Saudis it would cement the partnership.
Current CAR-T therapy is faced with multiple hurdles-the cost and time it takes to manufacture and most of all the need for patients to undergo chemo and be hospitalized doing so in order to rid the bone marrow of lymphocytes before the CART infusion. This process is called lymphodepletion. The toxic side effects and costs close to a million dollars is not sustainable. At our summit we showed how all of these were overcome! More to come. Immunotherapy 2.0
AI-designed nanobodies + NK cells could become one of the next frontiers in cancer treatment. Dr. Pat highlighted both in Saudi Arabia, with first-in-human AI nanobody trials beginning in the UK. $IBRX is thinking far beyond a single approved drug.
Guess who’s overseas now??
🚨 BREAKING: IRAN WAS MINUTES FROM LAUNCHING HELL ON EUROPE! 🚨
Sen. John Kennedy just dropped the BOMBSHELL classified intel that changes EVERYTHING:
“Our intelligence showed Iran stacking ballistic missiles and killer drones like never before… They were about to turn to America and Israel and SNARL:
‘We’re restarting our nuclear weapons program — and if you try to stop us, we’ll OBLITERATE the Middle East… and oh yeah, our missiles now reach LONDON, PARIS, and GERMANY!’”
Trump faced the nightmare decision: Let them arm up until they could rain fire on our allies and threaten the homeland…
OR STRIKE FIRST AND SAVE THE WORLD?
He chose to BOMB their nuclear sites and STOP THE MADNESS.
This wasn’t politics. This was SURVIVAL.
If Trump hadn’t acted, where would we be right now?
🔥 Drop your thoughts below — Did he save us or not? RT if you stand with strength over surrender! 🇺🇸💥
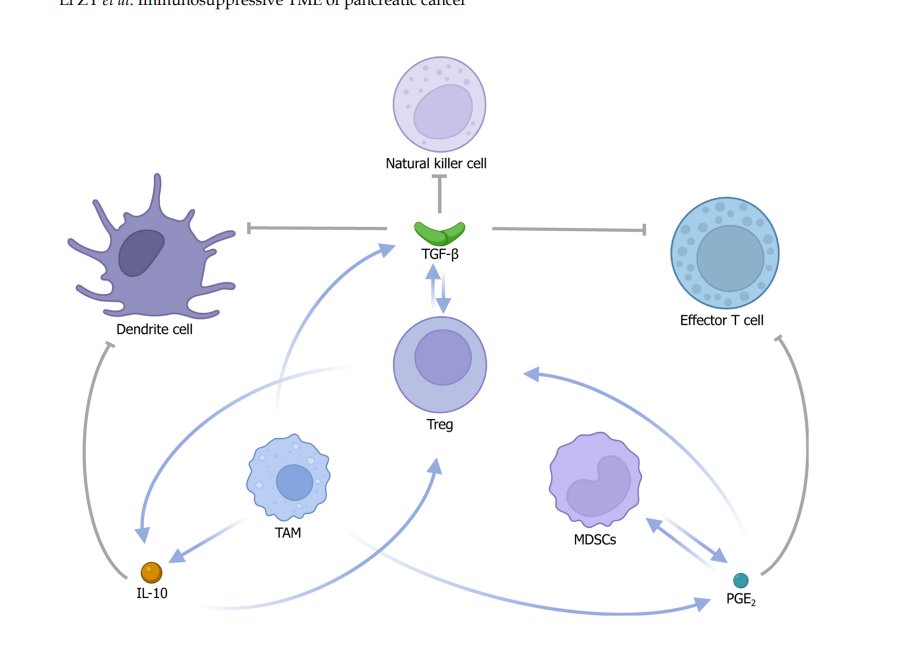
Tumor microenvironment shuts down immune responses against #cancer
You know what fixes the tumor microenvironment?
#Anktiva by $IBRX....thats what
https://t.co/8cGExbmX2y
@DaveScolte Am guessing that Leondaro is already doing this and at minimum working on it. Who says they can't be made from sharks or camels? Nantobodies is what Dr. PSS calls them.
$IBRX there is a freaking goldmine of stuff posted by the Saudis, have to start searching for stuff in Arabic to find it.
Here is a post with 500,000+ views and 100+ comments saying we already deployed our cell robot in King Faisal hospital and it's being marketed to serveral countries.
This is not the first time I seen a lot of action regarding us and this hospital and comments saying we already got something in that hospital.
Why $IBRX is huge? #anktiva activates IL-15 pathway....IL-15 increases ADCC...which means it makes FDA approved antibodies such as #herceptin and rituximab work better....these are billion dollar a year drugs...
@DrPatrick is tha BOSS !
Paper showing IL-15 increases efficacy of #rituximab
https://t.co/KkkVGWHTNn