📱Os presento el nuevo vídeo de nuestra App Chronity.
Espero que os resulte útil la aplicación para el seguimiento de vuestros síntomas y la descarga de reportes para llevarlos a vuestras consultas médica.
📲 Descárgala aquí: https://t.co/maGtHnv7VX
Un abrazo!
💙 Nuevo video de Chronity 💙
Vivir con una enfermedad crónica no debería ser sinónimo de soledad.
En nuestro nuevo video te contamos cómo Chronity ayuda a pacientes, profesionales y asociaciones a conectarse, investigar y cuidarse juntos.
📲 https://t.co/q9TbL76QB4
‼️⚠️Please read this until the end.
A widely shared article has presented a deeply misleading view of Long COVID, suggesting once again that cognitive behavioral therapy, exercise, and “mind-body” approaches may be the uncomfortable truth patients refuse to accept.
This needs to be challenged.
Not because the nervous system does not matter.
Not because psychological support cannot help.
But because confusing support with cure, physiology with psychology, and heterogeneity with “it might be in your head” is exactly how medicine has harmed post-infectious patients for decades.
There are articles about Long COVID that look like science journalism, but in reality they repackage, in modern language, a very old idea: if we do not fully understand a disease, maybe the problem is in the patient’s mind.
And that is not science. That is repeating history.
The article begins with a striking sentence:
“There isn’t a single approved pharmaceutical treatment, not even a test to verify the presence of the illness.”
This may sound forceful, but it is a very misleading way of presenting the problem.
The fact that there is still no drug specifically approved for Long COVID, or a single diagnostic test, does not mean that “nothing has been found.” It means that we are dealing with a heterogeneous disease, probably with several biological subgroups, and that medicine has not yet converted those findings into validated clinical tools.
“No single diagnostic biomarker” is not the same as “no biology.”
In just a few years, immunological, vascular, neurological, endocrine, and metabolic abnormalities have been described in subgroups of Long COVID patients: autonomic dysfunction, herpesvirus reactivations such as EBV/HHV-6, alterations in the cortisol axis, autoantibodies against GPCR receptors — including adrenergic and muscarinic receptors — persistent viral antigens, endothelial damage, muscle abnormalities after exertion, mitochondrial dysfunction, persistent inflammation, and differential immune changes.
Is everything settled? No.
Does that mean it is psychological? Also no.
Science does not work like that. Multiple sclerosis did not stop existing before we had MRI. Many autoimmune diseases do not show up in routine blood tests. If a complete blood count, a basic biochemistry panel, or an X-ray comes back “normal, normal, normal,” that does not prove the absence of disease. It only proves that you are looking with inadequate tools.
One of the article’s most serious mistakes is this: it confuses the absence of a simple clinical test with the absence of organic disease.
And that mistake has caused harm for decades.
The article also says:
“Almost $2 billion and half a decade of international effort have yielded little more than hypotheses about micro blood clots and spike proteins and mitochondrial dysfunction.”
No. That is not correct.
A hypothesis is a provisional explanation. But when you compare patients and controls and find significant differences in muscle tissue, metabolism, response to exertion, immune biomarkers, viral antigens, autoantibodies, or vascular dysfunction, you are no longer talking about “little more than hypotheses.” You are talking about lines of biomedical evidence that still need to be organized, replicated, stratified, and translated into treatments.
That is not scientific failure. That is research into a complex and new disease.
🔵Continued in the next post.👇🏻
(1/6)
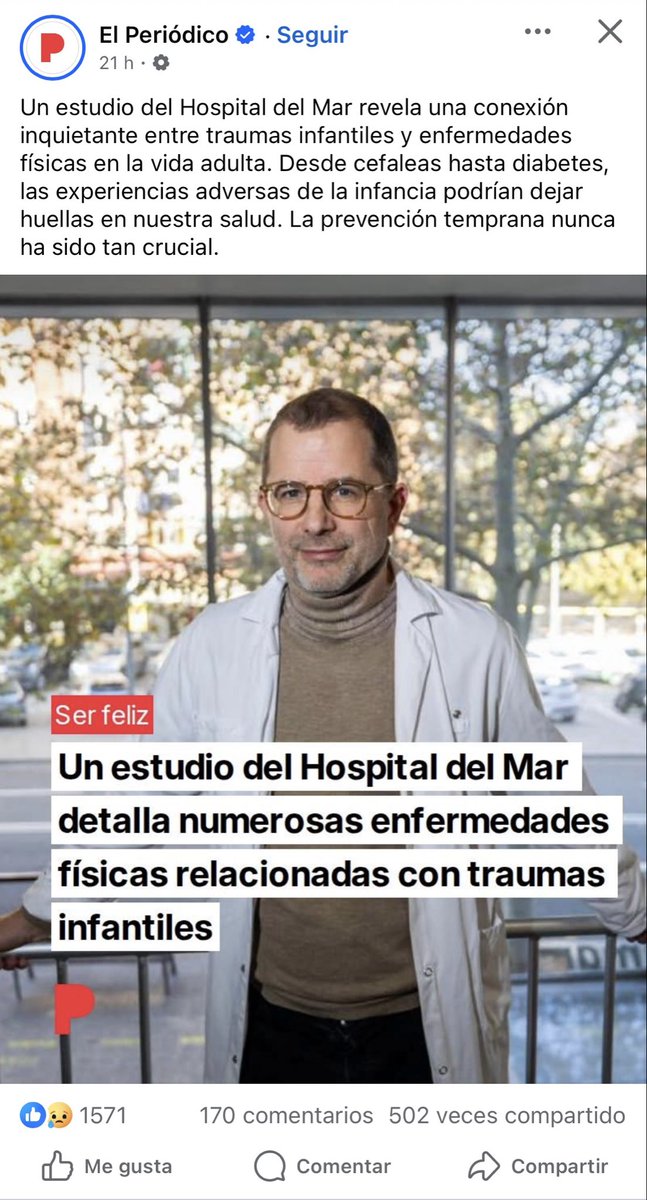
⚠️‼️ I came across this news in Spain, and this discourse keeps doing enormous harm.
