Enrollment isn't adoption.
A wearable on the wrist ≠ one worn correctly, charged, and synced.
When patients drift, it shows up in your endpoints, not your enrollment numbers.
The tech is the easy part. Keeping patients using it right is the work.
Wearable data in clinical trials:
Everyone's talking about collection.
Nobody's talking about what happens when the signal doesn't translate into usable, study-ready data.
Deployment isn't execution. That gap is where endpoints break down.
Clinical trial patient goes quiet in Week 3.
No diary entries. Wearable unsynced. At risk of dropping out.
Delve Health concierge calls him. On the phone. Right then.
Diary completion: 91%
Retention: 96%
Human support = study integrity.
#ClinicalTrials#DelveHealth
Same patient. Same trial.
One difference:
someone actually helps.
Not reminders.
Not dashboards.
A real person.
That’s when compliance starts to recover.
Episode 2 of 3.
#ClinicalTrials#PatientEngagement#DigitalHealth
Clinical trials don’t fail at visits.
They fail between them.
No support → confusion → missed data → dropout.
Compliance doesn’t crash—
it erodes.
Episode 1 of 3.
#ClinicalTrials#PatientCompliance#DigitalHealth
Clinical trials are not just more digital.
They are more operationally complex.
More endpoints.
More vendors.
More longitudinal data.
Execution continuity — not technology — will define usable evidence.
#ClinicalTrials#PMCF#RWE#MedTech
AI can predict adherence risk.
It cannot sustain execution discipline.
Long-duration trials degrade quietly.
Post-approval evidence quality increasingly depends on continuity ownership, not instrumentation.
#ClinicalTrials#AIinHealthcare#RWE#DigitalHealth
Clinical trials are failing because of poor execution between visits.
As trials grow, retention, adherence, and data continuity become structural risks.
Protocol complexity already impacts outcomes:
https://t.co/1i4erf2AYJ
The next evolution in trials = execution discipline.
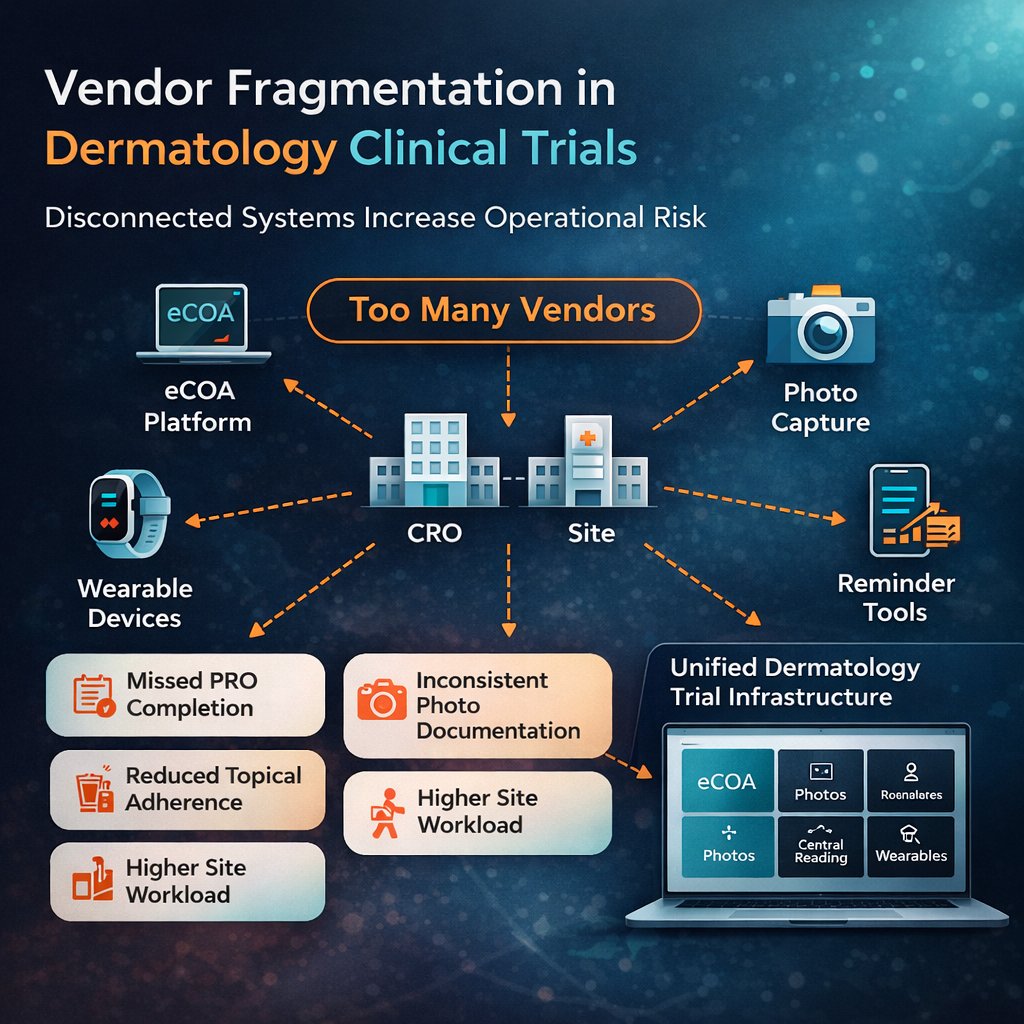
As trials grow more digital, fragmented outcome capture creates real execution risk.
eCOA, engagement, and data oversight must work as one system — not separate vendors.
