Heidi Klessig MD is a retired anesthesiologist who writes/speaks on the ethics of organ donation and transplant. Her new book is "The Brain Death Fallacy."
Since some new followers have joined us recently, I thought I’d share my personal experience with organ procurement.
Back in the late 1980s, during residency training, I came in for night call and was told to go up to ICU and prepare a young man for organ harvesting. I believed my authorities when they told me that the brain dead young man I was to anesthetize for organ procurement was dead. Even though he had a normal blood pressure, heart rate, great oxygen saturation, was warm and with good color, and was making urine. In fact, he was more stable than most other ICU patients I had anesthetized. I was so brainwashed that I wasn’t even going to give him actual anesthesia, just a paralyzing drug and meds to keep his blood pressure and heart rate controlled so as not to damage the organs. But when I presented my anesthetic plan of care to my supervisor, he said I should give a consciousness blocking drug “just in case.” I did as I was told, and the young man responded to surgery just like anyone else, requiring the same types and amounts of anesthesia. When I told this story to a pathologist friend, she said that when she removes organs during an autopsy, she doesn’t need to give any of these drugs.
This bothered me enough that eventually I did my own research. I discovered that there have never been any facts, studies, or evidence that these people are dead. Doctors, lawyers, philosophers, and scholars have been debating the veracity of brain death for nearly sixty years in the medical literature, but the public is never told that there is any controversy. I wrote a book, “The Brain Death Fallacy,” and maintain a website Respect for Human Life, to provide fully informed consent for the general public on these issues.
The new American Academy of Neurology brain death guideline now explicitly states that brain death can be declared in the presence of ongoing brain function. It has long been known that 20% of people declared BD still have electrical activity on EEG, and over 50% have ongoing function of a part of the brain called the hypothalamus. BUT the Uniform Determination of Death Act stipulates that there be an irreversible cessation of ALL functions of the entire brain for a legal diagnosis of brain death.
It is troubling that not only is the brain death concept unproven, but also the way doctors are diagnosing it does not comply with the law. That’s why I do what I can to give the public a place at the table in this debate.
Germany is again considering making every citizen a compulsory organ donor unless they opt out.
But consent cannot be presumed when no one is being informed of the facts surrounding “brain dead“ organ donation.
Brain death is not true death, but a severe form of neurological injury.
The idea of brain death being death has been falsified: people have recovered brain function and continued to live after a brain death diagnosis made according to brain death protocols.
Implied consent, especially in absence of the facts, is NO consent and a violation of human rights.
@InitiativeKAO
BIG Thanks to Maatkamp Publishing in the Netherlands for providing their book chapter on treating severe brain injury to the family of Annelise Camp and her caregivers!
I had the privilege of assisting in the English translation of this book by Ruud van der Ven last year.
Chapter 15 reviews multiple treatments for brain injury, beginning with hypothermia, and including a critique of the Eurotherm trial. The chapter includes this quote:
“Joseph Varon, chief of critical care at United Memorial Medical Center in Houston, used hypothermia to protect his patients from neurological damage after various types of trauma, including cardiac arrest, stroke and hepatic failure. He routinely had his patients cooled to 32°C (89.6°F) (that temperature was maintained for 11 days). In 2014, he saved his own life when he suffered a stroke. The first thing that came to his mind was: cool me! (Jaekl, 2017)”
The chapter also discusses treatment of the damaged hormonal system with T3/T4, hydrocortisone, and ADH, as well as the treatment of global ischemic penumbra.
Also included is an excellent review of use of antioxidants in brain injury, such as B vitamins, glutathione, choline, glutamine, vitamin D, omega 3 fatty acids, and DMSO.
Unfortunately, research into the best treatment practices for people with severe brain injury is still in its infancy because most of these sufferers very quickly either have their support withdrawn or become organ donors.
Giving these desperately ill people and their families the right to try new and innovative treatments will only end up helping us all.
