One mindset that separates of surgical trainees:
1) The resident who hopes they'll be told what and where to dissect the whole case
2) The resident who has mentally mapped the dissection from the lastCT scan.
Preparation separates the robots from the surgeons.
There are only two kinds of surgical trainees:
1) The one who treats the ward work as an annoying distraction.
2_ The one who views flawless ward management as the prerequisite to operating.
One stays a spectator. The other becomes a surgeon.
If your had major screw up in the theater (e.g. trigger major hemorrhage), the first move is not to explain.
It’s to verbally admit the entirety of it and then tell you senior what is ONE thing you will drill at home to avoid it.
Extreme ownership means you treat the error as a rescue mission you have to complete, not a chance to create a story about “bad luck.”
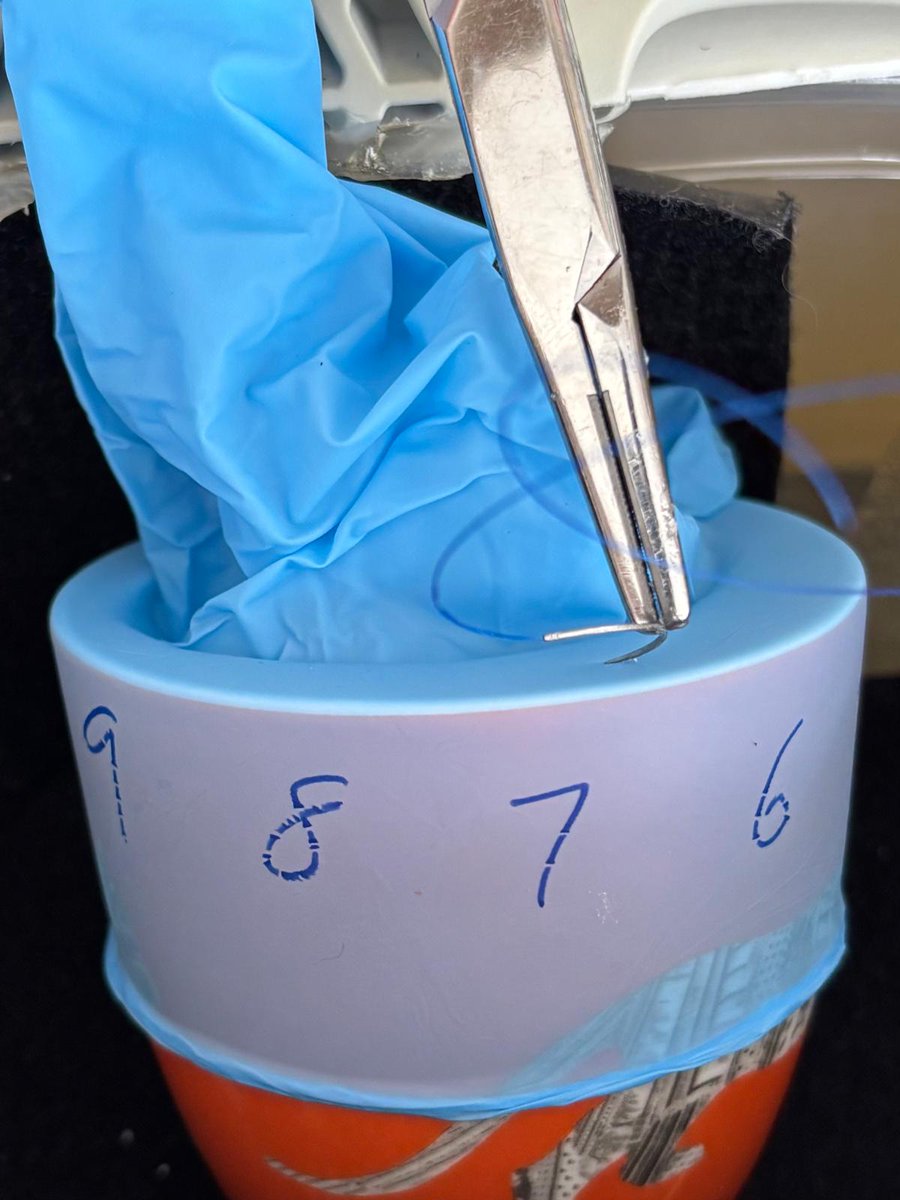
How to master needle driving fast at home:
-Latex glove over a mug
-Place cup inside a shoebox
-Drive bites from 12 o clock to 6 o clock forehand on the glove
-Repeat from 6 o clock to 12 o lock backhand
-Film yourself doing it and pinpoint which areas suck most
PS I bet you its going to be 10 and 5 o clock 😉
Senior don't hand over the cases because you're nice.
