❦ Archives, studies & commentary (2020–2026) compiled by Durian LiftOff:
💧 https://t.co/Lh8BpXS3HX
✾ Threads by @DurianLiftOff:
🦋 C-19 in the UK: (25 Aug 2021–'23/'24)
▫️https://t.co/lQ4cVlaLjR
🦋 C-19 ~ On Air: Solutions
▫️https://t.co/nMv5aimw3d
#SARS2#PASC#C19Life
A rash of mask tweets 🧵.
On elastomeric masks, N95s, KN95s, FFP2s, KF94s, care and fit, sourcing, testing, real-world examples & tips, warnings, children's masks, cute alternatives - and why you might want to upgrade now.
#facemask#facemasks#Masks#COVIDisAirborne
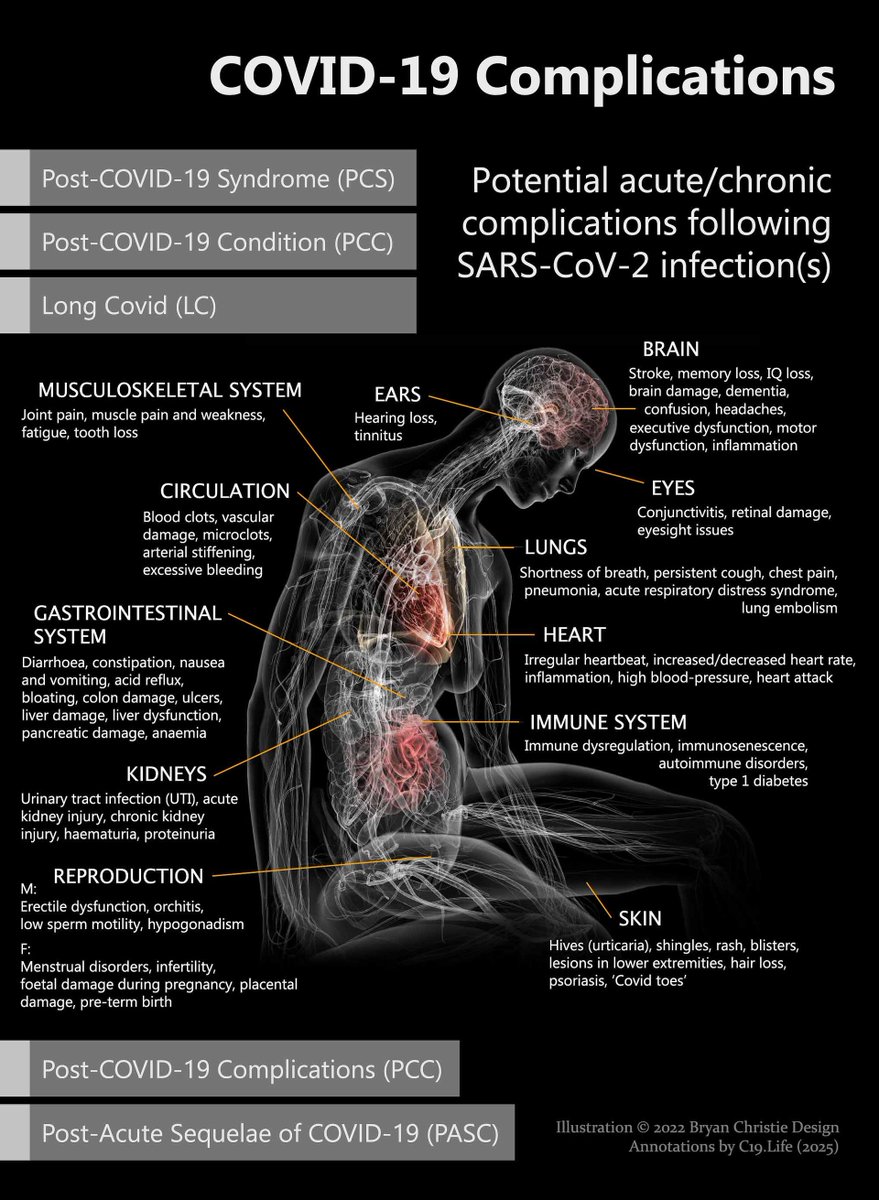
1/2 Long COVID Burden Twice as High as Current Estimates
"Groundbreaking research emerging from Mass General Brigham has unveiled that the true burden of long COVID may be starkly underestimated by current surveillance methods, potentially doubling previously reported figures."