@TXRightToLife@SteveTothTX@joevaron@MidwesternDoc
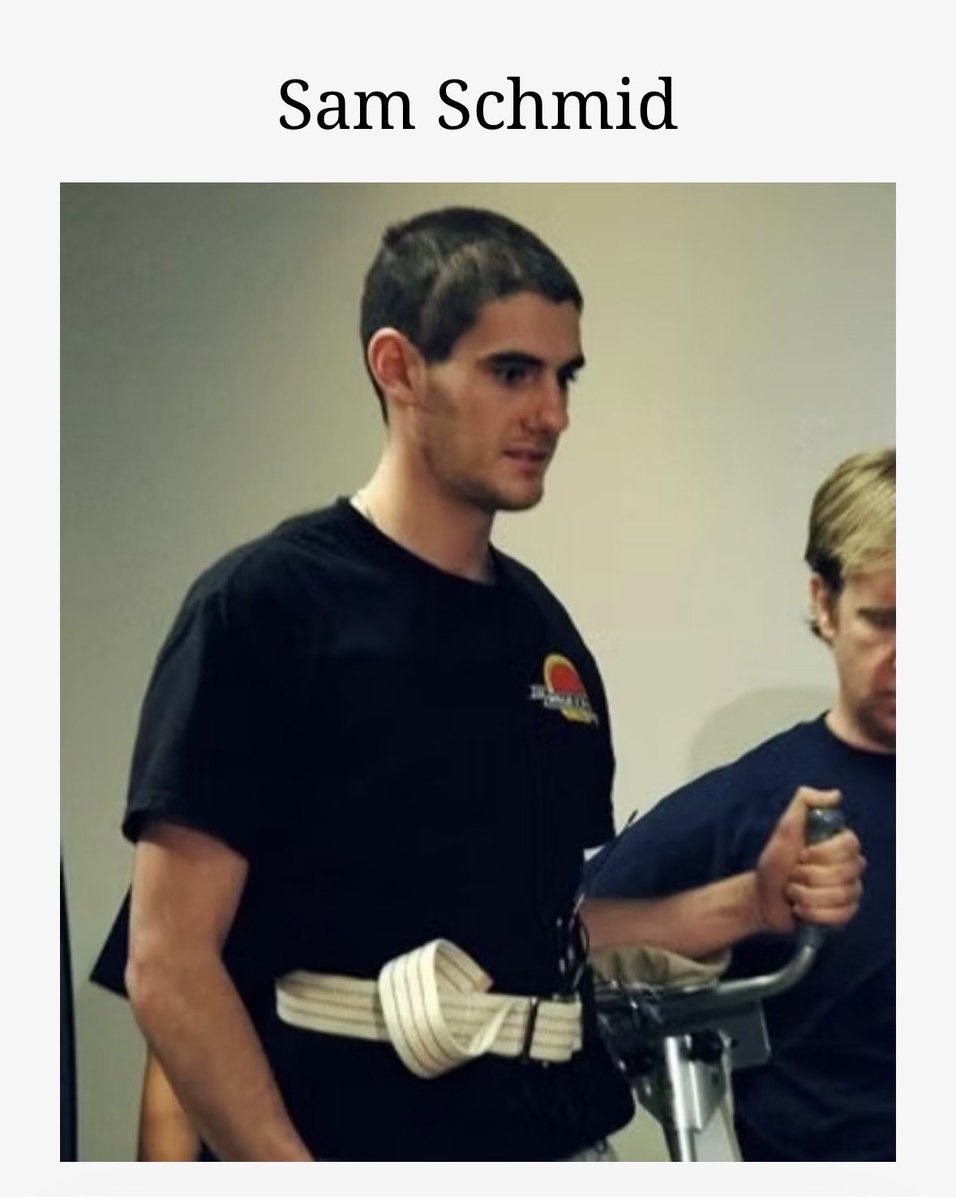
Sam Schmid sustained massive brain injuries after a car crash in 2011.
