We're so excited to welcome our amazing upcoming cardiology fellows for 2024-25! Welcome to the 🫀 family! Can't wait for you to get started ☺️ @DellMedCardio@DellMedCardio#MatchDay
Exciting day for Ascension Texas EP with EP Fellow and future partner @joshuadavisdo helping perform first AF Ablations done at ASMC Hays. Lots of work and planning by so many to make this such a success. The future is bright.
Great persistent AF case with #TactiFlex a few weeks ago with @Hong_CCEP. Safe and efficient with stable and predictable 50W lesions with first pass isolation. Great mapping and support as always by @cassi_g_ep and @ryan_OTman. @DellMedCardio
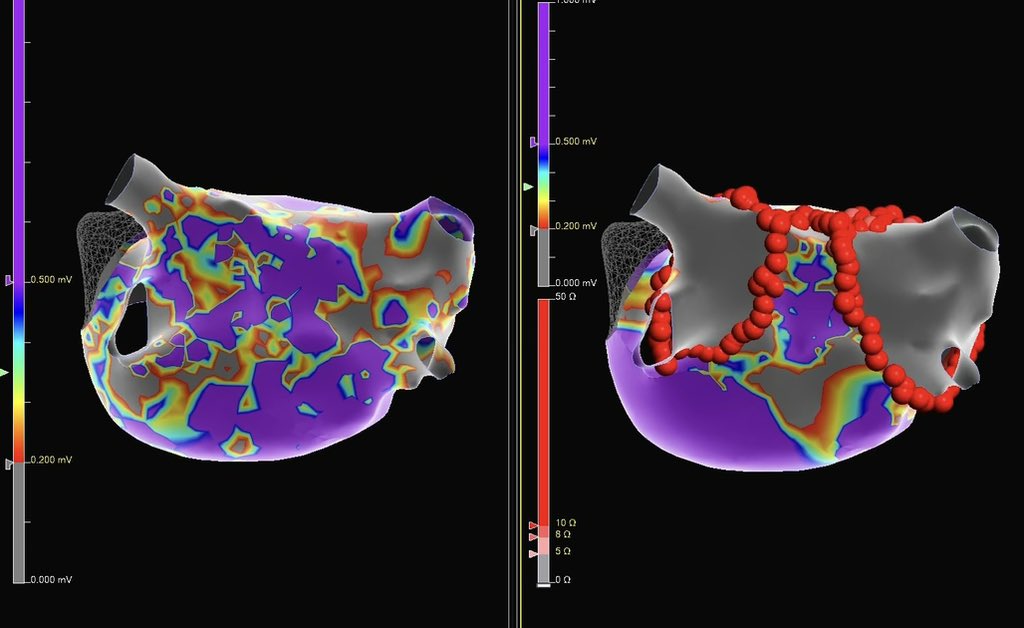
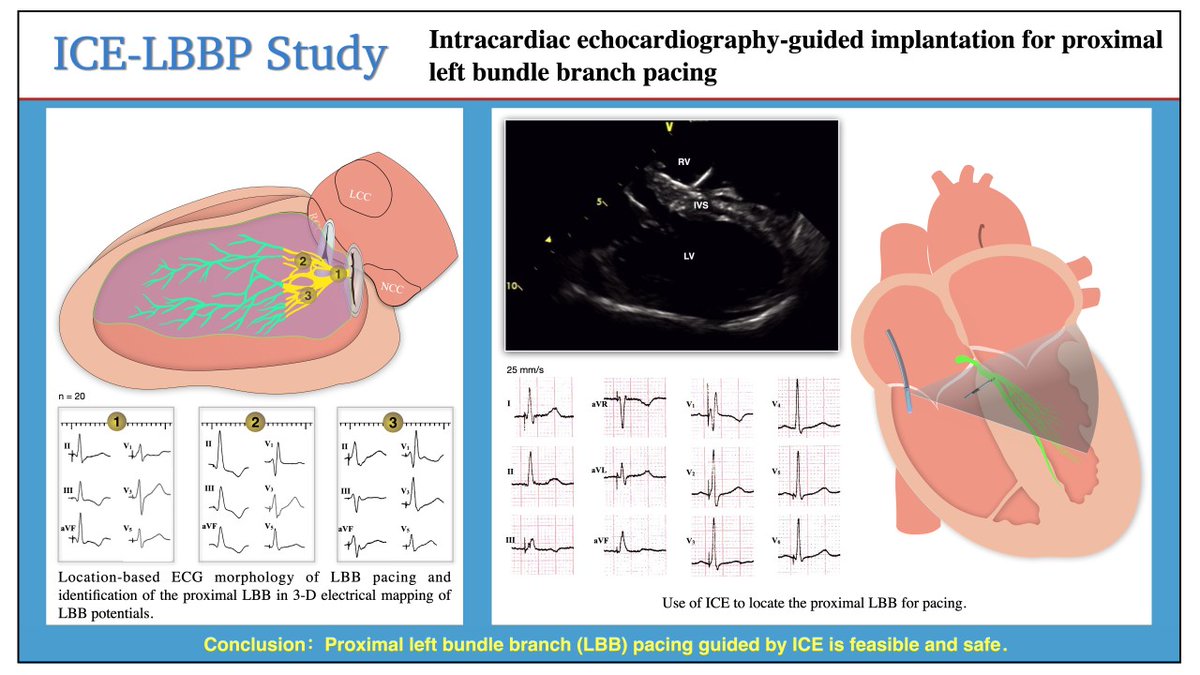
This study demonstrates that the intracardiac echocardiography-guided implantation of proximal left bundle branch pacing is feasible and safe @MdHuang#AHAJournals#Epeeps https://t.co/UqZ0DKwbOW
