@srrezaie discussion about Andexanet alfa and it’s use in ICH #resusxreunion2024
Always triple check big Pharma funded studies!! The primary outcome was hemolytic efficacy butshowed increased thrombotic events!!
In PE how to alteplase:
@srrezaie plan of action is to give 10mg bolus then 40mg over 2 hours. The idea is to HALF-DOSE your thrombolysis.
Thus if you are giving 100mg now then give half dose (ie. 50) @srrezaie#resusfest
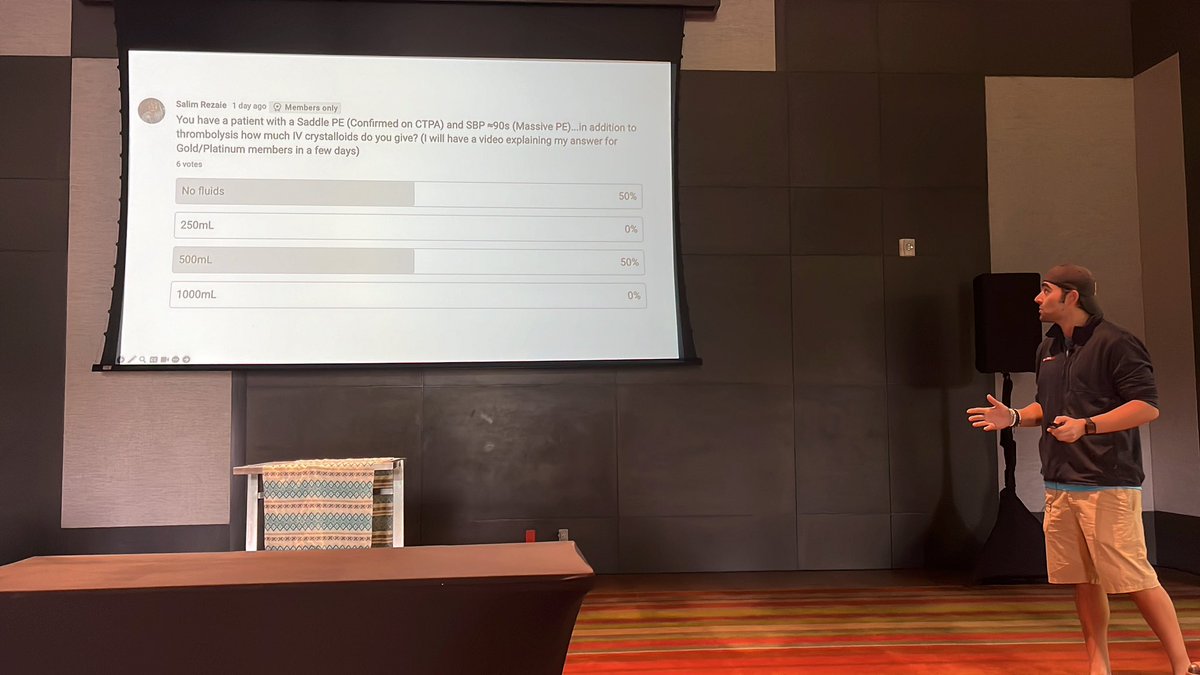
PE is an afterload problem. Hypotension with tachy = cardiogenic shock due to RV strain/failure. Thus giving fluids won’t fix PE spiral of death. PPL