Doctors were discussing organ donation and his parents were ready to take him off life support when he surprised everyone by raising his fingers.
With surgery and extensive physical therapy, he was able to recover and play basketball again.
“Schmid's doctor, renowned neurosurgeon Dr. Robert Spetzler, agreed that his recovery was miraculous. ‘I am dumbfounded with his incredible recovery in such a short time,’ said Spetzler. ‘His recovery was really remarkable considering the extent of his lethal injuries.’ … But he (Spetzler) said it was ‘reasonable’ for others to consider withdrawing the patient from life support. ‘It looked like all the odds were stacked against him,’ said Spetzler.”
It’s perfectly reasonable to consider withdrawing extraordinary medical support in order to allow a beloved family member to enter eternity.
It’s completely unreasonable to send a vulnerable person with a poor prognosis to a cold operating room to be dissected for their viable organs.
But this is what is happening in hospitals every day under the DCD organ procurement protocol. This could have happened to Sam Schmid if he hadn’t managed to move his fingers.
Thankfully, Sam Schmid was given a chance, and he recovered.
There is a grave lack of disclosure given to people who are registering in good faith to become organ donors.
Important information that any reasonable person would want to know before making end-of-life decisions should be made available to the public.
Here are the facts about brain death determination, donation after circulatory death organ procurement, and normothermic regional perfusion organ retrieval:
1. Whereas the Uniform Determination of Death Act (UDDA) requires that there be an irreversible cessation of all functions of the entire brain, including the brain stem for a diagnosis of brain death, the American Academy of Neurology brain death diagnosis guideline for physicians explicitly allows brain death to be declared in the presence of ongoing brain function.
👉Americans should be made aware that the way doctors diagnose brain death does not comply with the law under the UDDA.
2. Donation after Circulatory Death (DCD) organ procurement begins after just 2-5 minutes of pulselessness. But everybody knows that people are routinely resuscitated within this timeframe. Dr. Ari Joffe published a list of patients who auto-resuscitated up to 10 minutes after cardiac arrest, with some making a full recovery.
A case report from Illinois of a young DCD donor whose heart began beating again and who began gasping for breath during the removal of her kidneys also shows that people cannot be known to be dead within this short timeframe. (The county coroner determined her death to be a homicide.)
👉DCD donors are not known to be dead at the time that their organs are removed, and the public deserves to be informed of this.
3. Normothermic Regional Perfusion (NRP) organ retrieval begins by declaring death according to the UDDA’s circulatory-respiratory standard: the irreversible cessation of circulatory and respiratory functions. But then surgery begins with clamping off the circulation to the brain, following which a full resuscitation of the remaining organs takes place, such that the heart starts beating again in the patient’s own chest.
Of course, this shows that the UDDA’s legal definition of death under the circulatory-respiratory standard was never met because the patient’s circulatory-respiratory function had obviously not irreversibly ceased. But, because doctors are planning to restart the patient’s heart, they take steps to make the patient brain dead on purpose so that now the patient’s death becomes defined by the UDDA’s brain death clause.
This technique plays fast and loose with the legal definitions of death under the UDDA as well as with the dead donor rule. The American College of Physicians (ACP) called for a pause in the practice of NRP in 2021, as "the burden of proof regarding the ethical and legal propriety of this practice has not been met," but this concern has been ignored.
👉People should be informed about the particulars of the NRP donation process, and that the largest medical specialty organization in the world (ACP) has called for a pause in this practice because of concerns regarding its ethical and legal propriety.
In Summary
Each of these points listed above is of sufficient magnitude to deserve immediate remedial action, and in aggregate constitute a severe breach of public trust by the current organ procurement and transplantation system.
The determination of death affects us all, and reflects deeply held philosophical, cultural, and religious value systems. The public has a right to know in what ways their deaths are being determined prior to registering as an organ donor.