They hand it over because you’ve eliminated every reason for them to worry. Early detection of complications. Good communications. Treating everyone as though they're your family admitted to your ward by chance.
Trust is a currency built on the wards and redeemed in the OR.
We just combined a custom AI engine, 3D-printed parts, and perfused pig lungs to train 9 cardiothoracic trainees in Hong Kong. Here’s why.
Traditional training is subjective. We use elite athlete & fighter pilot training principles to create:
• AI-tailored scenarios
• Individually designed perfused pig lungs
• VATS hemorrhage control
• Skill acquisition based assessments
Practice on major bleeds and difficult anatomy before real life. Thanks to all trainees, trainers, Medtronic & Karl Storz for making this happen!
What we built for tomorrow’s lab:
1️⃣ In-house AI individualized VATS scenarios
2️⃣ Personalized assessment reports
3️⃣ Dynamic bleeding ex-vivo lungs
What we couldn't automate: Me, manually dissecting & prepping the specimens tonight. 🔪🩸😂
The OR feels brutal because you only practice in comfort.
Train at awkward angles. Train standing tired. Train with mild distractions.
Make practice harder than reality, and reality stops feeling like an ambush.
How to survive a toxic rotation:
-Assume they're having a bad day (they probably are)
-Track objective data (e.g. types of cases seen)
-Build a home simulation on cases/complications you see
You can't control the senior's mood.
You can control how you maximize your time there.
Every time you finish a case, write down ONE thing you’d do differently.
Not ten. One.
Compound that over a 5-year residency and you'll have 2,000+ incremental improvements.
That is how mastery is built.
Burnout is not personal failure.
Its a mismatch between your expectations and what your program can offer you.
That's why is so important to build self-reliance and drive your own training with sims and feedback loops
The best residents do 3 things differently:
-Ask extremely specific questions
-Logs their complications and reason
-Drill on weak steps on purpose even if its tough
That beats “working hard” almost every time.
Surgery training fails when it gives you:
-Cases without coaching
-Criticism without feedback
-Complications without corrections
That is how you make trainees burnout, not better.
Simulation is not fake surgery.
It is where you should make your worst mistakes safely.
If you only learn on patients, you are paying for your education in blood loss and outcomes.
If you're rehearsing every step, you're not rehearsing any.
Rehearse the part that's the most difficult to you.
One step. One risk. One correction.
That’s how you stay clean, not scattered.
Before you do a procedure for the first time, slow your first 3 breaths before you touch any tissue.
It cuts panic, sharpens hand control, and buys you 10 seconds of clarity that most residents waste on adrenaline
Be cool. Don't rush in trying to "look cool"
98% of trainees feel imposter syndrome.
So it shouldn't mean anything
Do does though is whether you keep showing up, stay coachable, and train yourself when nobody is grading you.
Stop asking your seniors"How did I do?"
It's lazy and gets a lazy answer.
Ask: "What is one specific motion I can fix for the next case?"
Force them to give you actionable data. Then go drill it in the sim lab.
Imposter syndrome isn't a disease you cure. It's a signal you are growing. 98% of residents feel it. The 2% who don't are dangerous. If you aren't terrified of the responsibility, you have no business holding a scalpel.
Confidence is overrated. Evidence is better.
Trainees don’t need to “believe in themselves” more. They need accessible simulations they can do at home can help them chart progress.
That's why we developed so many simulations that you can set up in <5 minutes in your office while waiting for your next case.