🤕🤦♂️Headache Thread🤦♀️🤕
I will try to cover common DDx in 1ry & 2ry Headache, Red Flag/screening Qs, resources/links etc
I may add to it over time so consider bookmarking / sharing if useful.
Aimed towards MSK clinicians, FCP/ACPs, Primary Care non-medics for now
Long-term risk of knee replacement after ACL reconstruction using the contralateral knee as an internal control: a National Hospital Episode Statistics database study of 135 881 patients
👇👇👇
https://t.co/av0xUm0P3d
Neurogenic Claudication Territories in Lumbar Spinal Stenosis.
📚 Young JJ et al. Digital pain diagrams to identify common lumbar spinal stenosis pain distribution patterns: a cross-sectional latent class analysis. European Spine Journal. 2025.
https://t.co/8YI0D1E2ch
Preliminary investigation. More atypical & heterogeneous than you might think
Authors used digital pain diagrams in 2,379 patients with LSS. 6 clinically recognisable pain distribution classes rather than one classic “textbook” presentation.
📊 Pain distribution classes:
⭕️ Class 1 (11.4%) → Bilateral posterior leg pain
⭕️ Class 2 (8.7%) → Bilateral posterior + anterior leg pain
⭕️ Class 3 (26.1%) → Unilateral posterior leg pain
⭕️ Class 4 (21.0%) → Unilateral posterior leg pain + low back pain
⭕️ Class 5 (22.9%) → Unilateral anterior + posterior leg pain