NRP organ harvesting: first they stop your heart, then they clamp off the blood flow to your brain (to make you brain dead on purpose), then they restart your heart in your own chest to be sure it’s in good shape to put into somebody else.
In the never-ending quest for viable organs, doctors have found a macabre new way to skirt both the brain death and circulatory death criteria. Transplant centers around the country are removing people who have signed a DNR order from life support, waiting for their hearts to stop, and then immediately clamping off the blood flow to their brains to make them brain dead on purpose. Then their organs are resuscitated, but the person doesn’t wake up because the circulation to their brain has been clamped off. The protocol for this procedure, called normothermic regional perfusion (NRP) from the University of Nebraska notes: “The initial step for ligation of the blood vessels to the head is necessary to ensure that blood flow to the brain does not occur. Once blood flow to the heart is established, the heart will start beating.” How dead are you if doctors can re-start your heart in your own chest?
Lauris Kaldjian, MD, PhD, director of the program in bioethics and humanities at the University of Iowa Carver College of Medicine writes, “NRP represents a technologically elaborate attempt to refashion definitions of death to maximize the number and quality of transplanted organs. It both depends on and violates the circulatory definition of death and arguably employs iatrogenic [doctor-induced] brain death.”
The American College of Physicians recommended in 2021 that the practice of NRP be paused, as "the burden of proof regarding the ethical and legal propriety of this practice has not been met." Other nations, such as Australia, have banned NRP altogether. But despite ongoing ethical concerns, this type of organ harvesting is continuing and expanding in the United States, with half of the country’s organ procurement organizations already participating.
How many families would give their loved ones over to transplant teams if they knew the grisly reality taking place behind operating room doors? While professionals debate the ethics of NRP, people continue to sign their donor cards in ignorance of these facts. Refuse to be a registered organ donor.
“In fact, it has now become clear that no reasonable person accepts the Harvard committee position that ‘brain death’ is a plausible definition of death.”
Robert M. Veatch was a graduate student in 1968 when the Harvard ad hoc Committee published their landmark article proposing the idea of brain death. Fifty years later, in 2018, he wrote:
“Little did we realize that not only would the work to defend this position have yet to be done but that, once started, it would run into snags, leaving us fifty years later with the definition of death still unresolved.”
“Presently at least six significant disputes rage about brain-based death pronouncement: whether patients and families should have the right to refuse testing such as apnea testing, which criteria set should be used in measuring brain function loss, whether clinician error in applying tests is too great, whether the criteria measure loss that is really irreversible, whether loss of all functions of the entire brain can be measured with existing criteria sets, and, most critically, whether current whole-brain concepts of death should be favored over some version of a circulatory or higher-brain concept.”
“Given that we now recognize three major alternative groups of definitions and countless variations within these groups, clearly no one view of what it means to be dead commands anything like majority support, and a literal whole-brain view is totally implausible.”
People with unresponsive wakefulness syndrome (vegetative state) are also being neglected and written off as “unsalvageable.” Neurological injury has a range of severity: from the football player who gets a concussion, to a stroke victim, to people like Terri Schiavo who had unresponsive wakefulness/vegetative state but could still breathe independently, to people whose coma is accompanied by an inability to breathe on their own — these last are the ones being falsely labeled as “dead.”
Many people believe that once a person has permanently lost the capacity for consciousness, their life is no longer worth living.
Some philosophers have taken this idea to the next step and proposed that once patients have a permanent loss of consciousness, they should be considered dead for all ethical and legal purposes: the “higher mind” definition of death.
This view suffers from a couple of very significant problems.
First, thousands of people in a persistent vegetative state (thought to be permanently unconscious) are living in nursing homes throughout the world, breathing on their own and receiving tube feeding. Under the "higher mind death standard," all of these people would be legally dead, and we would be logically committed to treating them in the ways that we treat dead people, including burial and cremation. Yet very few would be willing to bury or cremate a person who is still breathing.
Second, the old idea that a persistent vegetative state eventually became permanent has turned out to be false.