2/2 It is predicted that, without substantial changes in current trends, the long COVID burden will expand exponentially over the coming decade, posing a formidable public health challenge.
https://t.co/43OGmeWQ7m
@DurianLiftOffJr
Tsai, YT., Wang, BY., Ho, SW. et al.
Association of long-COVID with major adverse cardiovascular events and mortality: a real-world data cohort study.
BMC Cardiovasc Disord (25 May 2026).
https://t.co/xvyQqO52xa
#SARS2#CardioPASC
Large study (av age 45) shows people with #LongCovid are 4.48x more likely to have a Major Adverse Cardiovascular Event (stroke, pulmonary embolism, heart failure) & 53% more likely to die.
True regardless of age, BMI, vaccination, variant. Risks last 3+ years from infection. 1/
@DurianLiftOffJr
Tsai, YT., Wang, BY., Ho, SW. et al.
Association of long-COVID with major adverse cardiovascular events and mortality: a real-world data cohort study.
BMC Cardiovasc Disord (25 May 2026).
https://t.co/xvyQqO52xa
#SARS2#CardioPASC
Sex was significant: female sex = 454% more likely to have a MACE (vs 258% for male).
Variant didn't matter - risk of MACEs were 308% for Alpha, 310% for Delta, & 335% for Omicron.
Age didn't matter - risk was 363% for <65 & 283% for 65+.
https://t.co/zf6KtjffOW 2/ #LongCovid
A classic Top Ten++ from Tern on increases in far more than just ten pathogenic infections...
A lot of homework from our favourite online priest: a lot of links, and another page to add to...
❦ Ten people who were wrong.
➲ https://t.co/0yOQHnESwn
#SARS2#PASC#ImmunoPASC
Normally, I like 254nm over 222nm whenever possible because it's so, so much less expensive per watt of output, but bathrooms are harder than expected.
Right before China came out of COVID-Zero I put GUV in my bathrooms in anticipation of infected neighbors and potential transmission through plumbing.
Initially, I found some nice fixtures with built-in PIR sensors. Unfortunately, PIR is nowhere near robust enough for 254nm- if you sit too still on the toilet, it comes blasting on, cooking your eyeballs while you wave your hands frantically to turn it off. I added microwave sensing to that, and it no longer came on when occupied.
The next problem was that the white tile is a pretty decent reflector of UV- so with the door open, all that UV came out into the house. My dogs like to lie in front of the bathroom, and my makeup table was right next to it. It wasn't a super high dose, but it was enough that sustained exposure posed a risk.
I added interlocks to the bathroom doors so the GUV would only turn on if the door was closed and no one was in the bathroom. A lot of wiring and hassle, but it worked.
Even then, it wasn't safe for sequential use. I typically offer the bathroom to women delivery drivers (not that I exclude men who ask, they are very safe and polite, but I am proactive with women because we tend to need it more). That use puts the bathroom out of commission for about 5 minutes while I close the door after they leave, the 254nm lights come on, and any suspended aerosols are inactivated.
254nm also can't be on while I shower- and I have very long hair, so washing it takes a really long time, during which I am entirely unprotected from anything coming out of the drains, which, as we have established, seems to be a primary infection route here in China.
So 254nm can be made to work, but it's complicated, and the protection isn't really optimal. In the end, 222nm really has the edge here, the final cost of a Lantern is almost the same as a 254nm install, and the bathroom is still the place I think most people should install it first if they can afford only one unit.
If you can only budget for 254nm, are handy, and willing to deal with mains voltage, let me know, and I'll put together a parts list for you to DIY.
