C'mon @WIRED, you have a chance to do better. Instead of amplifying pseudoscience, why not talk to the patients living with #LongCovid and the researchers studying its biology? Levinovitz is not a physician, neuroscientist, or virologist. His expertise is in religion. Try again!
Research progress on the association between viruses and cardiac diseases
🚨Your heart’s deadliest serial offender just got named: SarsCoV2
Interesting Chinees review just mapped how six viruses attack the heart.
One stands out!
Not because the authors scream “worst ever,” but because the science does.
→Direct heart-cell invasion + long-term damage + cumulative hits from regular reinfections = a unique threat!
Vaccines help. But the data is sobering.
Let’s break it down virus by virus(review):
1. SARSCoV2:
- Enters cardiomyocytes and pericytes via ACE2 receptor (membrane fusion/endocytosis).
- Direct infection triggers myocarditis, pericarditis, arrhythmias, heart failure (de novo or exacerbation), microclots, thromboembolic events and myocardial infarction,
- Long-term: persistent cardiac inflammation, dysautonomia and long-COVID cardiovascular symptoms,
- Possible viral persistence in tissue,
- Vaccination reduces myocarditis risk/CV complications compared with natural infection,
-Regular reinfections!
2.Influenza (A/B):
- Direct replication in cardiomyocytes, Purkinje cells and endothelial cells (independent of lung titers),
- Causes myocarditis, pericarditis, arrhythmias, heart-failure flares and myocardial infarction via both cytopathic effects and cytokine-driven systemic inflammation/endothelial dysfunction.
- Long-term: myocardial fibrosis and remodelling,
- Vaccines lower infection-related cardiovascular complications,
3. HIV:
- No productive cardiomyocyte infection,
- Indirect damage from chronic immune activation, endothelial dysfunction, metabolic changes and antiretroviral toxicity,
- Drives cardiomyopathy (myocarditis in advanced cases), heart failure, myocardial infarction and stroke,
- Long-term: premature cardiovascular aging, fibrosis and remodelling even on suppressive therapy,
4. CVB3 (Coxsackievirus B3):
- Enters via CAR receptor,
- Direct cytopathic necrosis, oedema and impaired contractility in cardiomyocytes,
- Rapid progression to myocarditis, dilated cardiomyopathy, arrhythmias (QTc prolongation) and heart failure,
- Chronic inflammatory cardiomyopathy is a hallmark sequela,
5. Human cytomegalovirus(HCMV):
- Lifelong latency with reactivation (especially in immunocompromised),
- Induces myocarditis, heart failure, transplant vasculopathy and atherosclerosis through sustained inflammation and vascular injury,
- Long-term myocardial remodelling,
6. Arthropod-borne viruses(Arboviruses = DENV, CHIKV, ZIKV):
- Direct cardiac invasion (some models) plus immune-mediated injury,
- Associated with myocarditis, arrhythmias, heart failure, shock and (CHIKV) dilated cardiomyopathy or long-term ischemic heart disease/cerebrovascular risk.
‼️So, this minireview examines six cardiotropic viruses side-by-side, yet SARS-CoV-2 receives the most space because of its proven direct cardiomyocyte invasion, explosive multi-pathway damage, and documented long-term cardiac persistence, risks that broader population data show accumulate relentlessly with every regular reinfection, creating an immediate and chronic cardiovascular burden on a global scale that no other virus in this review matches.
→Your heart’s deadliest serial offender just got named: SarsCoV2!