The post literally says:
“A study from Hospital del Mar reveals a worrying connection between childhood trauma and physical diseases in adult life. From headaches to diabetes, adverse childhood experiences could leave marks on our health. Early prevention has never been so crucial.”
“A study from Hospital del Mar details numerous physical diseases linked to childhood trauma.”
Not because they literally said that most organic diseases are caused by childhood trauma, but because in practice, many of the diseases they attribute to or reduce to trauma end up being organic diseases whose biomarkers have not yet been discovered, or whose proper medical workup was never even done.
And that is the real problem.
For years, many patients are first filtered through the lens of trauma, psychosomatic illness, or somatization, when in reality what they have is an organic disease that has simply not yet been diagnosed. I would even go further and say that this also happens with diseases we now understand well: before reaching the right specialist and before the appropriate tests are performed, many patients are treated as if the origin of their symptoms were psychological or trauma-related, simply because nobody has investigated their case properly.
That is not precision medicine.
That is a way of covering diagnostic ignorance with a psychological narrative.
The history of medicine shows this again and again: many diseases that in their early stages were treated as “nervous,” “hysterical,” or “psychosomatic” later turned out to be well-defined organic diseases. This happened with multiple autoimmune, neurological, and inflammatory diseases. And it is still happening today.
That is why this discourse is so dangerous. Because it not only delays the real diagnosis, but also blames the patient, isolates them, sends them into the wrong clinical pathways, and steals years of serious medical investigation from them.
Most of these patients do not need their illness to be explained through trauma.
They need the right tests, the right specialist, and serious investigation of their real biology instead of convenient theories being projected onto them.
Enough of turning the absence of known biomarkers into a psychological explanation.
What some people today call trauma or somatization too often ends up tomorrow having a name, a mechanism, and a biological marker.
Llega un buen momento… y en lugar de disfrutarlo del todo, te preguntas cuánto durará 💭
Cuéntanos 💬 ¿te pasa eso de medir el tiempo incluso cuando estás bien?
Ese “no te obsesiones” cuando lo único que has hecho es intentar que alguien te escuche de verdad 💭😔
Cuéntanos 💬 ¿cuántas veces has sentido que no te toman en serio?
‼️📢Ya está abierto el periodo de votaciones de los proyectos participantes en la 5ª edición de “La voz del paciente”, la iniciativa solidaria de @CinfaSalud con la que Cinfa quiere apoyar y reconocer la labor de entidades como la nuestra que ayudan a pacientes, personas con discapacidad y a los familiares que les cuidan.
📆Desde hoy, 16 de abril, y hasta las 12 del mediodía del 6 de mayo, se pueden conocer los 436 proyectos que se han presentado a esta edición y votar por ellos.
Para poder votar es necesario disponer de un teléfono móvil.
El proceso es muy sencillo: tras indicar el número de teléfono, se recibe un código de verificación que es necesario introducir para que el voto quede registrado correctamente.
Por defecto, este código de verificación se enviará a través de WhatsApp.
En caso de no disponer de este servicio o no recibirlo, se puede escoger su envío por SMS.
Al finalizar el periodo de votaciones, las 100 entidades que más apoyo hayan obtenido 📈 recibirán las aportaciones de Cinfa.
Este es el enlace directo a nuestro proyecto:
https://t.co/eTQM3q2TJW
‼️VÓTANOS Y AYUDARÁS A NUESTROS SOCIOS/AS CON ENCEFALOMIELITIS MIÁLGICA Y A SUS FAMILIARES, ya que nuestro proyecto tiene como objetivo mejorar la calidad de vida de las personas socias de la Asociación de Personas con Encefalomielitis Miálgica (PEM) y de sus cuidadores (socios), mediante la concesión de ayudas económicas directas destinadas a cubrir gastos derivados de su atención sanitaria y terapéutica.
Las ayudas económicas directas se concederán a personas socias de la asociación para contribuir a sufragar gastos como:
- Consultas médicas privadas.
- Tratamientos de fisioterapia.
- Atención psicológica o psiquiátrica.
- Medicación prescrita y suplementos utilizados como parte de su tratamiento.
#VozPacienteCinfa #EncefalomielitisMiálgica #pwME #MyalgicEncephalomyelitis
‼️Ayúdanos y difunde este mensaje para que consigamos ser una de las asociaciones de pacientes que recibe la ayuda. Podéis usar las imágenes que adjuntamos para vuestras publicaciones de redes sociales y para vuestras stories.
Por fuera todo parece normal… pero por dentro es otra historia completamente distinta 💭
Cuéntanos 💬 ¿cuántas veces te han confundido “verte bien” con “estar bien”?
Repitiendo lo mismo una y otra vez… como si tuvieras línea directa de atención al cliente 24/7 📞😅
Cuéntanos 💬 ¿cuántas veces has tenido que explicarlo desde cero?
Mirando el reloj… no para ver la hora, sino para calcular cuánto más puedes aguantar ⏰💭
Cuéntanos 💬 ¿cuántas veces has estado así, contando energía en lugar de tiempo?
Como si la paciencia viniera en pastillas… y no fuera lo que más cuesta cada día 💊😅
Cuéntanos 💬 ¿cuántas veces te han pedido paciencia como si fuera tan fácil?