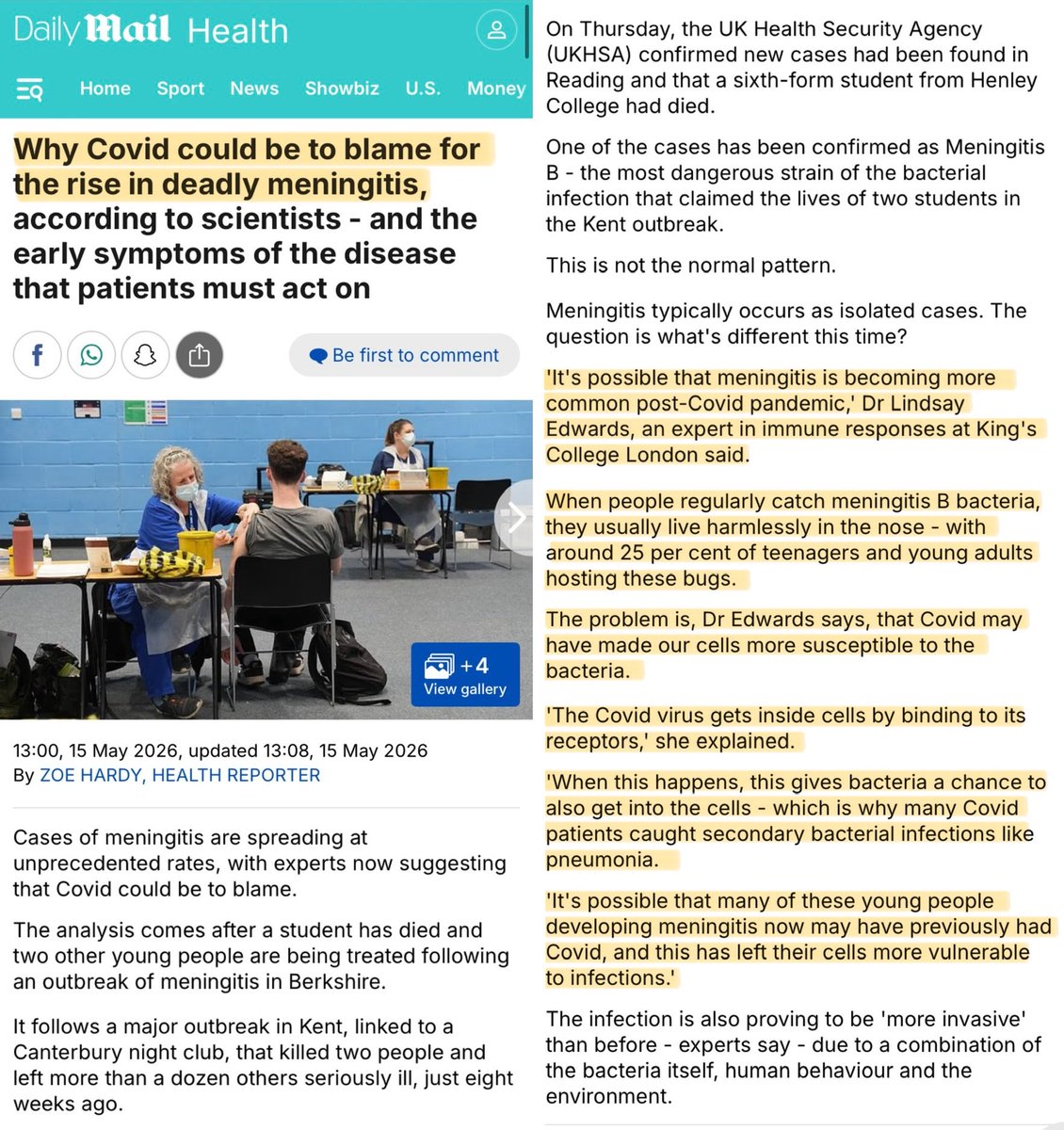
🚨“Why COVID could be to blame for the rise in deadly meningitis”
“When people regularly catch Meningitis B bacteria, they usually live harmlessly in the nose.”
