The INSEMA authors write that omission of SLNB was must be weighed against potential benefit of RNI.
If RNI was a requirement in those with 1-3 nodes, and the trial was properly powered, EBCTCG 2023 suggests the results may have been different.
From one perspective, INSEMA and SOUND are poorly designed and underpowered clinical trials for RNI.
SOUND authors themselves write in the discussion that the trial was not powered to detect differences from adjuvant treatments.
@AppleHelix@JackWestMD Is the pad thai standard of care for treating cancer? Then yes the chef is supposed to change it
Your tweet suggests that those who failed observation should be withheld osi so that the trial is powered
@JackWestMD@AppleHelix I'm rad onc so not totally familiar with the practice patterns at the time, but:
The trial started 10/21/2015
Osi was approved by FDA 4/18/2018
Trial closed to enrollment 1/17/2020
39% in control arm with progression had osi
Seems not too bad given the timeline?
@BijoyTelivala There is no such thing as a “surrogate” endpoint.
Not only that, PFS is a heterogeneous endpoint. “Surrogates” do not take into account toxicity or QOL either
Correlation doesn’t equal causation, as much as pharmaceutical companies trying to save money would like it to.
@gammaemitter @RadoncTables Where is this in the paper? I see that it says TBI was not related, and this post is meant for people to consider ISRT, not TBI
@NRGonc wishlist
1) hyperfx RT with concurrent chemo vs conventional chemoRT for newly dx H&N
2) IMRT vs conventional for breast w or w/out RNI
3) low dose RT for osteoarthritis and other benign things
4) bolus vs no bolus subanalysis on post mastectomy protocols
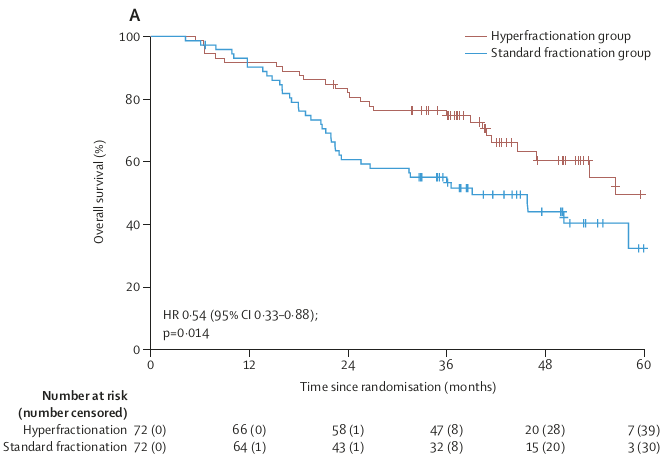
This exciting paper was just published showing proof-of-principle of a core belief in radiobiology we’ve had for a long time: that hyperfractionation can reduce long-term side effects of radiation, in this case translating to OS improvement! #radbio https://t.co/Ixu96EqFoU
@safaviaa@RadoncTables It's difficult to believe that these could be the final DFS outcomes with the length of f/u and that OS hasn't even been reported yet. Data cutoff too early
There are differences between the settings of the trial and SINDAS for sure
@ParikhSimul I like the scope. You can see things that don’t show up on imaging.
If ENT gives you their video that’s fine but photos only are often not adequate
The prostate exam though can go away for rad onc
STRIDE (tremelimumab + durvalumab)
Median OS 16.4 vs. 13.8 mos
3-yr OS 31% vs. 20%
Median PFS not different
Grade 3-4 events similar
Checkmate 459 (nivolumab)
Median OS 16.4 vs. 14.7 mos
2-yr OS 37% vs. 33%
Median PFS 3.7 vs. 3.8 mos
3/3
RTOG 1112
Median OS 15.8 vs. 12.3 mos
Median PFS 9.2 vs. 5.5 mos
TTP also improved
Grade 3+ toxicity not different
KEYNOTE-240 (pembro)
Median OS 13.9 vs. 10.6 mos
Median PFS 3.0 vs. 2.8 mos
Grade 3 events 53% vs. 46%
2/3
@subatomicdoc@bvbal79 @ParikhSimul @Ozradonc@KoneruMd Also there are lots of cancer patients we already see that just happen to also have arthritis pain. Might try this out!