@cameron_baston My approach to this is to find a patient who definitely will have B lines (e.g. missed hemodialysis) and try all transducers and presets to identify the best mode for the machine. Then use that going forward
Excellent! "The question is beginning to transition from whether one should learn [lung ultrasound] to a question of if it is possible to justify continuing to use the inferior diagnostic modality of CXR for patients?"
I recently tried to explain the anion gap to someone... And really struggled.
Here’s an update of the gamblegram graphic from @thecurbsiders’ acid-base episode, in case anyone else has as hard of a time as I did!
#MedStudentTwitter#NephTwitter
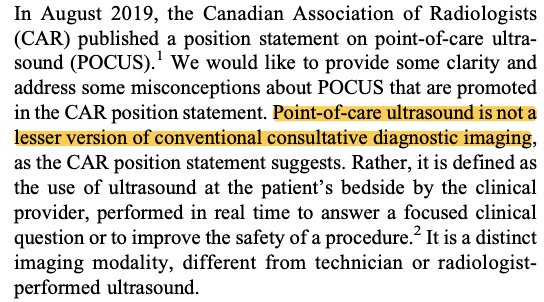
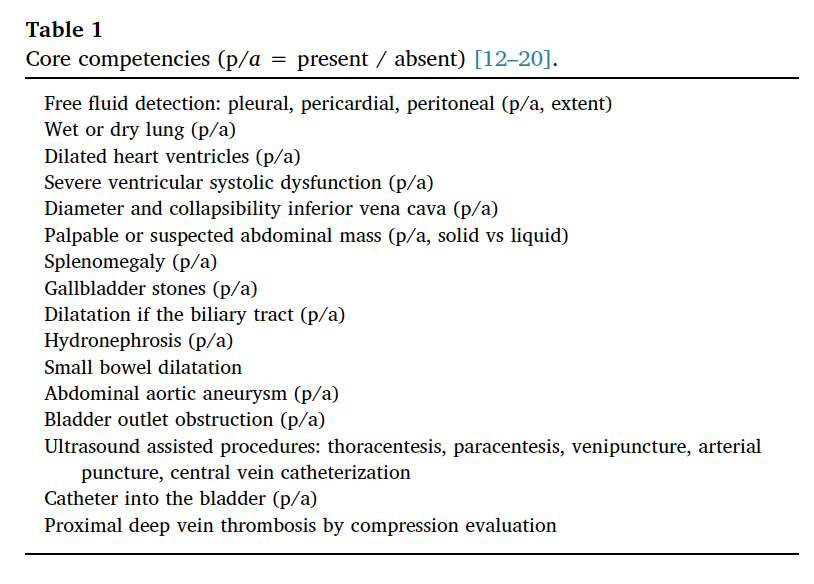
Core Competencies for #IMPOCUS published by European Federation of Internal Medicine. Congrats @jtorresmacho for leading the effort to advance #POCUS in Europe https://t.co/DJe0LdeeHo
@TheCaseyGlass @G2Disrupt@DRsonosRD@SonoInternist Depends on responsibilities. If just residents maybe 0.1, add more time for training faculty, med students, or fellowship.
Point-of-Care Ultrasound for Internal Medicine Residency Training: A Position Statement from the Alliance of Academic Internal Medicine https://t.co/wacve1R9C4
That’s a wrap—Thanks to this crew for making the AIUM’s 1st POCUS Hands-on Training Course for Beginners a success! Look out for recaps next week on LinkedIn & Facebook.
Our focused cardiac ultrasound learner core doc by @HeartDocSharon@shanearish Drs. Sarah Weeks and Kristin Lyons is now online #CIMUS#IMPOCUS: https://t.co/WiuVvyfPuL Or you can find it on https://t.co/0DVLZRUJDC under the cardiac tab.
@cameron_baston But what if I enjoy relying on the same physical exam findings and imaging modalities that were available in 1897? It makes me feel adventurous and sophisticatedly retro...































![UltrasoundJelly's tweet photo. Major https://t.co/ZBKn5yjoZS upgrade today. Highlights include:
1) tagging system to track over-reads, quality, and diagnosis
2) stats page summarizing data [sens/spec/acc]
3) new archive thumbnail view 4-10x faster loading
4) archive multi-share
#FOAMed https://t.co/3bTzKNTSww](https://pbs.twimg.com/media/EIIBkKCWwAIbbls.jpg)




