who think fluids of 500ml for PE are WRONG. only study of support was in 1999 & not on for massive PE. @srrezaie#resusfest
@srrezaie#resusfest
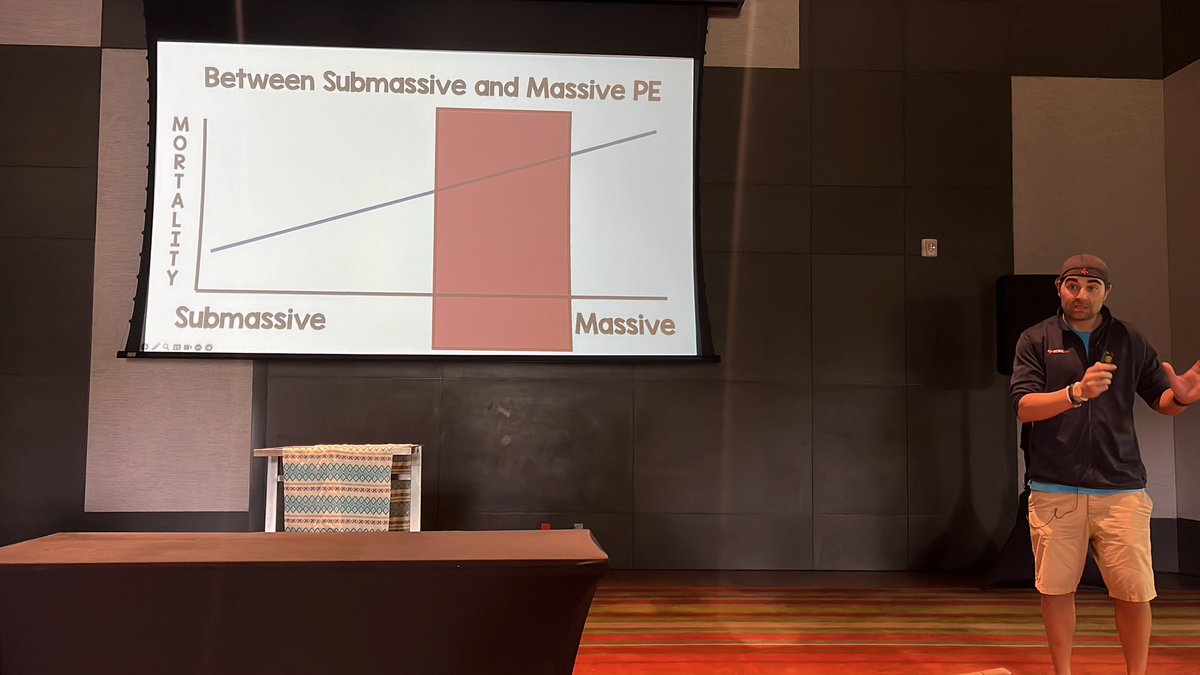
PE categories:
- Incidental
- Segmental
- Submassive (RV looks dyfx= anticoag tx)