#PREVENTION #COVIDHeart #RepeatInfectionKills #AvoidSars2 #AvoidReinfections #YouOnlyHaveOneHeart
https://t.co/BPKRV7nwbA
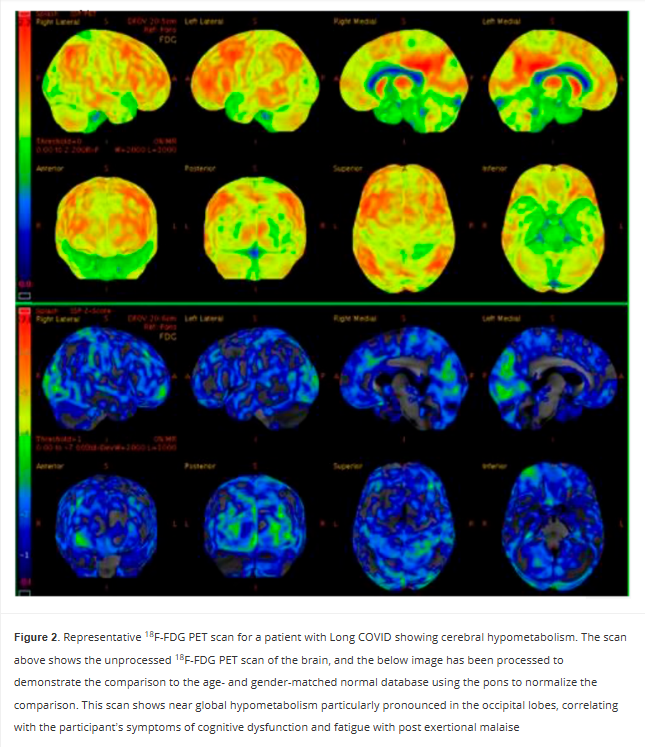
Persistent Cerebral 18-FDG PET Changes in Patients With Long COVID Presenting With Fatigue and Post Exertional Malaise
🚨We already knew Long COVID brain damage could last 6 months.
Now this new PET scan study proves it’s still there at 2 YEARS and counting.
Hypometabolism hits the left sensorimotor cortex (movement + body sense), left superior parietal (spatial awareness + attention), and bilateral visual cortex (raw sight processing).
This is NOT just “tired.”
This is a broken sensory-motor command center.
Is this the start of a lifelong neurological disease?
➡️Mayo Clinic observational cohort study of 40 Long COVID patients (70% female, median age 53) from a specialized clinic who underwent brain 18F-FDG PET-CT scans 17–149 weeks (median 62 weeks) after SarsCoV2 infection,
➡️73% had predominant fatigue with post-exertional malaise (PEM),
➡️This group showed statistically significant cerebral hypometabolism vs. non-PEM patients in the left sensorimotor cortex (p=0.0253), left superior parietal cortex (p=0.0276), and bilateral primary visual cortex (p=0.0096 and 0.0016),
➡️Abnormalities persisted already up to ~2 years post-infection,
➡️Scans used pons-normalized Z-scores against age/gender-matched controls with common comorbidities included psychiatric, GI, and cardiovascular conditions,
➡️Caveat: No references to vaccination status and/or reinfections,
➡️Authors propose 18F-FDG PET-CT as a potential diagnostic and therapeutic biomarker for the fatigue/PEM phenotype of Long COVID.
‼️So, AGAIN, Long COVID fatigue and PEM have a demonstrable, persistent neurological signature! Cerebral hypometabolism, still detectable on PET scans up to two years later and hits the left sensorimotor cortex (movement + body sense), left superior parietal cortex (spatial awareness + attention), and bilateral primary visual cortex (raw sight processing).
This isn’t just “tired.”
It’s a broken sensory-motor command center.
😡Study proves LC is biologically real, not psychosomatic or any other stupid FND diagnosis.
Without urgent validation of this biomarker and targeted therapies, patients will continue to be dismissed despite objective brain damage!
#AvoidSars2 #AvoidReinfections #BrainDamage
https://t.co/OfoOlgDyt0
Early treatment in the upper respiratory tract may help prevent neuroinvasion.
Nasal and oral sprays/rinses reduce risk for COVID-19 as shown in extensive clinical data, including 65 randomized controlled trials: https://t.co/TIFIqV4ovO
Mechanisms of action include virucidal effects, blocking viral attachment, creating a physical barrier, physical removal, and enhancing mucociliary clearance. Combined nasal and oral application is most effective.
