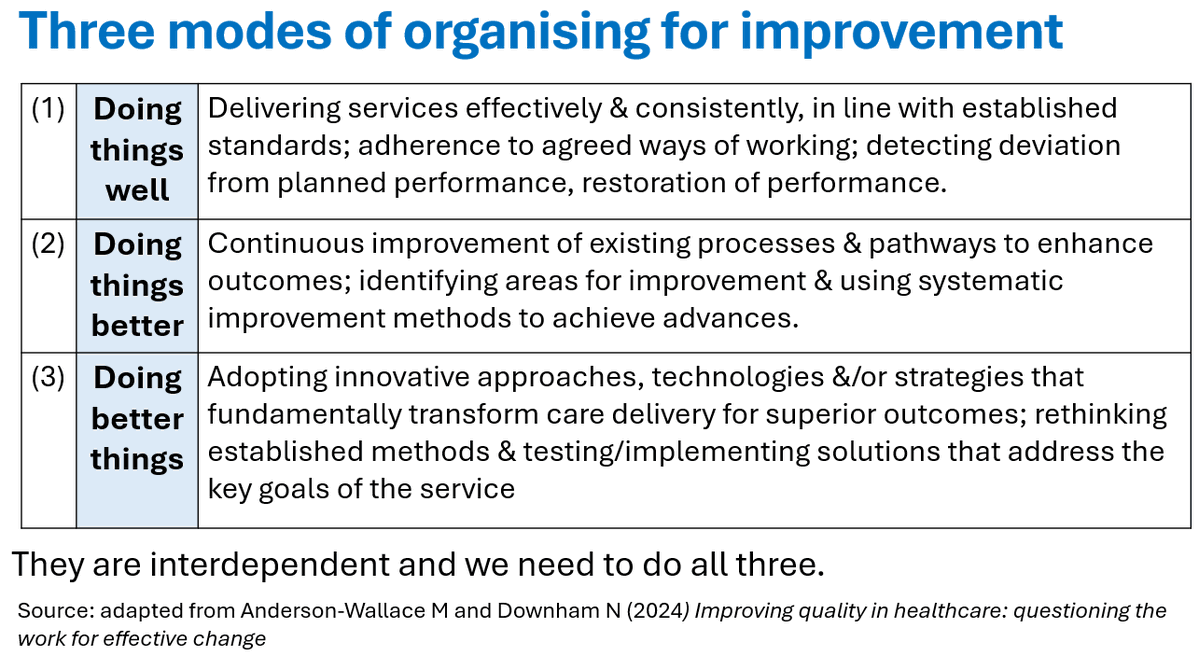
Three modes of organising for improvement:
(1) Doing things well
(2) Doing things better
(3) Doing better things
An organisational improvement strategy should focus on all three. Many organisations currently are overfocussed on (1) & (2) and under focussed on (3). This is risky because we can end up focused on improving the "wrong" or suboptimal things. The environment of change that we find ourselves in means that we have to focus increasingly on (3). It won't happen unless we build in the time & space for connection, collaboration, experimentation & learning into daily work.
I adapted this table from content in "Improving quality in healthcare: questioning the work for effective change" by Murray Anderson-Wallace & Nick Downham. I really like this book, written by highly experienced practitioners: https://t.co/HfBU4n5U85.
It's recruitment time! The VA Quality Scholars Program is recruiting qualified individuals to participate in a two-year advanced fellowship focused on developing leaders & scholars in healthcare improvement. Please see the brochure below for more information & feel free to share!
@austincamp Our institution will be transitioning to EPIC from Cerner in the next 2 years. I appreciate all of these pearls! I’m making a list of these things to look into during the build phase! Keep the pearls coming!
UAB Surgery resident @adamtlucy gave a paper presentation this morning at #AAST2024 - Standardized electronic orders decrease opioid use in emergency general surgery
Great job, Dr. Lucy!
@UABSurgery@traumadoctors
@walidgellad I feel the same way when a single Rx claim for codeine cough syrup 6 months after a surgical procedure qualifies as “persistent opioid use” …
@clhubes My almost 5 year old had a meltdown over this tonight. We usually put both baby and big girl toothpaste together, but ran out of baby toothpaste. Complete meltdown.
Doctors and first responders are sounding the alarm on a critical lifeline that most ambulances don’t have. As @CynthiaMcFadden reports, they say it could save tens of thousands of lives a year.
@DusetzinaS One day everyone will look back in disbelief wondering why the line was never there. Like the “opioid crisis” there will be documentaries about people suffering due to corporate greed & the heroic work of those who FINALLY drew the line. I hope that documentary comes out soon…
I’m not one of those cool pharmacists that just knows the best antibiotic alternative for documented allergies. But… Need someone to comb the EMR to find where the patient got said drug class w/ no reaction? I’m the coolest at that.
@randallwoodfin AL Medicaid has been doing this since 2007!! This is NOT a tax — it’s a fee for INSURANCE COMPANIES (pharmacy benefit managers) to pay!! Instead of paying drug cost x 10% service fee, it’s a flat fee. $800 drug = $80 or $10.64…. Which is “more affordable”?
@chrissyfarr My husband & I are both pharmacists working in very different settings. This article was written 2 years ago, but sadly the reality is that nothing has changed in 10+ years & we will be fighting for another 10+ years.
“Hey this order is going to kill your patient but idk I am just the pharmacist”
*left on read*
“So… are we gonna do anything about this”
*left on read*
Nurse call: “WHY ISNT THIS ORDER VERIFIED???????”