- Massive PE (2 types: hypotensive type which don’t look bad and emergency type which look bad)
@gagestuntz#resusfest
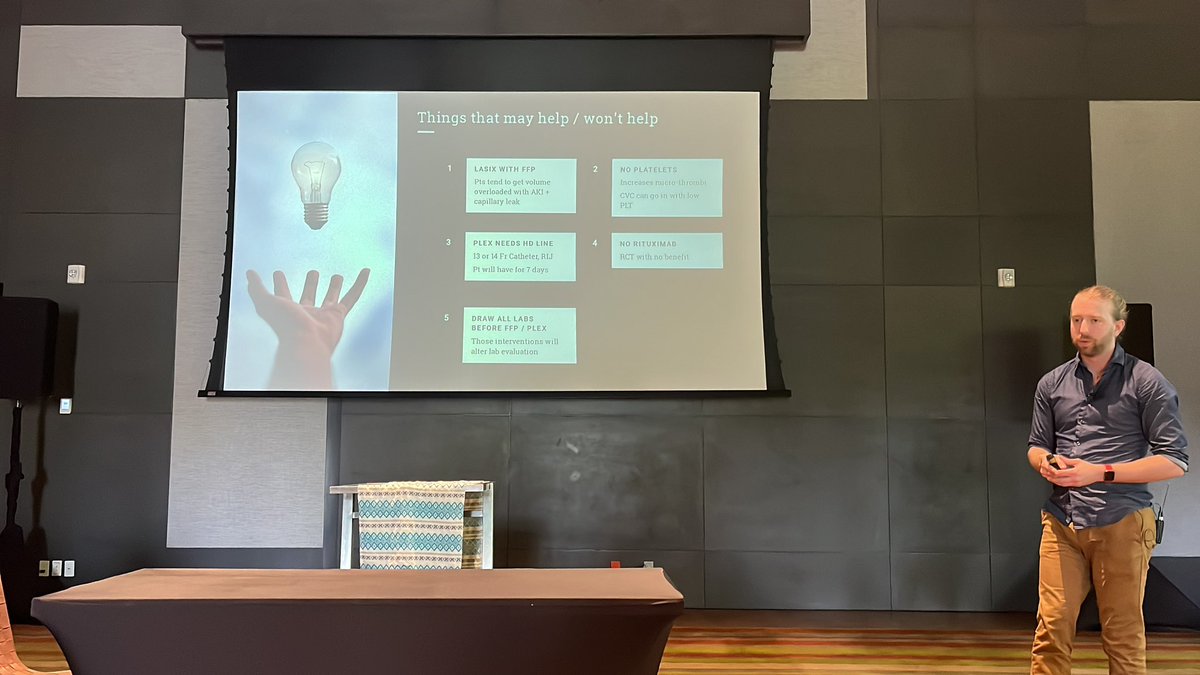
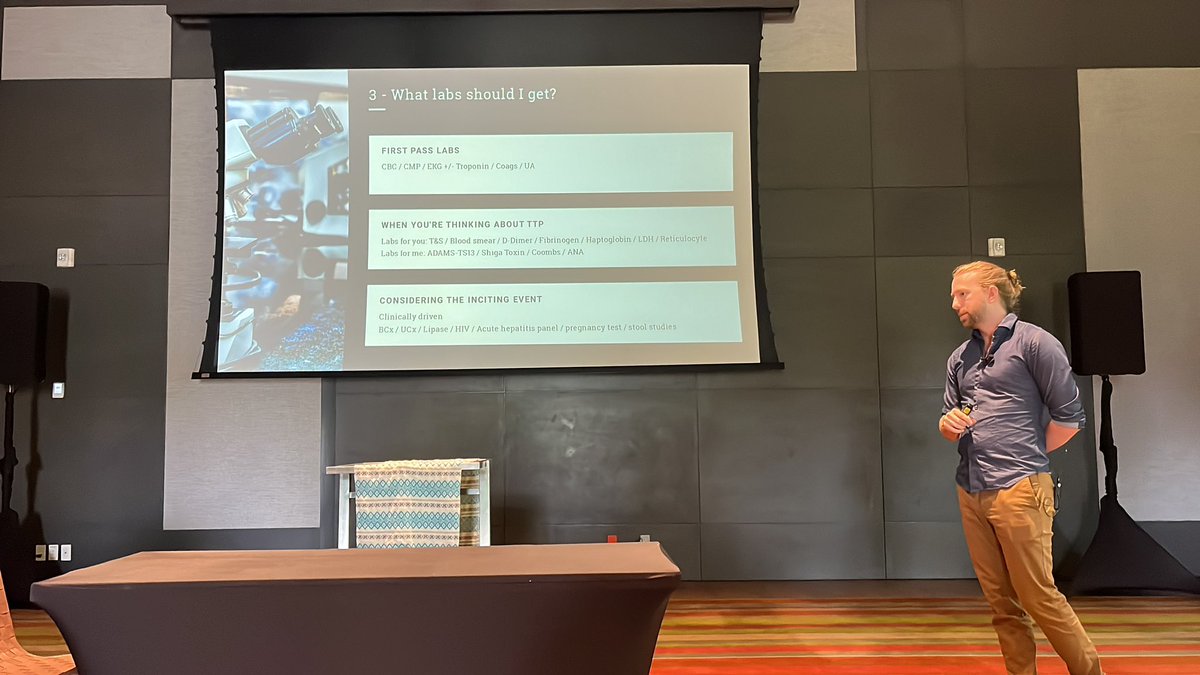
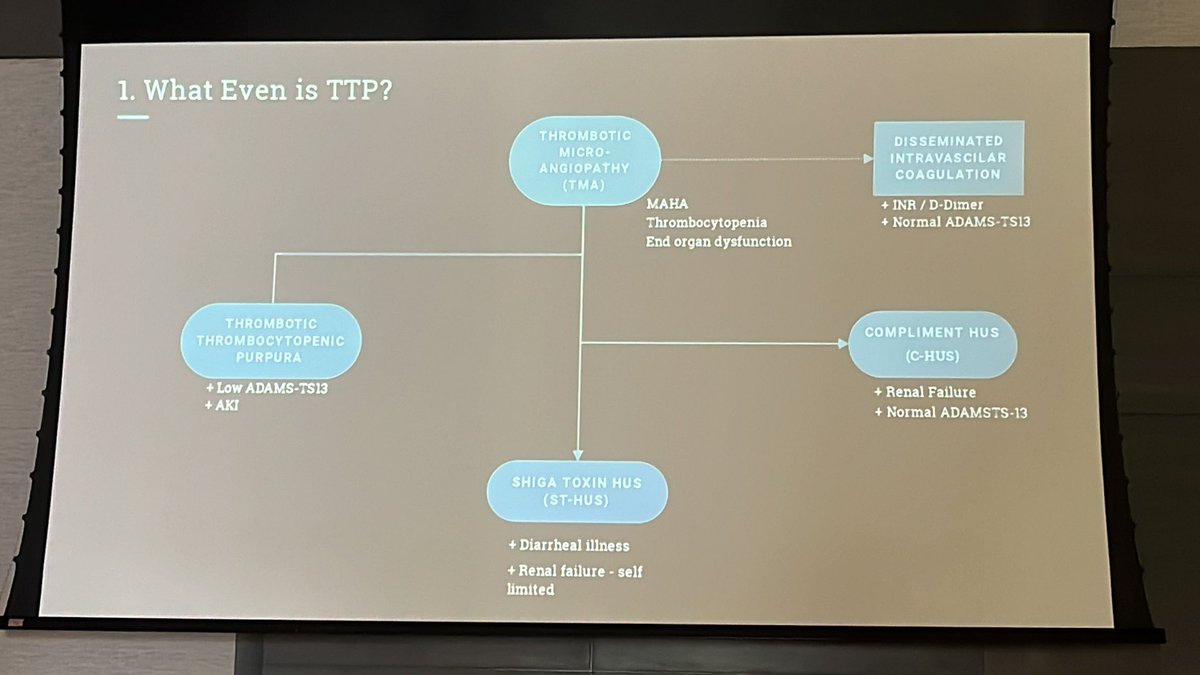
In TTP:
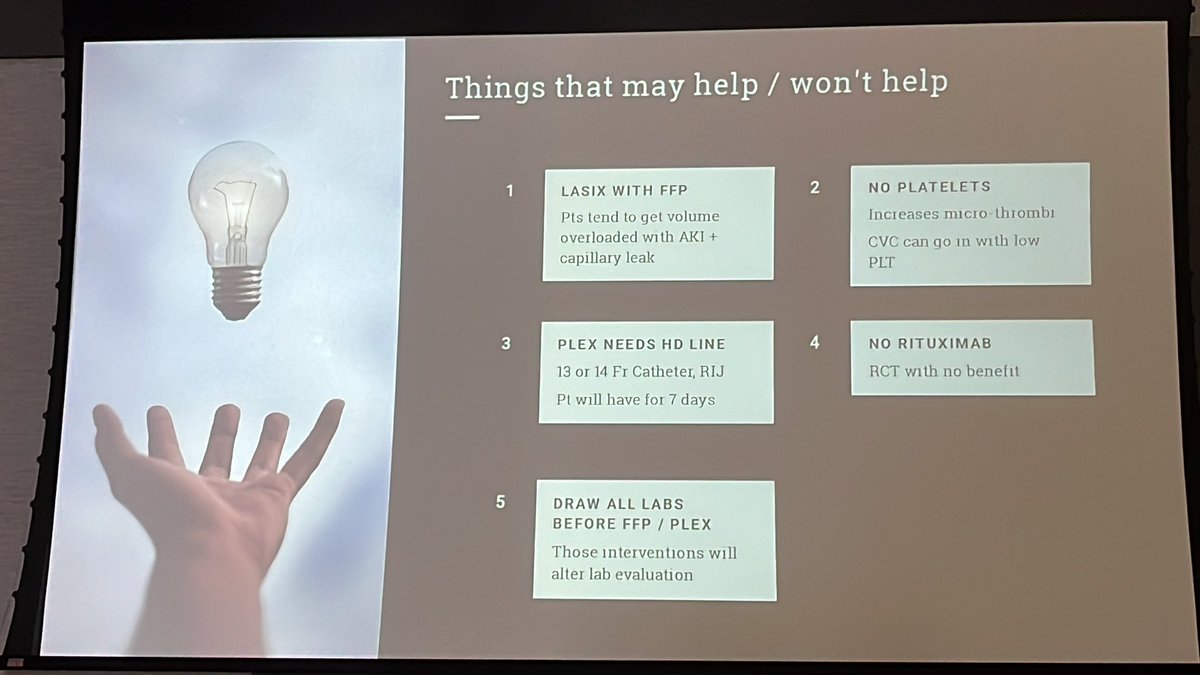
➡️Furosemide can help cuz pt usually are fluid overloaded.