⭕️ Class 6 (9.9%) → Multisite pain
Clinical take aways👇
⚠️ The “classic” bilateral posterior leg pattern was less common.
⚠️ Unilateral presentations were more common than bilateral ones.
⚠️ Anterior thigh/leg symptoms were common, challenging the idea that LSS is predominantly a posterior calf/buttock condition.
⚠️ Low back pain severity was relatively similar across groups, questioning how diagnostically useful back pain itself may be.
⚠️ Multisite pain presentations existed
So not so neat, entirely fits my biases and observations.
⚠️ Drawbacks: cross-sectional study only, preliminary data, secondary care sample, based on clinical coding rather than imaging-confirmed standards, no symptom-quality mapping or imaging correlation, several common co-morbidities/masqueraders excluded.
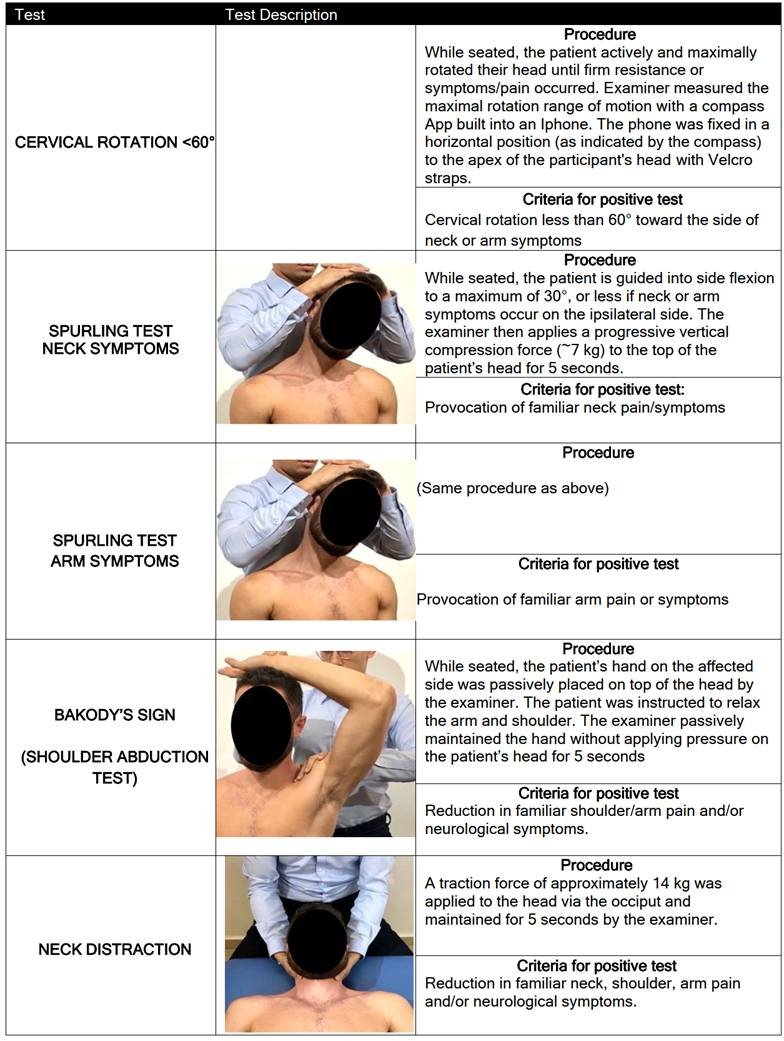
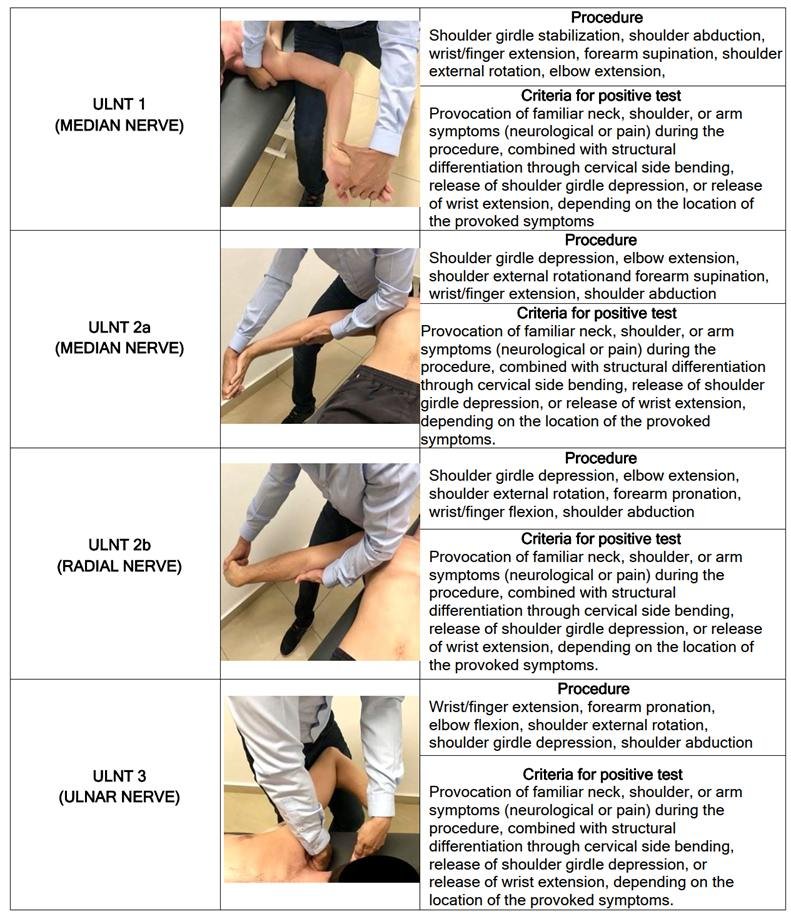
An independent validation of a clinical prediction rule for the diagnosis of painful cervical radiculopathy. 2026.
Highlights:
New 3-test cluster showed stronger diagnostic utility than original clinical prediction rule.
New cluster includes Spurling, Shoulder Abduction test, ≥2 positive ULNTs.
Positive cluster (3/3) rules in CR with 100 % post-test probability.
Negative (0/3) cluster rules out painful cervical radiculopathy diagnosis.
