@adfurlan Interesting - data from Wolfe has shown that people who have RA and fulfill the WPI/SSI criteria have significant distress that differentiates them from RA patients who don’t fulfill the FM criteria.
@AsafKlaf 2/2 this means you cannot have pain without nociception, because nociceptive circuits are being stimulated any some@point within the neuraxis
@AsafKlaf Is it not possible that circuits in the brain which orchestrate a stress response interact/overlap with central nociceptive circuits? I think the problem here is that people believe nociception to be purely a peripherally mediated phenomenon. 1/2
Radicular pain and/or radiculopathy. A thread on decision making.
1️⃣ setting the scene
3Ps or serious suspicion aside. What does the evidence tell us
❇️ Wait and see
❇️ Physiotherapy
❇️ Nerve root blocks
❇️ Microdiscectomy
👇👇👇
@CraigLiebenson@sconinxphil @Peter_Stilwell @DrZoffness @JanHartvigsen I believe the best and most empowering narratives is that we teach patients coping strategies to deal with pain as they improve. I find this to be more empowering than a “we fix it” model/narrative
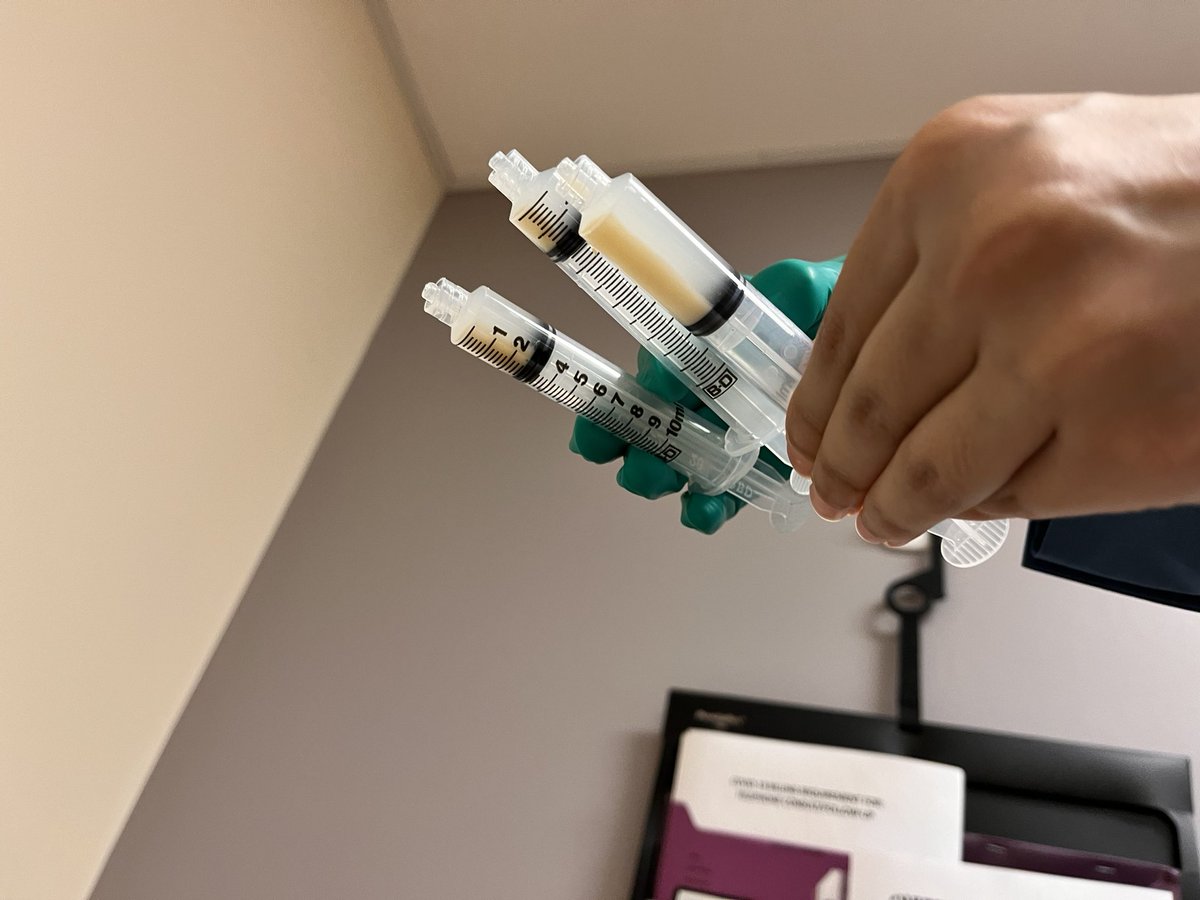
Barbotage of calcific tendinopathy (pics from today) is valuable US guided procedure.
Generally, calcific deposits more than 5mm linear width and posterior acoustic shadow are amenable to barbotage. Come join to learn at USG workshop CAPMR 2023 meeting. https://t.co/1laQMeYs0M