➡️Put a HD line
➡️Draw all labs b4 FFP/PLEX
➡️NO RITUXIMAB or PLT!
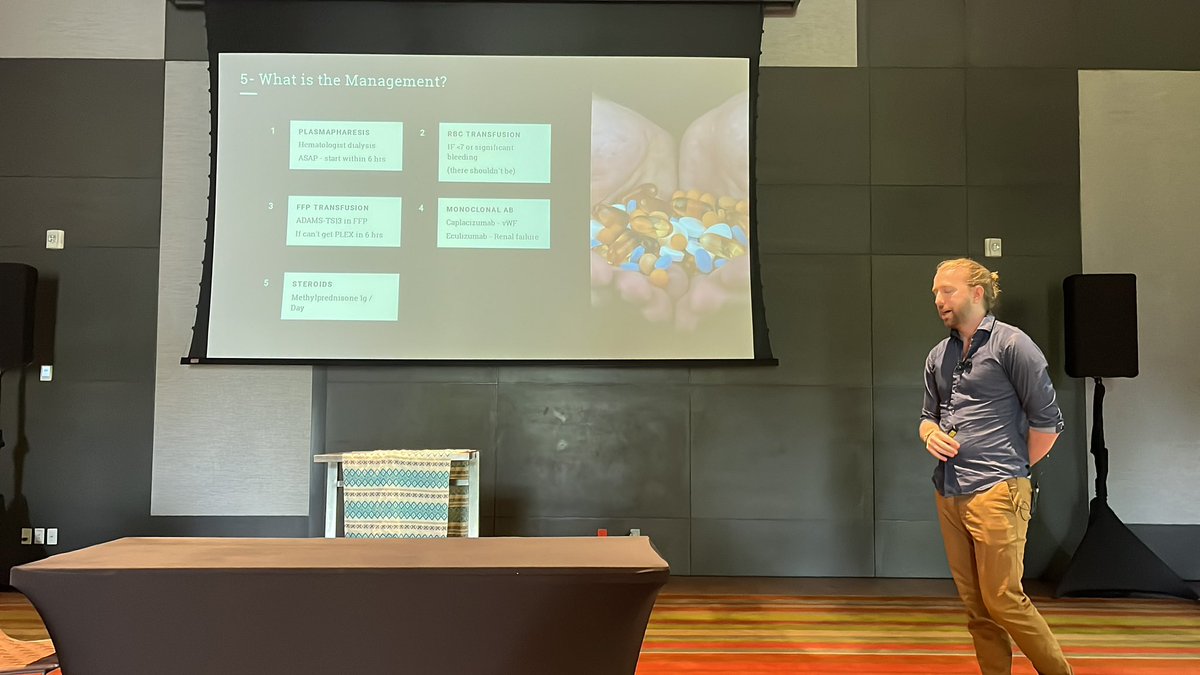
How do you manage TTP? -
1. Plasmapharesis
2. Plasmapharesis
3. Plasmapharesis
4. Plasmapharesis
5. Plasmapharesis
Jk you can also use steroids, FFP/RBC transfusion, or monoclonal AB. @gagestuntz#resusfest
When trying to diagnose TTP feel free to use the plasmid score as a clinical decision tool. Keep in mind that it is not a validated score. @gagestuntz#resusfest
@gagestuntz#resusfest
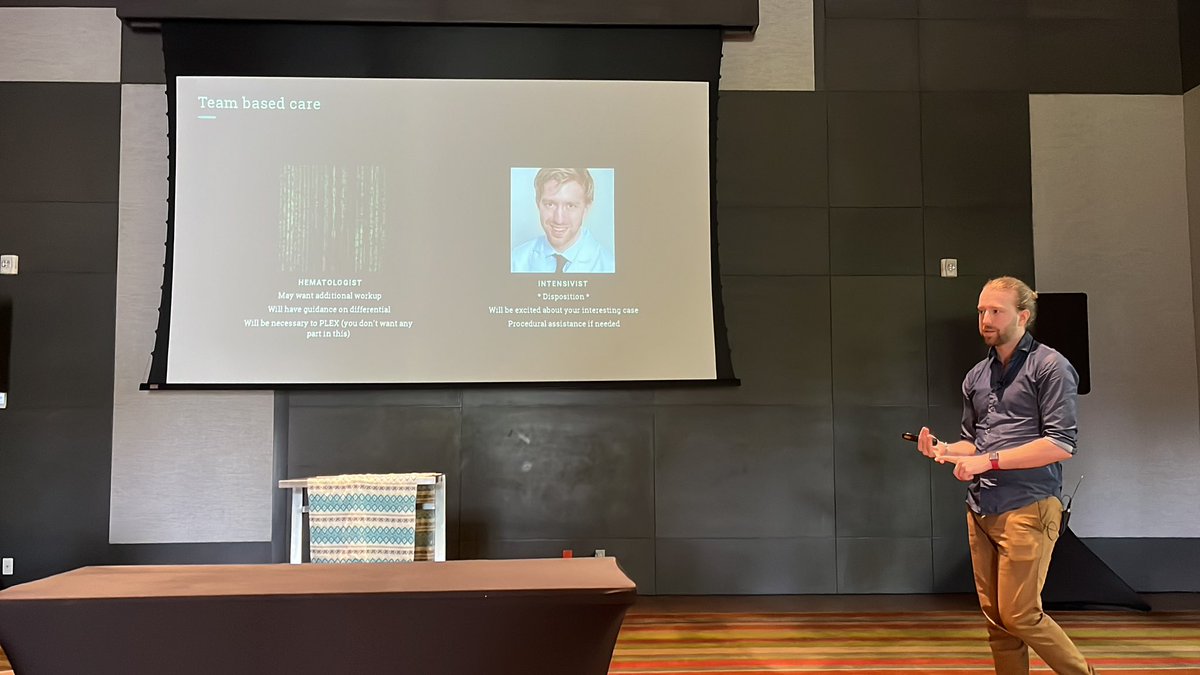