Modified Shoulder Abduction test showed higher post-test probability.
https://t.co/6M5gkzs7BU
.@Retlouping's recent posts on Centralisation and Peripherilsation in Radiculopathy reminded me of my recent use of the Puddle metaphor in Radicular Pain - which has been received well by Sciatica patients.
Sometimes with progress I don't see a pattern of centralisation or peripheralisation... just a "drying up" of radicular pain.
I present to you: Puddlisation.
Comes with the added metaphorical benefits of using "rainy days" to explain an exacerbation, and the use of seasons "summer is around the corner" for drying up (majority of Australians get it).
19/Now move beyond mneumonics!
Remember, brachial plexus splits & recombines like jumping jacks w/a very palindromic 5-3-6-3-5 pattern
The names tell you if they are splitting or combining (Trunk=Together, Division=Divide, Cord=Combine, Branch=break)
Dear followers and colleagues of exercise works,
this verified professional account has been compromised and the rightful owner is locked out.
We’re asking for your help- please retweet this post so @Support can see the request to restore the account.
Your support is appreciated
PSA "Exercise works" - a verified, well respected account created by Ann Gates X/twitter account has been hacked and unfortunately we can not gain access, they have renamed the account "bluntnchill". Please be advised this is not associated with us.
@Safety@Support
PSA "Exercise works" - a verified, well respected account created by Ann Gates X/twitter account has been hacked and unfortunately we can not gain access, they have renamed the account "bluntnchill". Please be advised this is not associated with us.
@Safety@Support
@Support@Safety
Verified account @exerciseworks has been hijacked. The owner’s original case is stuck in your queue with no human follow-up. The account contains her verified professional work and intellectual property. Please escalate for manual verification and restoration.
ACL ruptures in under 18s - how do you manage them?
🧑⚕️👩⚕️ Calling UK surgeons, sports med docs, physios & sports therapists.
We’re exploring equipoise in the treatment of children & adolescents with a primary ACL rupture.
📢 Have your say by completing our short survey
👇👇
🛑 Physiotherapists are breaking down.
Workload pressures, lack of autonomy, and emotional strain are fueling a burnout crisis in UK physiotherapy.
If we don’t prioritise support structures, we risk losing valuable professionals.
What can we do to change this?
Could anyone help please, with
Predictors of injury in terms of assessment
Predictability of work placed Msk issues
Any data on the above or papers?
From my limited knowledge in this field I feel there is nothing concrete?
Is it time to "redefine" obesity? Is BMI no longer sufficient to diagnose excess adiposity?
The Lancet seems to think so, and they just proposed a new diagnostic framework to reflect this new thinking.
Limitations of BMI:
- BMI is useful for identifying individuals at increased risk of health consequences but is not a direct measure of body fat.
- BMI cannot determine the distribution of body fat or establish whether excess body fat is a health problem.
For example...
Overweight (BMI: 25–29.9) may include individuals with excess body fat or those who are metabolically healthy, while obesity (BMI: 30+) can include individuals with high body fat who may or may not exhibit signs or symptoms of illness.
This may have several unintended consequences:
1. Individuals with high muscle mass (e.g., athletes) may have high BMIs despite low body fat, leading to inappropriate diagnoses of obesity.
2. People with excess body fat but a BMI under 30 may go undiagnosed, even though they have health risks.
3. Some individuals with high BMI may maintain good health and normal organ function, challenging the current definition of obesity.
Basically, BMI alone is insufficient for diagnosing obesity, more comprehensive assessments are needed to determine the full extent of weight-related health consequences, and health context matters more than BMI as a number.
Thoughts?
Your regular reminder, @NHSEngland & @wesstreeting, that when trusts treat their resident doctors this callously, their willingness to go the extra mile dries up.
Productivity starts with staff feeling valued - not trampled on.
Someone should study whether trainee portfolios actually achieve anything. I’m seriously unconvinced they make better doctors.
All I see are trainees drained of the joy of medicine and patients.
There has to be a better way than this tick-box rubbish.