This old dogma was based on a 1994 NEJM task force report saying that a persistent vegetative state became permanent if it lasted three months after an anoxic brain injury and 12 months after a traumatic brain injury. But we now know that even adults diagnosed as being persistently vegetative can improve.
Terry Wallis was thought to be in a permanent vegetative state following a car accident in 1984. But in June of 2003 he began to speak, asking for his mom and a Pepsi. He lived for 19 more years, interacting with his family.
An even more recent (2024) NEJM article reports that 25% of people who doctors believed to be unconscious showed covert consciousness when given advanced diagnostic testing.
Our biases about brain injuries have led us to write these people off as being “as good as dead.” Our biases have also led to premature discussions about terminating care instead of pursuing innovative strategies for healing. We need to do better.
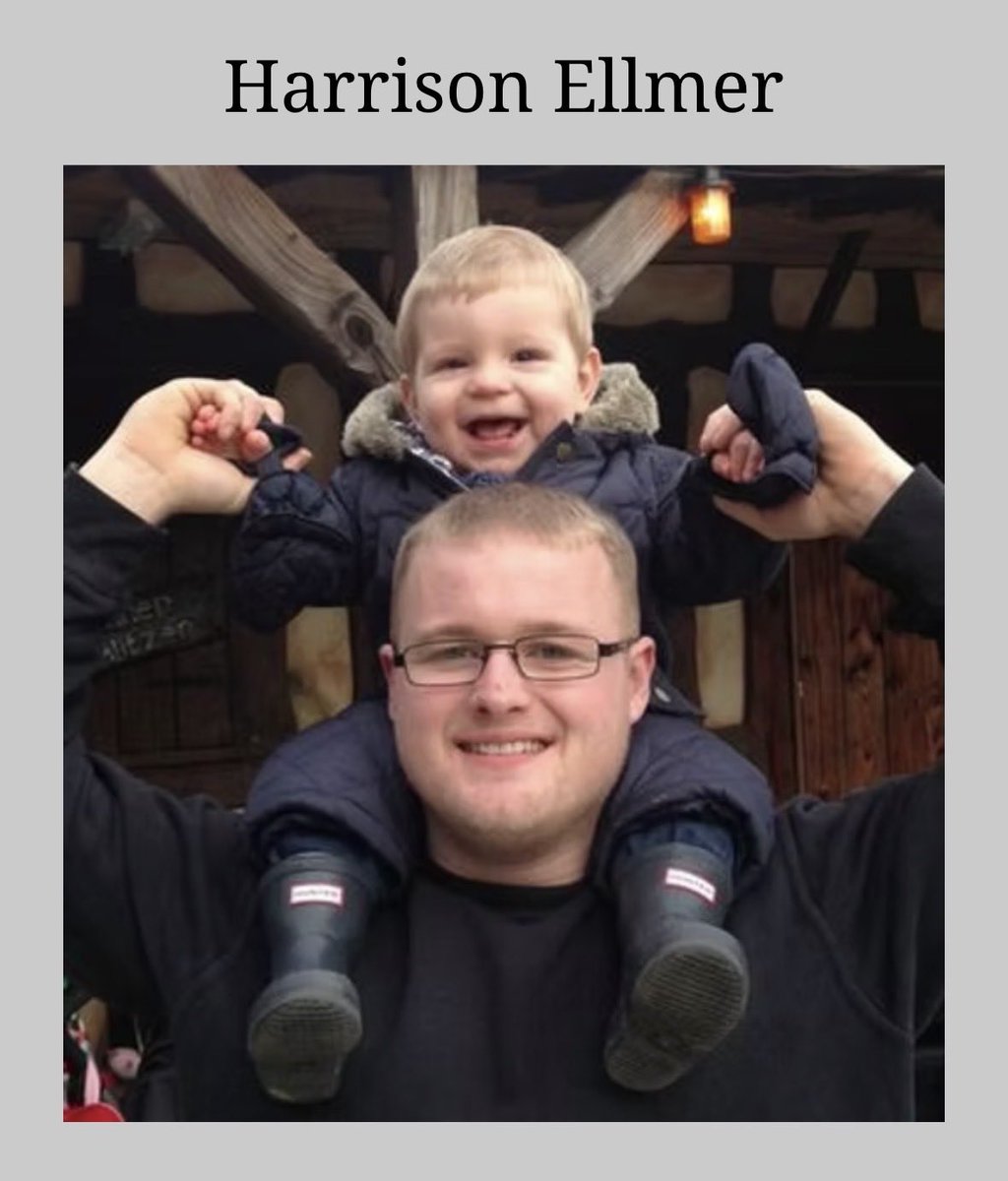
Harrison Ellmer contracted meningitis in 2013 when he was just three weeks old. Doctors said he was brain dead and that there was no hope.