That’s where study performance is shaped.
https://t.co/KOZk8LZJs2
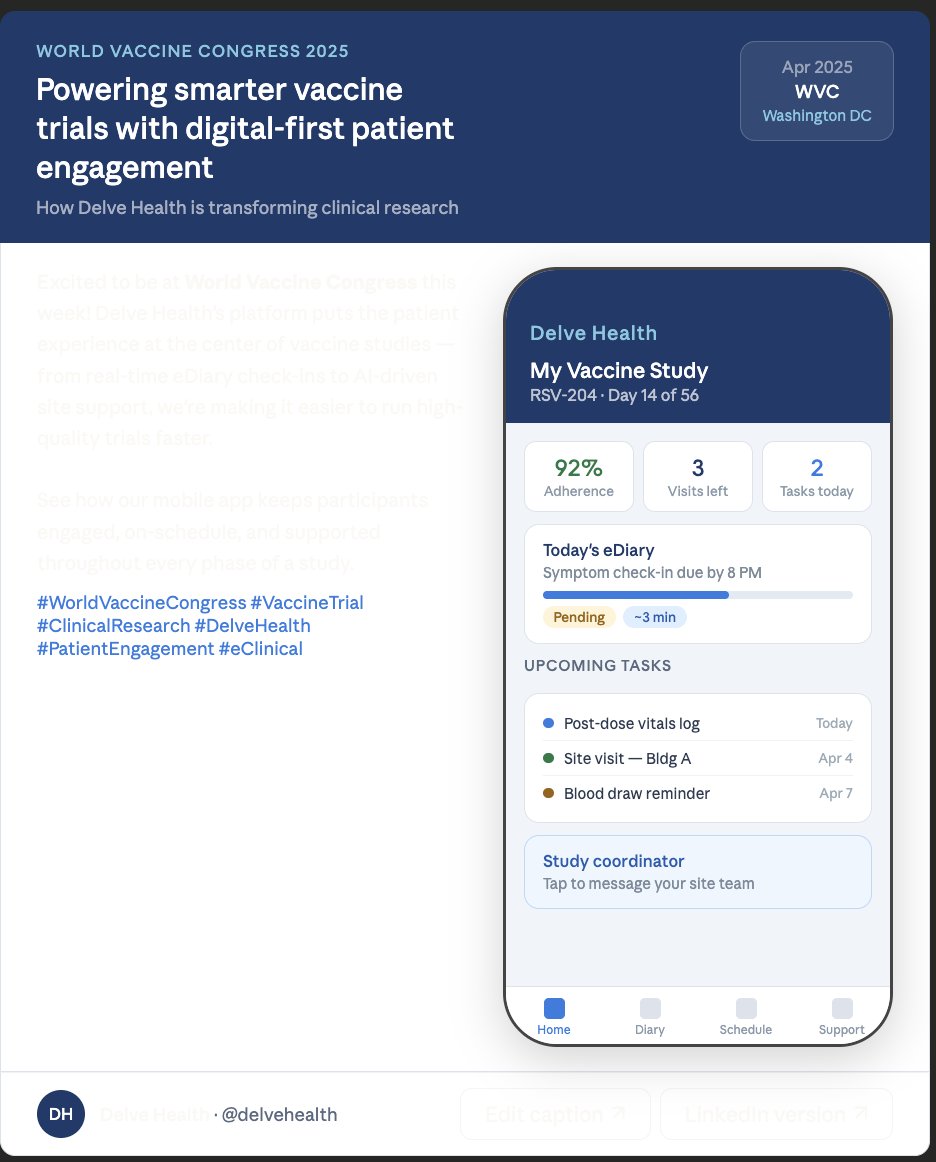
Tired of low eCOA completion? Delve Health delivers 92–98% completion with real-time QC, wearables integration, & human concierge support. Unified eCOA/ePRO for cleaner data & faster readouts.
Check it out: https://t.co/KOZk8LZJs2
#eCOA#ClinicalTrials#DigitalHealth
Alzheimer’s, Parkinson’s, and MS studies depend on data collected between visits.
That’s why modern CNS clinical trials rely on wearables, digital biomarkers, and eCOA to protect the signal.
https://t.co/AF5QPgYXer
#CNSResearch#ClinicalTrials
Rare disease trials have no operational cushion.
When enrollment is 30–60 patients, small gaps become endpoint risks.
Proactive concierge isn’t support.
It’s protection.
#RareDisease#ClinicalTrials
Learn more:
https://t.co/tcemDypPST