@CRUDEOIL231 Thank you for always sharing your insights and trades. Too often X is filled with cherry picked correlations without trades to back up their assertions, nor any admission of trades that don’t work out.
The British establishment have all ready covered this new Banksy up.
Can we get it Retweeted 10,000 times to show that they can never cover up their complicity in war crimes??
Protect the right to protest! RT!
When VL was used as the first-choice device:
⬇️ patients experiencing at least 1 complication (5.5% vs. 9.7%)
⬇️ 3+ intubation attempts (1.2% v 2%)
⬇️ need to change operator (1.8% vs. 4.9%)
⬇️ oesophageal intubation (0.5% vs. 1.4%)
#anaesthesia#MedTwitter
https://t.co/f10XvyQRSi
@Anaes_Journal The dose of the low dose group that demonstrated reduced delirium also worked out to be about 20mg over total procedure. I don’t see anyone using such a small dose and suspect the other confounders you have identified to have perhaps caused a false signal.
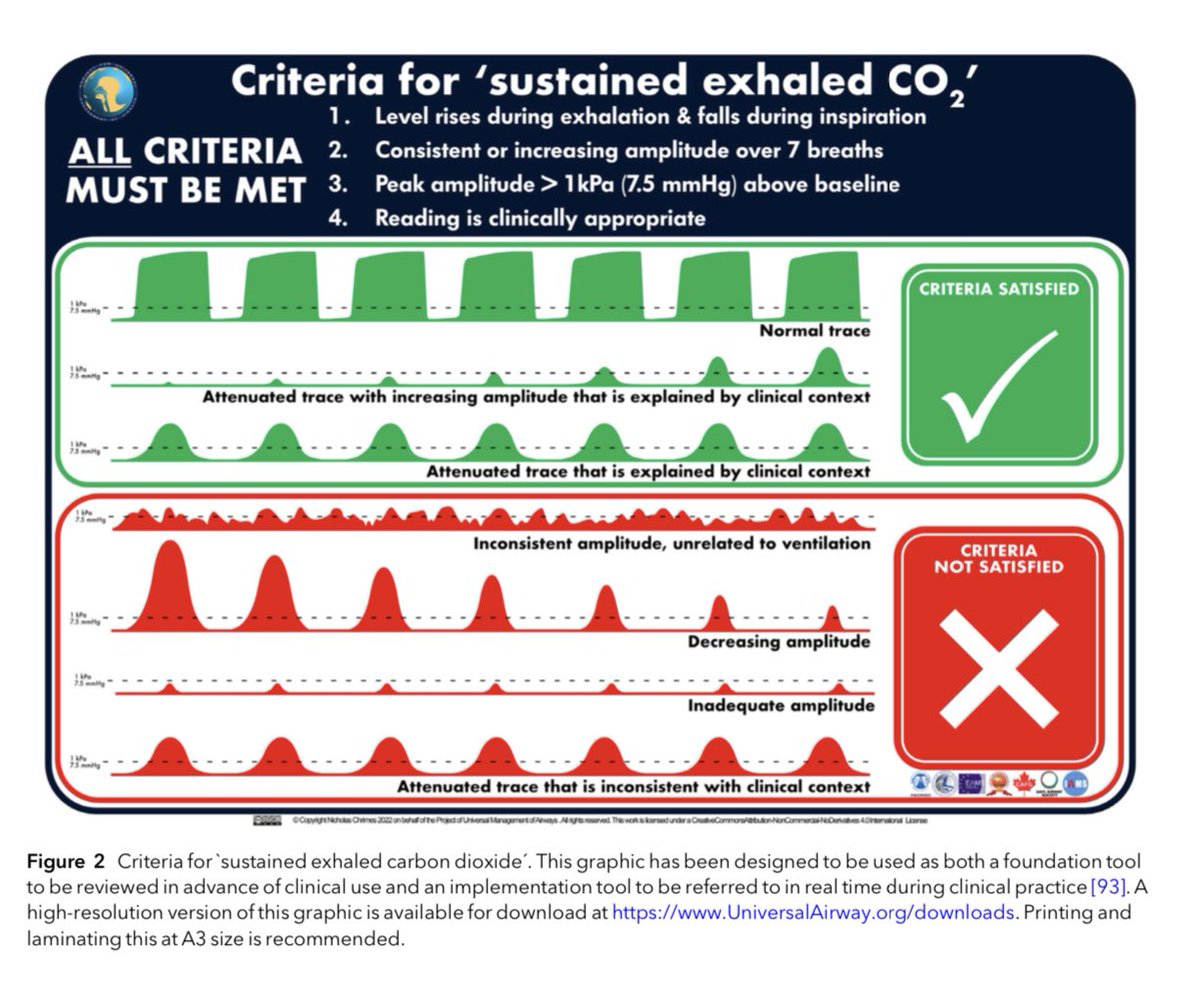
Avoiding unrecognised oesophageal intubation
The @RCoA & @dasairway have agreed to drop ‘no trace wrong place’
The message now is that we need to exclude oesophageal intubation by identifying SUSTAINED EXHALED CO2
This requires 4 elements
-CO2 rises & falls with respiration
-sustained (non-fading, >7 cycles)
-amplitude >1 KPa
-clinically appropriate
It replaces ‘no trace wrong place’ which is insufficient & therefore inadequate
See these two updated webpages
Sustained exhaled CO2
https://t.co/ZAdO23sHil
Prevention of future deaths
https://t.co/goxZZEcCzu
@AAGBI@AndyHiggsGAA@NicholasChrimes
@Anaes_Journal The lower total intraop dose of <0.35mg/kg would for a 70kg of only end up as 24.5mg. It surprises me that anyone would even consider giving such a small amount. Clearly a prospective trial would be warranted to account for the many confounders of this retrospective analysis.
@Anaes_Journal Just use pressure support and PEEP with the mask instead of wasting equipment and time doing HFNO. I easily get ETO2 > 90% in obese pts.
@doctimcook@dasairway@SOBAuk PreO2 using pressure support (I use 4/4cmH2O) means you don’t need to mess about with HFNP. Helps a lot with obese pts to prolong apnoea time prior to desat.