@RichardAFerraro I tell fellows that we should never forget that we cath in a “laboratory”… we study things… we try new things… clinical trials may slow down the day a bit… but the daily work of the lab is almost as much about tomorrow as it is about today. @DellMedCardio@DellMedSchool@SCAI
Our PGY-6 fellow @doctormontano sharing a complex structural case at #SCAI2022 fellows course- key takeaways:
➡️ a multidisciplinary heart team approach is critical
➡️ think outside the box- novel solutions for challenging scenarios
#whatstartshere#CardioTwitter
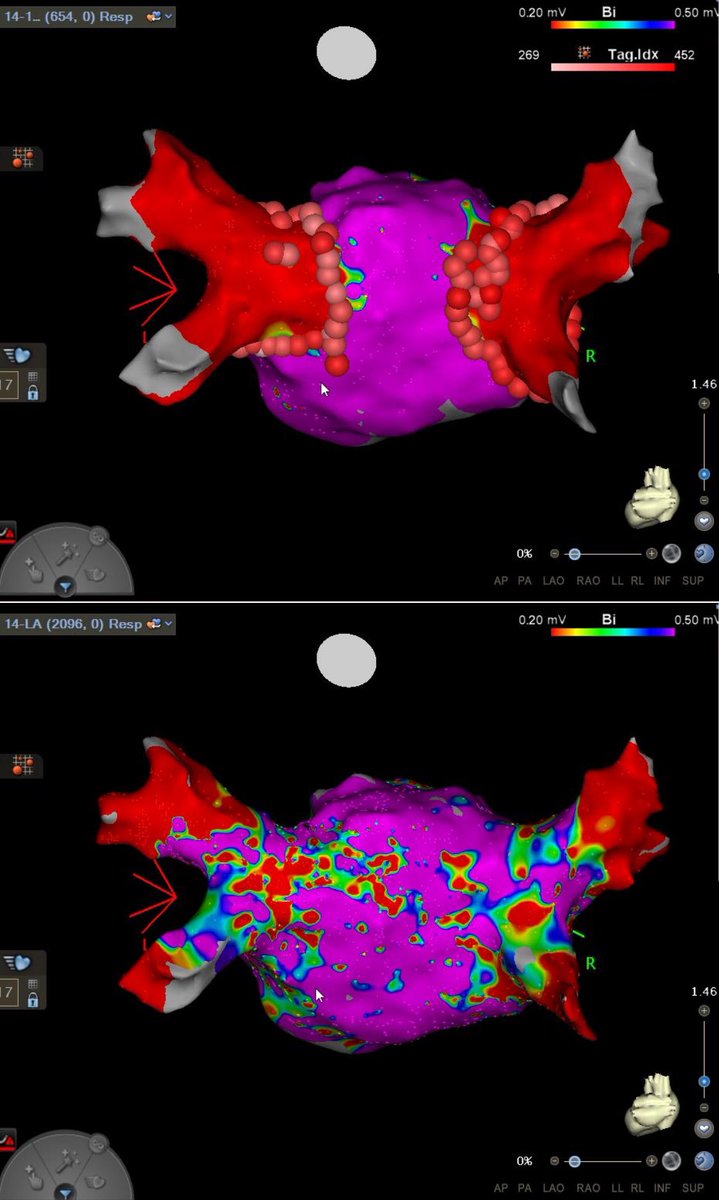
A typical atypical flutter. Hx of CHF and PersAF s/p prior PVI - roof line and anterior Mitral line. Terminated on the roof very quickly and confirmed block of veins and lines.
@sgreenbergmd Will occasionally see higher HRs post PVI usually from normal to 90s or 100s. Those patients quite anecdotally seem to respond well to PVI. They also seem to return to baseline HRs in 6 - 12 months so may not be out of the woods for a pacemaker. Be interesting to follow.