“The problem is that COVID may have made our cells more susceptible to the bacteria.”
https://t.co/APskCrYVni
Unfortunately, "protective bubbles" are almost entirely a marketing myth. Where you place an air purifier in a room in relation to yourself has almost no effect on how much protection it grants you. Air is a fluid, and fluids mix constantly with the slightest movement.
It's like trying to make a "cream only" bubble in your coffee while you're stirring. Only in a room, people are the spoon.
This is easy to verify with even a cheap particle counter. Take a measurement with an air purifier across the room, take a measurement with it next to you- it will be almost identical. The measurement will remain almost identical until you are a few centimeters from the air purifier's output.
People feel a breeze from a purifier blowing on their face, so they think they are protected, but with the exception of some very specialized units like the Air Fanta Wear, there is almost no localized effect- it's all CADR per room, not CADR per cm away from you.
Here's a CFD model with an air purifier in various locations and the relation to particle count in the breathing box (inhalation zone) of a room occupant.
In short, it doesn't matter if you have a lot of CADR close to the performer, just how many CADR in the room. Big air purifiers on stage are mostly for feels and vibes. The data just does not support it. It's too much air, mixing too quickly for a localized effect. A particle counter near the performer and in the audience will show almost the same number.
The bus seat next to me is always the last to be taken on a busy route...
Which I definitely like.
(I also wear @Engineer_Wong's HEPA 'Wear', which fully ensures a wide berth... 😉😁)
#UnintendedBonus
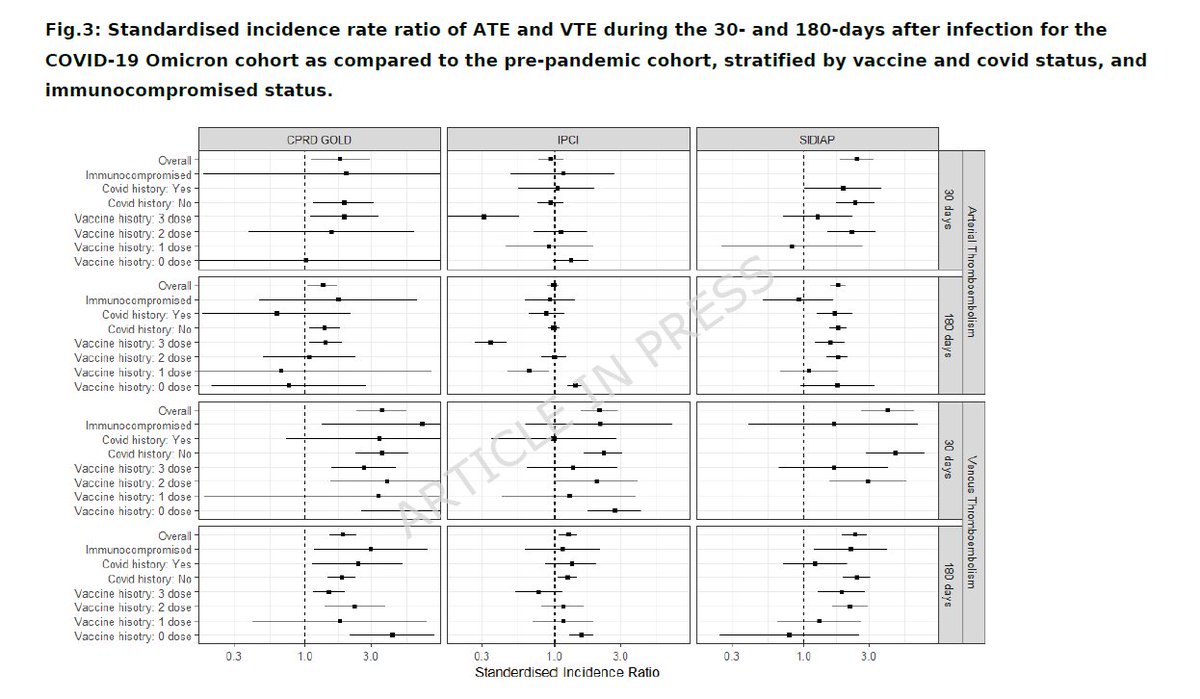
Venous and arterial thromboembolic events after COVID-19 during the Omicron period in three European countries
🚨OOOOh boys and girls, WE WARNED YOU:
With “Mild” Omicron COVID your blood-clot risk is still highly elevated, even if you’re vaccinated. A new 7.6-million-person study just dropped: clots nearly 4× higher in the first month… and still doubled at 6 months!!