His heartbroken parents decided put him on hospice and withdraw his support.
But when the ventilator was disconnected, Harrison surprised everyone by breathing on his own. His mother describes their experience:
"We were terrified but so thankful he had survived that we just took each day as it came. Harrison's brain scan results showed that he was completely brain dead but we always hoped he'd defy the odds. We still can't believe it ourselves when we see him walking and talking. Harrison wasn't expected to survive but now he's hitting all his milestones just like other children his age."
Harrison had almost completely recovered as he reached his 3rd birthday and plans were being made for him to attend preschool.
NRP organ harvesting: first they stop your heart, then they clamp off the blood flow to your brain (to make you brain dead on purpose), then they restart your heart in your own chest to be sure it’s in good shape to put into somebody else.
In the never-ending quest for viable organs, doctors have found a macabre new way to skirt both the brain death and circulatory death criteria. Transplant centers around the country are removing people who have signed a DNR order from life support, waiting for their hearts to stop, and then immediately clamping off the blood flow to their brains to make them brain dead on purpose. Then their organs are resuscitated, but the person doesn’t wake up because the circulation to their brain has been clamped off. The protocol for this procedure, called normothermic regional perfusion (NRP) from the University of Nebraska notes: “The initial step for ligation of the blood vessels to the head is necessary to ensure that blood flow to the brain does not occur. Once blood flow to the heart is established, the heart will start beating.” How dead are you if doctors can re-start your heart in your own chest?
Lauris Kaldjian, MD, PhD, director of the program in bioethics and humanities at the University of Iowa Carver College of Medicine writes, “NRP represents a technologically elaborate attempt to refashion definitions of death to maximize the number and quality of transplanted organs. It both depends on and violates the circulatory definition of death and arguably employs iatrogenic [doctor-induced] brain death.”
The American College of Physicians recommended in 2021 that the practice of NRP be paused, as "the burden of proof regarding the ethical and legal propriety of this practice has not been met." Other nations, such as Australia, have banned NRP altogether. But despite ongoing ethical concerns, this type of organ harvesting is continuing and expanding in the United States, with half of the country’s organ procurement organizations already participating.
How many families would give their loved ones over to transplant teams if they knew the grisly reality taking place behind operating room doors? While professionals debate the ethics of NRP, people continue to sign their donor cards in ignorance of these facts. Refuse to be a registered organ donor.
Annelise Camp is scheduled to undergo brain death testing — over her family’s objections — today at 9AM CST.
“Because of the lack of high-quality evidence on the subject,” the American Academy of Neurology’s (AAN) brain death guideline was based, not on science, but on 3 rounds of anonymous voting.
Hmm…We’ve been declaring people to be “brain dead” for nearly 60 years…wouldn’t you think there’d be some high quality evidence for it by now?
In the absence of evidence, the AAN guideline was based on the shared biases of a panel of experts which was screened to exclude anyone who might disagree. About 30% of these experts reported a specific conflict of interest with the transplant industry.
