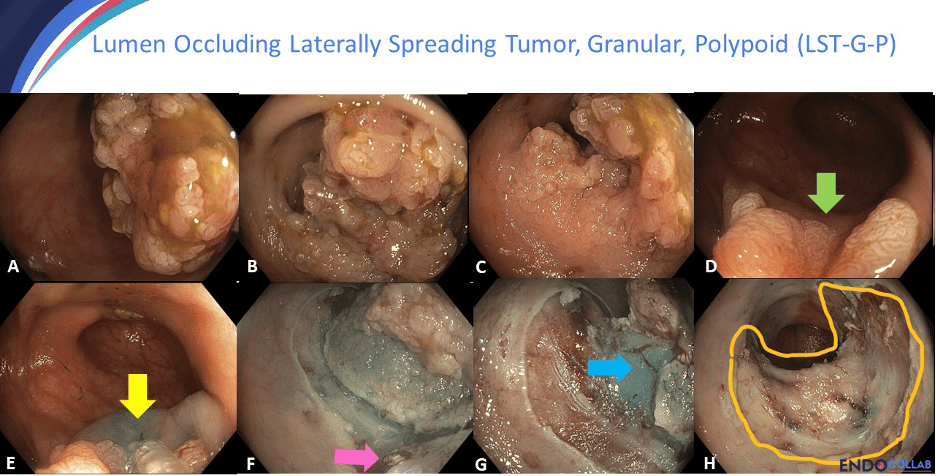
In cap-assisted APC margin ablation after resecting a 7cm LSTG lesion, attach the cap to the endoscope tip. Position the cap openings distally. This allows air, CO2, argon, and fluids to escape during ablation and hemostasis.
A single case report from 42 years ago revolutionized ERCP for bile duct strictures and cholangitis.
This publication fundamentally changed therapeutic endoscopy practices.
Need to review a specific endoscopy technique or classification before your next case?
We compiled our library of short, high-yield lecture clips and procedure segments into one searchable page: https://t.co/UBx5G1aukr
Update: @KMonkemuller account was compromised on May 28.
We are actively working with X Support on recovery (case filed).
Please report any spam/crypto posts or suspicious activity from that account as hacked.
Thank you for your patience—legitimate medical/education content will return soon.
For large balloon sphincteroplasty during ERCP, use a dilating balloon, not an extraction balloon. Obtain biliary cannulation, place a heavy guidewire, perform a small sphincterotomy, and inflate the balloon to create a wide opening for stone extraction.
Six steps for variceal ligation: inspect the varices, check the fundus for gastric extension and document it, target the varix, apply suction, release the band, and insufflate air to detach the banded varix before pulling back.
In mucosal defect closure after gastric ESD, the first clip is not meant to close the opening. Use it to create a small anchor bump on the margin. Place the second clip right next to it, approaching in an inverted T position to initiate effective closure.
Rule 1 for basket extraction: sphincterotomy has to be adequate. Wide exit first. Never size your balloon larger than the distal bile duct diameter. Know your stone, know your duct.
Upper gastrointestinal (GI) endoscopy or esophagogastroduodenoscopy (EGD) continues to be an extremely useful diagnostic tool for perspicuous macroscopic findings.
Read the full case: https://t.co/5eVmHstTvj
A tip every GI trainee should hear early:
When performing submucosal injection, don't just rely on preloaded syringes. Mix your own by adding a few drops of indigo carmine or methylene blue to saline.
Saline mixed with blue dye is a highly effective, low-cost solution.