When you suspect TTP, you need to focus on team based care which means having an intensivists and hematologist working with you in the emergency room.
@gagestuntz#resusfest
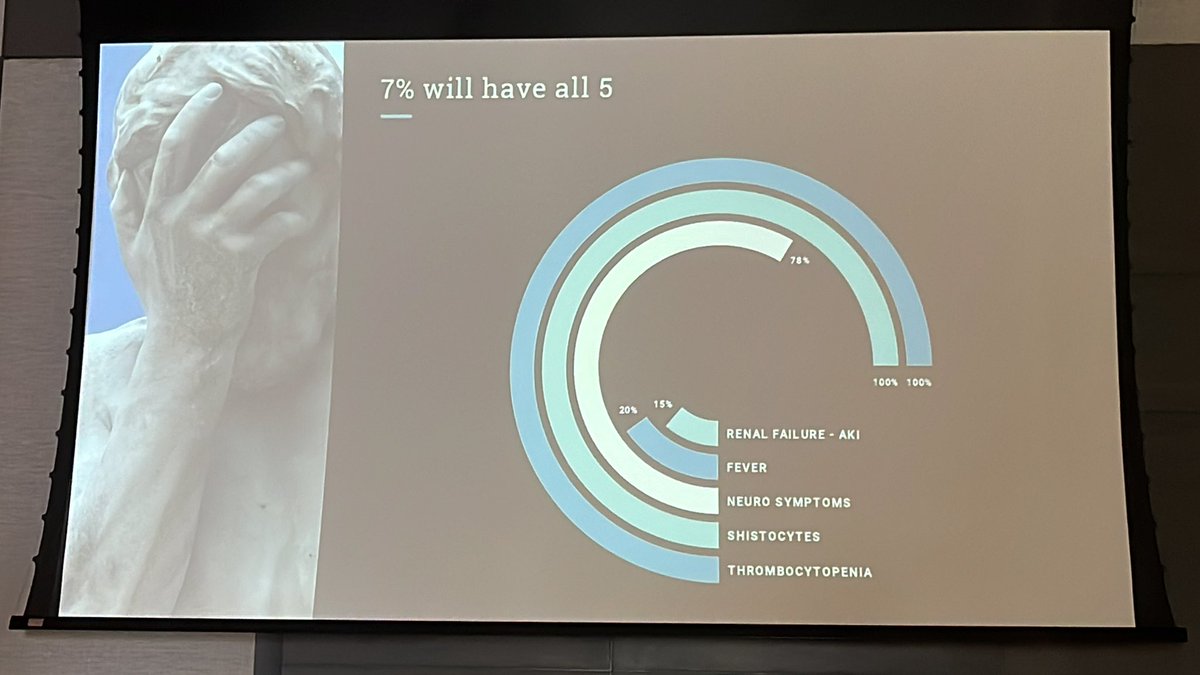
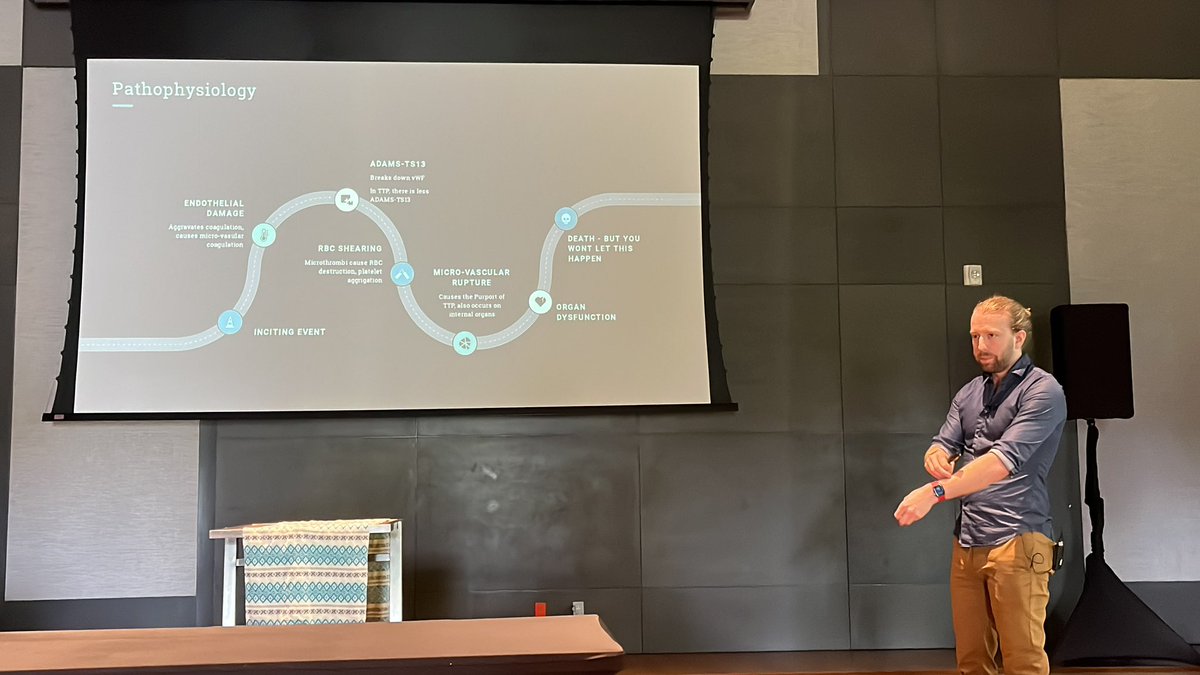
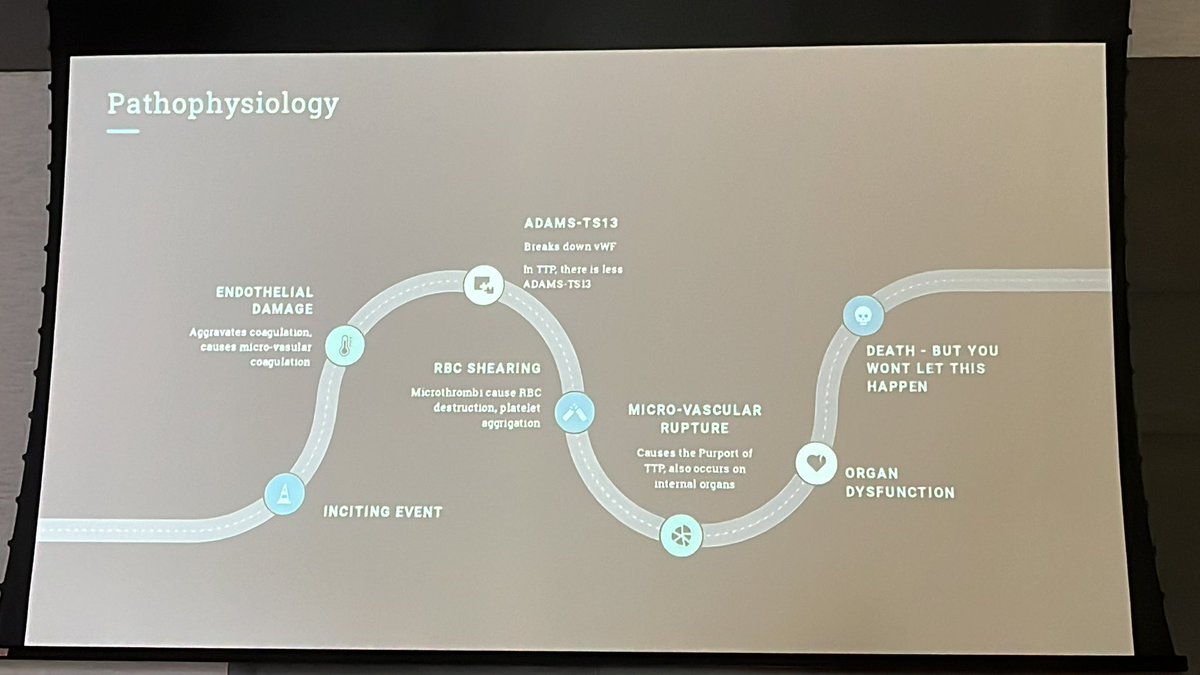
Pathophys of TTP. 90% mortality rate of untreated. Due to endothelial damage breaks down vEF causing RBC shearing leading to microvascular rupture organ dysfunction and ultimately death. While it presents in a pentad usually only 3 will be commonly seen.
@CriticalCareNow takeaways of post ROSC mgt:
Post-ROSC care should be grouped into 3 sequential bundles:
1) 15 minutes post-ROSC,
2) 45 minutes post-ROSC
3) an ICU-level of care in the ED.
#resusfest
Bundle focus:
1:focuses on stabilizing
2:fine-tuning tx
3: ICU-level mgt
In the event PT needs more time in ED after ROSC:
➡️preserve neuro fx; monitor EEG.
➡️ poor data to support empiric ABX, instead start steroids.
➡️Maint. fluids not needed & can cause harm due to excess fluid in the interstitium.@CriticalCareNow
45min post-ROSC:
➡️focus on fine-tuning tx to max survival by fine-tuning airway management, access, and optimizing MAP (goal is 65).
➡️Adjust vent settings to a tidal volume consistent with PT ideal body weight.
➡️Use vasopressors to maintain MAP at goal. @CriticalCareNow
After ROSC has been achieved do a team debrief. It is crucial to take at least 5 mins to discuss with the entire team what went well, what can be done better, and address any lingering thoughts regarding the case. @CriticalCareNow#resusfest
Airway management after ROSC: ⭐️hemodynamics is more important; focus on airway mgt after hemodynamic stability has been achieved.
⭐️consider swapping out SGAs/EGAs to a formal ETT
@CriticalCareNow#resusfest