• Large-scale European cohort study (UK CPRD GOLD, Dutch IPCI, Spanish SIDIAP, >7.6 million pre-pandemic controls, ~780 000 Omicron-era COVID-19 cases) mapped to OMOP model.
• Compared incidence of VTE, arterial thromboembolism and other CV events at 30/60/90/180 days post-infection vs 2017–2019 background rates.
• Age-sex standardised incidence ratios (SIRs) for VTE: 3.61× (UK) to 4.10× (Spain) in the first 30 days, remaining 1.88–2.37× at 6 months……even in vaccinated populations,
• Risks remained raised up to 6 months for pulmonary embolism (strongest signal), stroke, and heart failure,
• Highest risks in immunocompromised and infection-naïve individuals. Prior infection and higher vaccine doses blunt (but do not eliminate) the increase,
• Vaccination stratified by doses: individuals with exactly one dose showed numerically lower crude VTE/ATE rates (wide CIs, small subgroup),🤔
• Limitations: observational biases (testing, healthcare access, unmeasured confounders), heterogeneous coding across databases, no direct variant sequencing,
‼️Published yesterday, the pre-print “definitive version” of the three-country Omicron preliminary report from 2025, the data are unambiguous: even in the vaccinated, “milder-wave” era, COVID-19 drove a 3.6- to 4.1-fold surge in life-threatening blood clots during the first 30 days and left risk nearly doubled (1.9-2.4×) at six months. Prior infection and higher vaccine doses blunt, but do not eliminate, the hazard. The virus continues to damage the cardiovascular system long after “mild” symptoms fade and by doing so, SarsCov2 remains a potent cardiovascular hazard!
#AvoidSars2 #AvoidReinfections #Mitigate #COVID19 #Thromboembolism
https://t.co/VOcHIRFzk3
A growing number of scientists have been sounding the alarm recently about how repeated Covid infections may be damaging our immune systems…
https://t.co/cKsXSm9Bn2
Tissue-specific autoantibody signatures reveal immune alterations undetected by routine serology in long COVID
🚨83% of long COVID patients have rogue autoantibodies attacking their own heart, lungs & blood vessels, and every standard blood test misses it completely. VERY INTERESTING!
➡️In a UNIQUE Hungarian cohort of 114 long COVID patients versus 36 pre-pandemic controls, tissue-specific Western blotting detected autoantibodies in 83% of cases, with strong cardiovascular dominance,
➡️Vascular autoreactivity was markedly higher in long COVID (34% vs. 8%, p<0.05), cardiac (54%) and pulmonary (34%) signals trended elevated but did not reach significance( cohort size?),
➡️Autoantibodies were predominantly IgM-skewed, polyreactive (up to 8 bands per patient), and persisted longitudinally (mean 141 days), with new isotypes emerging over time,
➡️Standard ANA testing showed no group differences and zero clinical correlations, rendering it useless for detecting these alterations,
➡️Cardiac autoreactivity associated with hypertension and headache, overall autoreactivity correlated with anosmia/ageusia, female sex, CRP, BMI, creatinine, and troponin levels,
➡️The study used human cardiac, pulmonary, and vascular tissue homogenates.
➡️Findings were independent of routine serology and highlight an under-recognized immune component invisible to current diagnostics.
➡️“This persistent, IgM-skewed profile suggests ongoing immune dysregulation and may reflect a previously underrecognized component of the immunological response in long COVID, highlighting the need for targeted immunodiagnostic approaches beyond routine serology.”
‼️Why this is shocking:
It proves that in 83% of long COVID patients, the immune system is actively producing autoantibodies that directly target their own heart, lung, and especially blood-vessel tissues, yet every standard blood test (ANA HEp-2) comes back normal.
