APPROACH TO ANEMIA
Most anemia algorithms start with the MCV.
That’s a mistake.
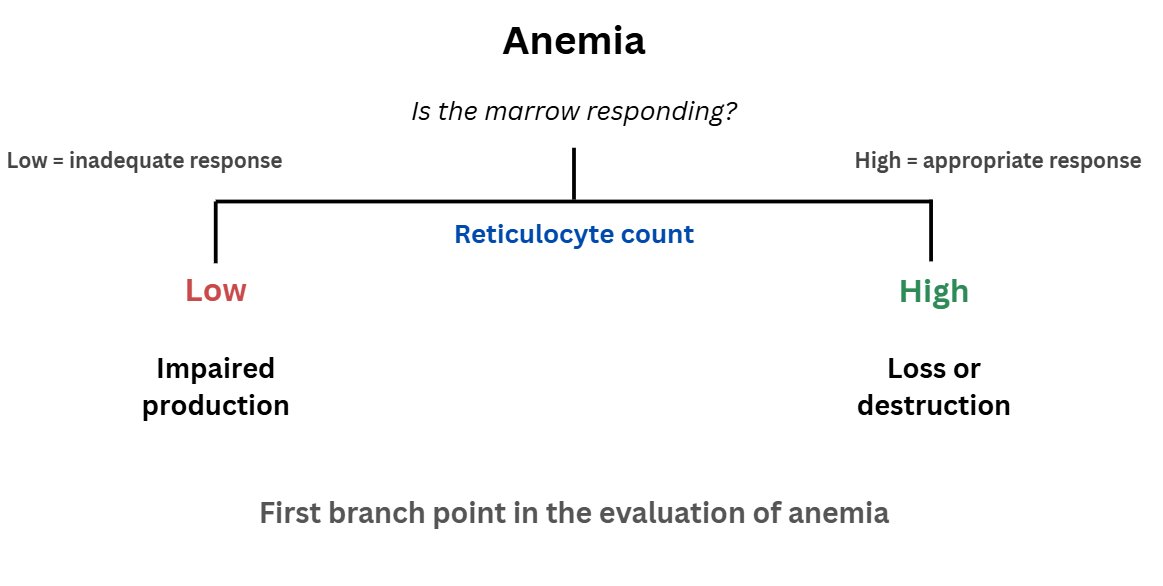
The first branch point is the reticulocyte count.
It asks a physiological question:
Is the marrow responding?
MCV describes appearance.
Reticulocytes reveal function.
Welcome to practicing medicine in Nigeria where becoming a doctor is the easy part.
A medical student once told me he is lacking motivation, I told him he hasn't seen anything yet.
You finish med school, swear the oath, and then begin the real nightmare. The first headache is finding a house job in a country that somehow has a doctor shortage AND no space for doctors at the same time.
If you try to explain this country, you wee just run mad. Then when you finally get one, your salary arrives like a rare celestial event, unpredictable, mysterious, and never on time.
You’re understaffed, overworked, and underpaid, managing 40 patients with God abeg, paracetamol, and faith because the hospital has no monitors, no oxygen, and NEPA is playing hide and seek again.
But don’t worry, if anything goes wrong, it’s your fault because you are the doctor. Nobody cares about the system held together by vibes and prayers.
After housejob, you are promoted to level 2 of shege.
NYSC posts you to a village general hospital or military hospital where the pharmacy is empty, the lab is decorative, and you’re the consultant, registrar, and house officer all in one. Improvisational medicine becomes your new specialty.
You will learn that a nail in the wall serves as perfect drip stand and the examination couch with stoods can actually work as improvised theater table.
Then God help you that you don't Japa and you enter residency. You will expect training but get inducted into a survival game instead. Toxic seniors everywhere who will themselves be complaining of toxic seniors? 36-hour calls will be your daily bread?
You'll wonder whether you're in training or an abuse camp to be stress-tested.
Meanwhile, patients arrive late because healthcare is pay out of pocket. And to be honest can you even afford 300k for emergency ex-lap? Your patients have tried herbs, prayers, and Chatgpt before coming and now they want a miracle. If it works, thank God. If it doesn’t, doctor is wicked.
Equipment? Let's not go there.
ICU beds? 🤣🤣🤣🤣
Security? They still beat your colleague last week and na only God save you.
And when your colleagues start japa-ing. The workload doubles and your HOD doesn't care. If you complain, he'll say he trained in Sokoto where he was the only one attending to 100 patients for 3 months.
The system worsens but no one cares. You consider your life choices at 3am on call while manually ventilating a patient because the machine isn’t working.
And through it all, the system remains underfunded, mismanaged, and somehow your patients keep blaming the doctor.
But yes, please tell us again how doctors are the problem.
A patient present with Hypoglycemia, symptoms relieved by glucose, and low plasma glucose
Diagnosis?
A) Addison’s disease
B) insulinoma
C) MEN syndrome
D) Zollinger–Ellison syndrome