The brain death examination consists of a series of bedside tests, because the guideline states that all ancillary tests (EEG, brain blood flow studies, brain scans) have shortcomings, and are not 100% sensitive and specific for brain death.
First, the patient is checked for unresponsiveness, because doctors have no tests for inward awareness: we can only test whether people are able and willing to respond, which is not the same thing. This is not really a fair test because many brain-injured people have cord compression and are unable to respond. Also, a recent NEJM article found covert consciousness with advanced testing in 25% of people who doctors believed to be unconscious.
Second, there should be no motion after a painful stimulus. But certain motions (lifting a limb off the bed, reaching with both hands toward the throat, opening eyes when the nipples are brushed) are allowed as “reflexes.” The guideline admits that it can be difficult to distinguish between volitional and reflex movements, and actually advises asking a friend if you are in doubt, showing the subjective nature of this assessment.
Third, whereas the legal definition of brain death requires the irreversible cessation of all functions of the entire brain, including the brain stem, the brain death guideline just checks a few brain stem reflexes. The guideline also explicitly states that brain death may be declared in the presence of ongoing brain function, in defiance of the law in most states.
Fourth, the patient is disconnected from their ventilator and observed for breathing. The guideline states that parameters for this test are ARBITRARY because there is no scientific data to justify the parameters recommended by the guideline.
So, today for Annelise, (and daily for many other patients around the world) life and death decisions will be made on the basis of an unverified and arbitrary exam for which there is no high-quality evidence.
Brain death is based on pseudoscience. It is an ethical choice masquerading as a medical fact.
@TXRightToLife@SteveTothTX@KenPaxtonTX@MaryBowdenMD@Fynnderella1
You are absolutely right: whether a person is dead or alive is an objectively recognizable fact, and is not dependent on the faith they practice.
Brain death standards also vary between countries, which makes whether you are determined to be dead or alive a matter of your geography.
In reality, “brain dead” people — irrespective of their religion or geography — are neurologically injured and not actually dead.


















![heidiklessigmd's tweet photo. NRP organ harvesting: first they stop your heart, then they clamp off the blood flow to your brain (to make you brain dead on purpose), then they restart your heart in your own chest to be sure it’s in good shape to put into somebody else.
In the never-ending quest for viable organs, doctors have found a macabre new way to skirt both the brain death and circulatory death criteria. Transplant centers around the country are removing people who have signed a DNR order from life support, waiting for their hearts to stop, and then immediately clamping off the blood flow to their brains to make them brain dead on purpose. Then their organs are resuscitated, but the person doesn’t wake up because the circulation to their brain has been clamped off. The protocol for this procedure, called normothermic regional perfusion (NRP) from the University of Nebraska notes: “The initial step for ligation of the blood vessels to the head is necessary to ensure that blood flow to the brain does not occur. Once blood flow to the heart is established, the heart will start beating.” How dead are you if doctors can re-start your heart in your own chest?
Lauris Kaldjian, MD, PhD, director of the program in bioethics and humanities at the University of Iowa Carver College of Medicine writes, “NRP represents a technologically elaborate attempt to refashion definitions of death to maximize the number and quality of transplanted organs. It both depends on and violates the circulatory definition of death and arguably employs iatrogenic [doctor-induced] brain death.”
The American College of Physicians recommended in 2021 that the practice of NRP be paused, as "the burden of proof regarding the ethical and legal propriety of this practice has not been met." Other nations, such as Australia, have banned NRP altogether. But despite ongoing ethical concerns, this type of organ harvesting is continuing and expanding in the United States, with half of the country’s organ procurement organizations already participating.
How many families would give their loved ones over to transplant teams if they knew the grisly reality taking place behind operating room doors? While professionals debate the ethics of NRP, people continue to sign their donor cards in ignorance of these facts. Refuse to be a registered organ donor.](https://pbs.twimg.com/media/Gva4VH8XgAAQBBm.jpg)