These rogue antibodies are polyreactive, IgM-dominant, persist for months, and keep evolving.
They correlate with real symptoms (anosmia, hypertension, headache) and lab markers of damage (troponin, CRP).
‼️In other words:
The majority of long COVID sufferers have smouldering, organ-specific autoimmunity that is completely invisible to routine diagnostics. Doctors are flying blind while patients’ tissues are quietly under autoimmune attack.
🤔As far as I know, this is the first direct evidence of hidden, cardiovascular-dominant tissue autoimmunity driving the chronic L0ngC0vid phase! #BookMark
#AvoidSars2 #AvoidReinfections
https://t.co/3n4gS7gZVI
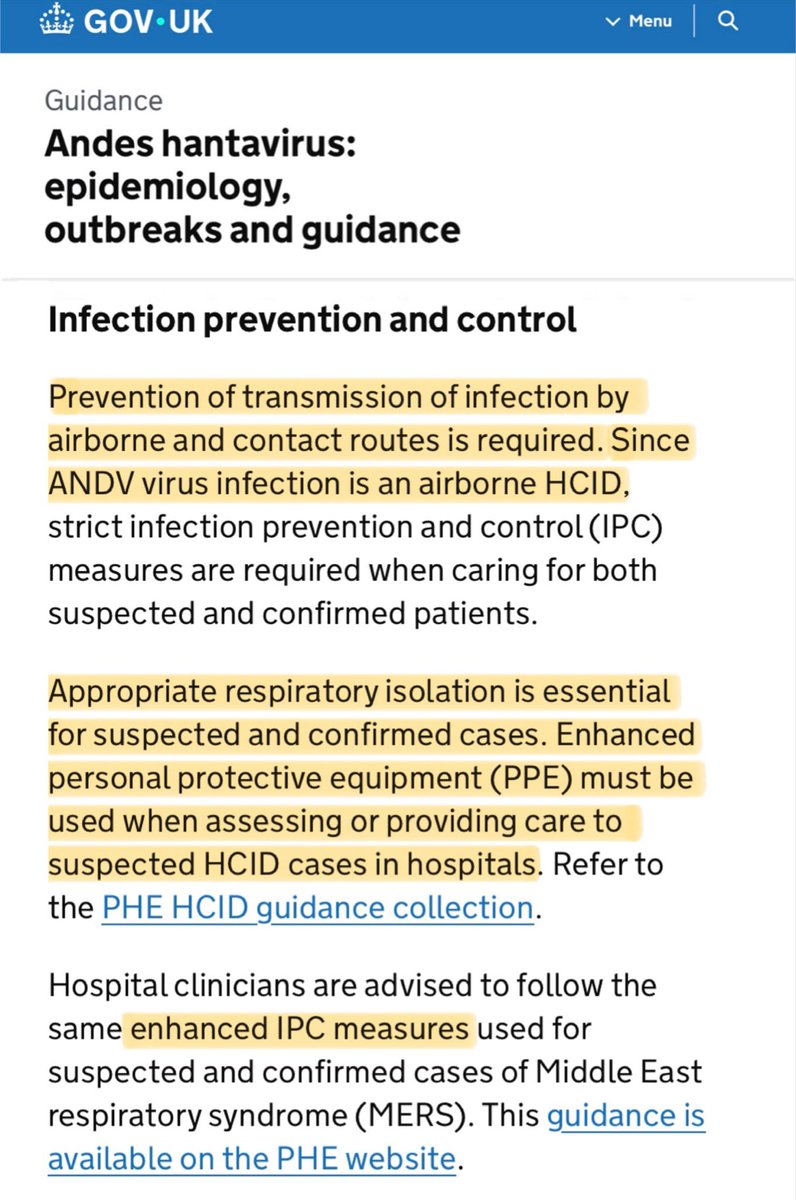
Here in the UK, infection control guidance when caring for patients with suspected or confirmed for Andes Virus requires:
▪️Prevention of transmission by AIRBORNE routes.
▪️Enhanced PPE (ie. FFP3 masks) when assessing or providing care in hospitals.
https://t.co/9vmnxXeqEN