Proposed mechanisms for SARS-CoV-2 entry into the CNS include: the olfactory route, traveling along or alongside olfactory nerve fibers through the cribriform plate; the nervus terminalis, whose fibers also cross the cribriform plate into the forebrain; retrograde transport along other cranial nerves, such as the vagus or trigeminal; the hematogenous route, which involves crossing or disrupting the blood-brain barrier; the "Trojan horse" mechanism via infected immune cells; and direct infiltration at more permeable sites like the choroid plexus or circumventricular organs.
Halting replication in the upper respiratory tract prior to progression may help avoid a cascade of potentially severe outcomes.
Caolan Robertson is probably the best investigative journalist on X right now - follow him!
Also huge thanks to NAFO and Irish investigative journalists digging deeper into this case.
Rusal needs to go!
I keep seeing people saying "I don't believe the data that says there's not much Covid around, there are loads of stories of people catching it at the moment".
Yes, but you're not seeing *as many* stories of people catching it at the moment.
Yes, it's around. Low Covid does not mean No Covid.
But here in the UK *every single possible metric* is indicating that there are historically low levels. We're still doing 20k PCR tests in England each week as a base level, plus more when there are more cases. Scotland has wastewater.
Tests, cases, admissions, deaths, wastewater, positivity are all tracking at the same rates - and it's very hard to manipulate one without manipulating all of them, and there's no need to, because 99% of the population don't care what the levels are.
I buy and hand out tests to people in our local community myself. The positives on those tests track quite closely to national numbers.
Some people are then arguing that it means that tests aren't picking up cases.
Well, that doesn't make sense either, because we've just had a wave that hit kids here, and the tests picked those up fine.
The final thing is:
What does low mean?
'Low' in terms of Covid doesn't mean *none*.
There are more Covid cases confirmed at the moment each week than Measles cases... but Measles cases are 'High'.
Covid cases are *low for Covid*.
Low Covid does not mean No Covid.
It just means that it's not overwhelming healthcare right now.
Low Covid does not mean that I'm stopping masking, or stopping any other mitigations that I've had in place for six years. It just means that there's not as much around as at other times.
Which would be a particularly daft time to catch it.
There are hundreds of thousands of publications on SARS-CoV-2 infection. They demonstrate multi-system pathology in acute and Long Covid through some of the most sophisticated scientific approaches in medical history.
These are irrefutable facts.
Ignorant scientists just dropped a 'post-pandemic diabetes' paper that pretends COVID-19 vanished in 2023.
Title screams “COVID-19’s Lasting Impact” yet the entire analysis dodges the elephant:
→ SARS-CoV-2 is causing new-onset diabetes in millions,
→ Science papers: 1.37% incidence in infected patients, 40%+ higher risk persisting 3–12 months, beta-cell destruction, chronic inflammation,
Global Burden of Disease (GBD) numbers didn’t magically accelerate, because of the “pandemic,”
SarsCoV2 is still driving them,
Calling it “post-pandemic era” while ignoring the active viral trigger isn’t science, this is wilful blindness,
This is how you gaslight a global metabolic catastrophe!😡
Wake up!!
#COVIDDiabetes #ScienceFail
https://t.co/R5gkb8OZf4
Child can recover from COVID.
Their routine tests can look normal.
Yet more sensitive testing may still detect abnormalities in the lungs, immune system, quality of life, and possibly even the heart.
A new review from Taiwan's DISCOVER cohort helps explain why🧵
Truly morally sickening: that anyone should wish all of Ukraine to suffer the fate of Mariupol or Bucha. Russian occupation of Ukraine means random arrests, executions, concentration camps; the destruction of language and culture; mass kidnapping of children. All of these things have been documented in the occupied territories and continue to go on.
Remember the pig heads at the Paris mosques? Or the Jewish centers painted green?
I knew exactly whose work it was the moment I saw it. Now — I finally have the proof. 🧵 [1/19]