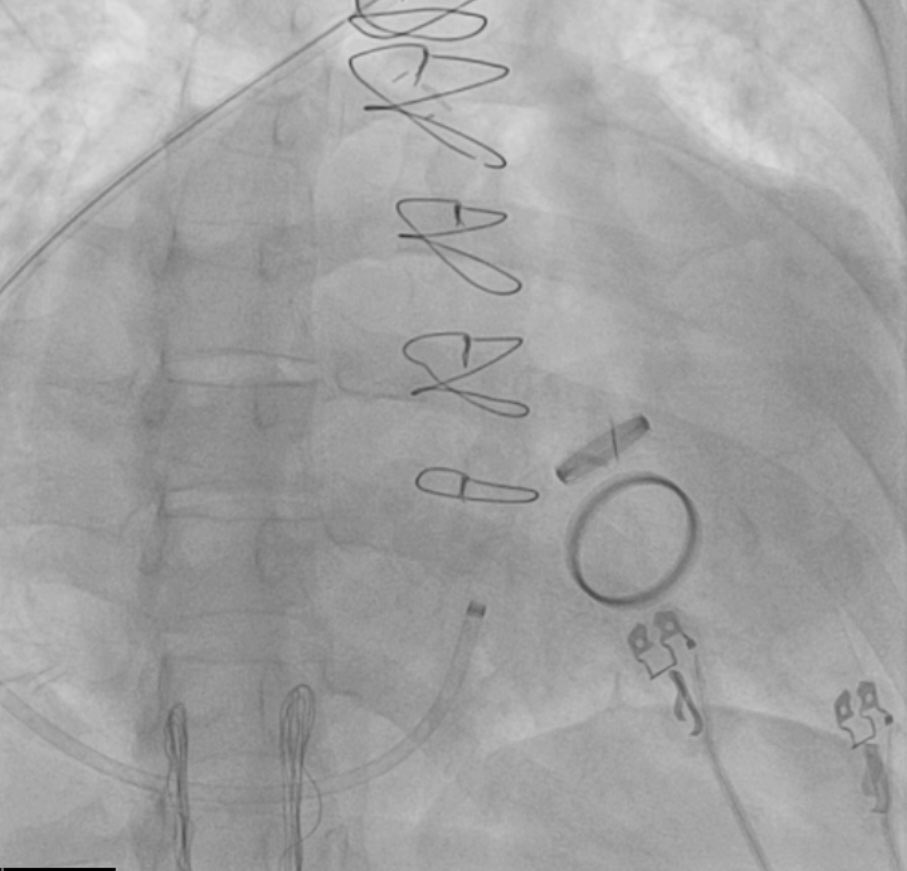
@AllenAmornMD@EPeeps_Bot Thanks. We used a DF4, are asking about dual coil? I am worried about DFT. He had some lower INRs recently so didn’t shock today and will have to bring him back. Don’t mind letting that lead settle in place for a bit either.
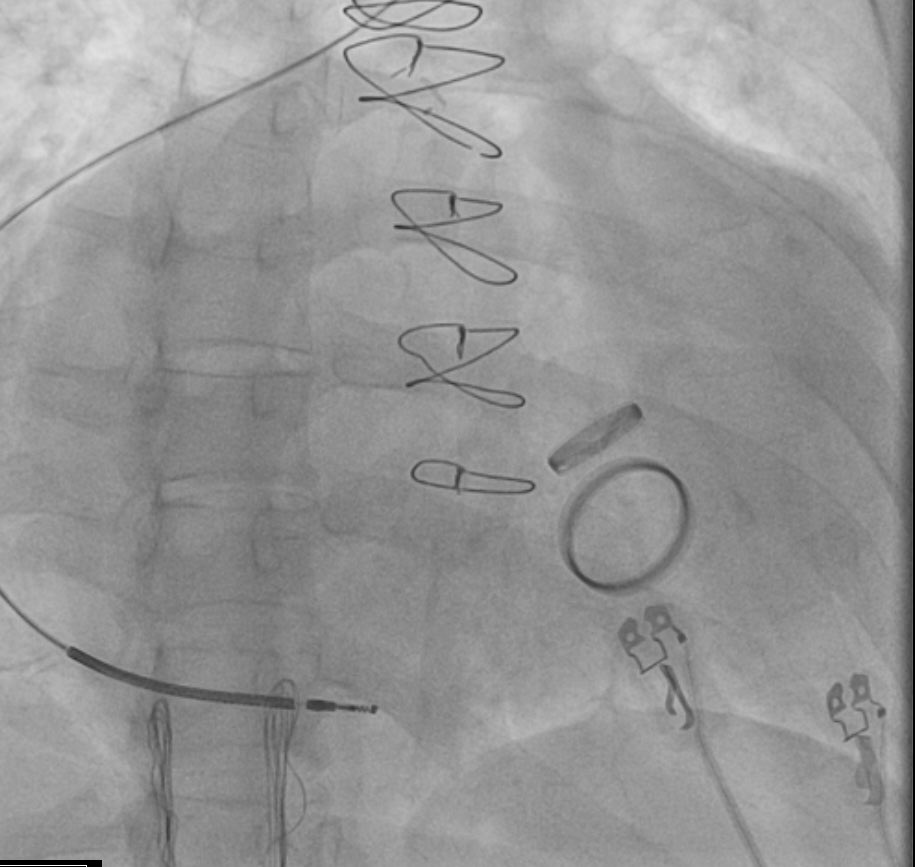
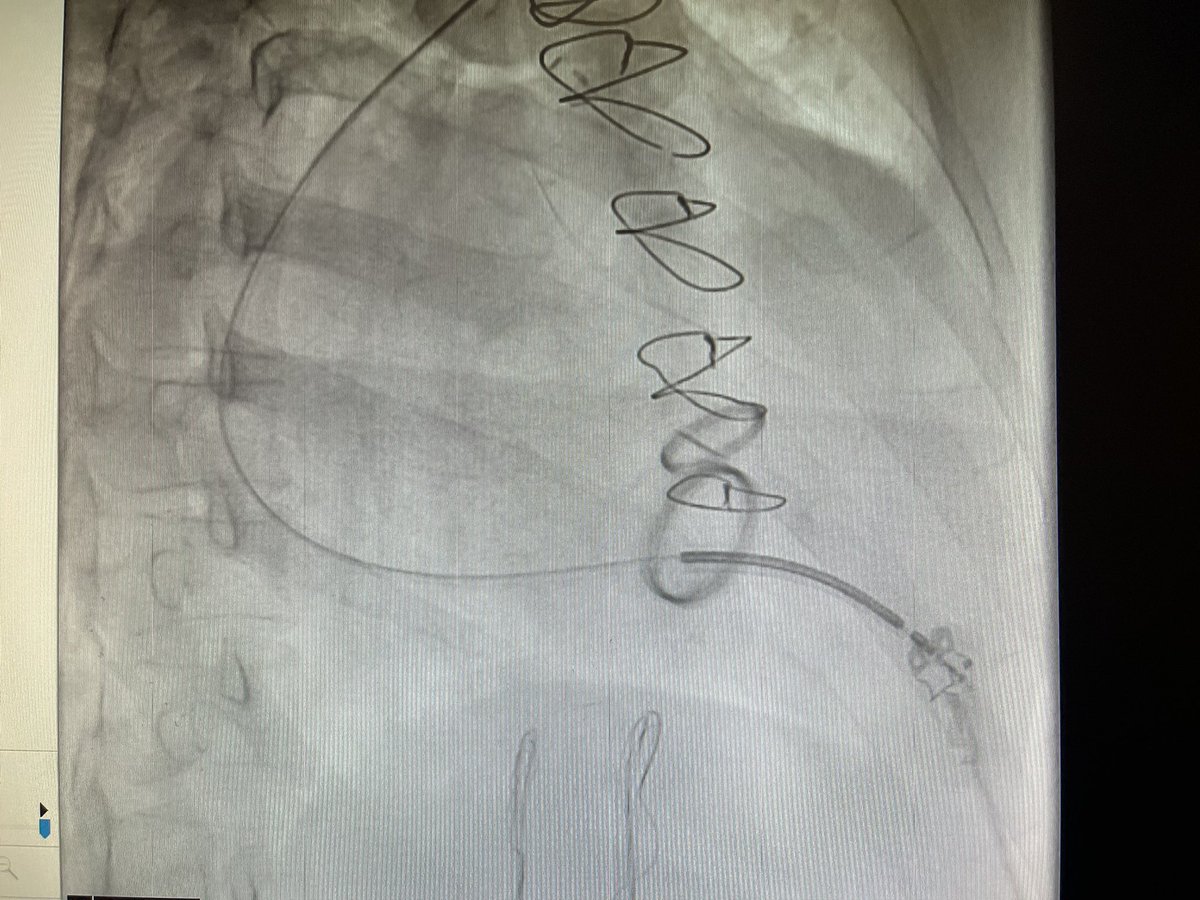
Eventually had to use a curved stylet that started the curve right at the RA/SVC junction and directed straight down to get the RV Apex/Low Septum. Great stability and numbers. What are other tricks?
Go to for severe TR is to use a Worley sheath to get bast the valve and achieve stability however it rode the back wall of the massively dilated atrium and the large could not reach the valve.