The human body has lessons to teach all of us in medicine. As a hematopathologist, I’m especially partial to the bone marrow. During my 2026 commencement keynote at Loyola University Chicago Stritch School of Medicine, I shared how the marrow models attentiveness, responsiveness, connectedness, adaptability, and resilience in ways that medicine should never forget.
Here’s a snapshot of a few of those lessons.
@LoyolaStritch@UMichPath@umichmedicine@UMichRISE@UMichMedSchool
A huge congratulations🎉 to Zubair Baloch, MD @aakasharmand for receiving the @PapSociety Lifetime Achievement Award last week at #USCAP2026! The award is a testament to his outstanding dedication and the significant impact.
We are fortunate to have him on our team!
Today is the last day of #USCAP2026 and it has been one of the best! Huge congratulations to the full Penn Path & Lab team for all of your presentations and talks this year!!
Sometimes, words fall short when trying to express the overwhelming joy and gratitude I feel toward God!
"Bless the Lord, O my soul! " Psalms 103:1
Grateful beyond words for this opportunity and ready to give my best in this next chapter @PennPathLabMed#Match2025#pathmatch2025
🎉Happy Match Day!!🎉
We are so exited to welcome our new class of PG1-Y residents to Penn Pathology and Laboratory Medicine! Congratulations on your match; we cannot wait to have you join us!
#MatchDay2025
Happy Monday everyone!
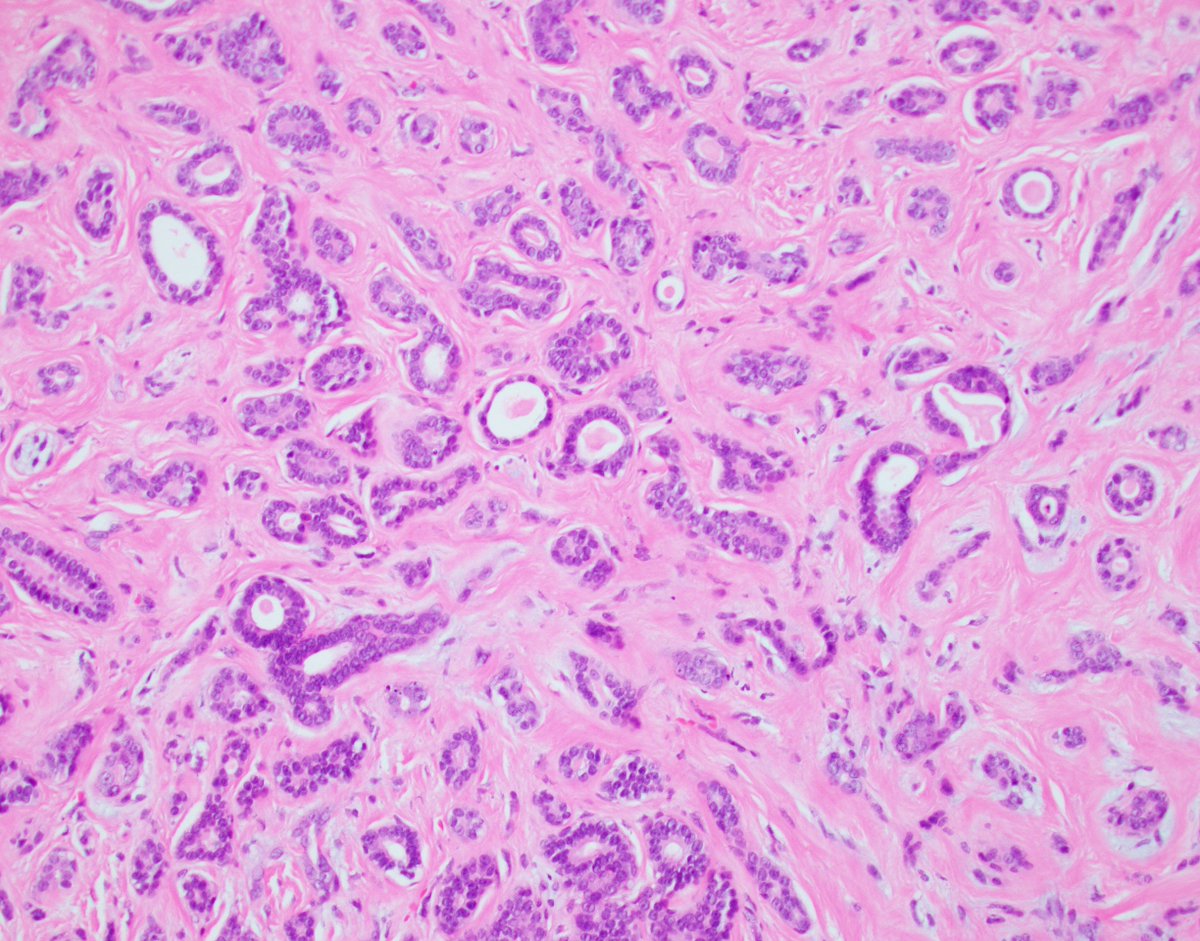
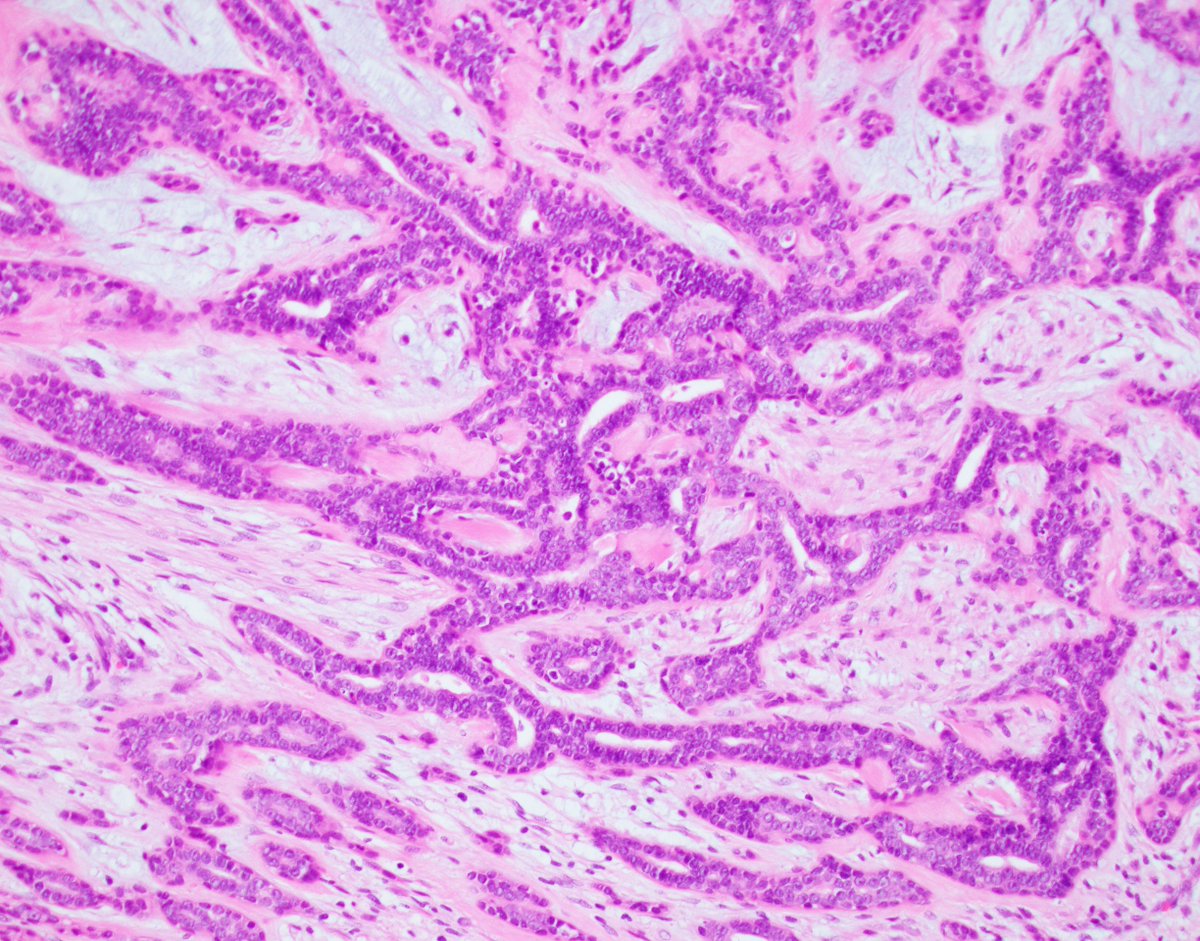
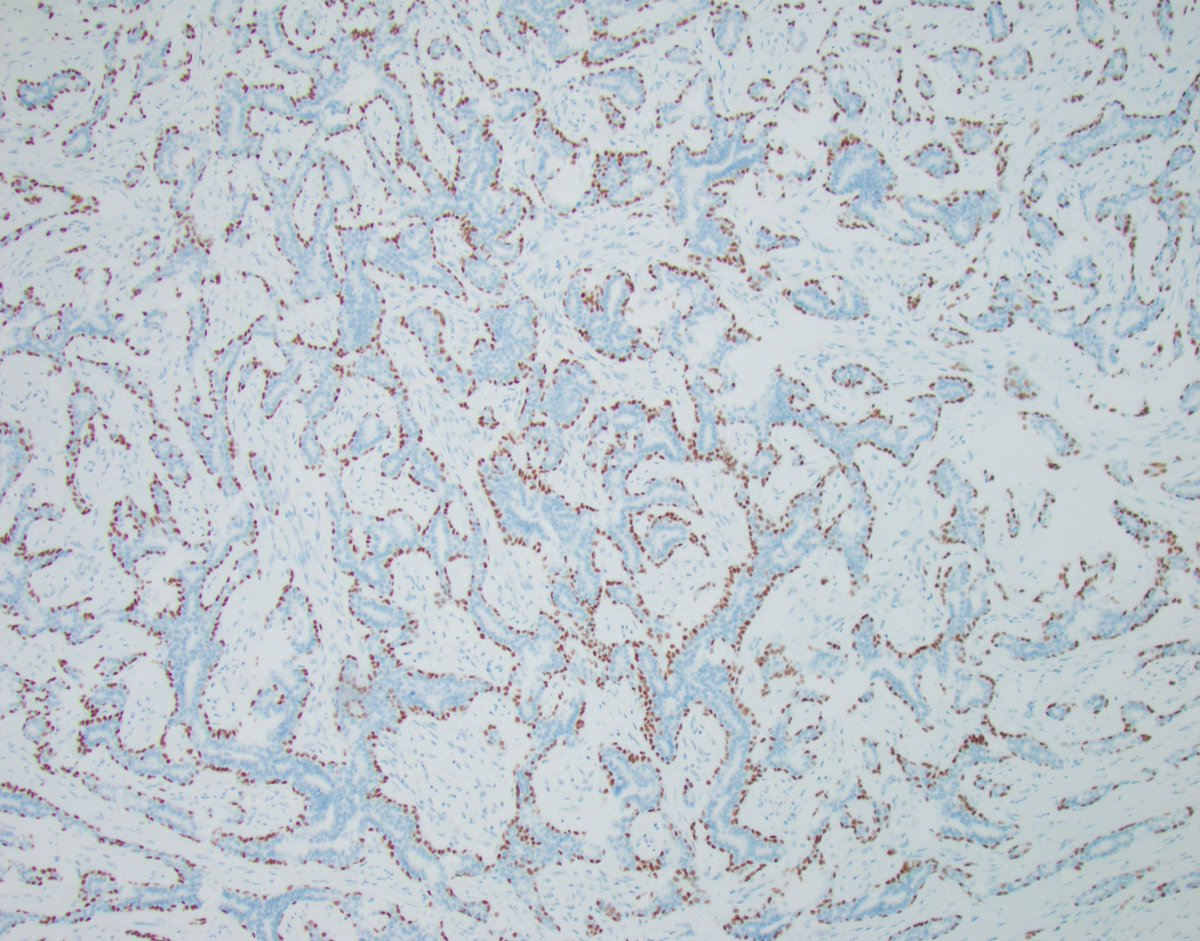
Let's go over case 4 of last week's series of p63 pitfalls. Tomorrow, we will tackle case 5.
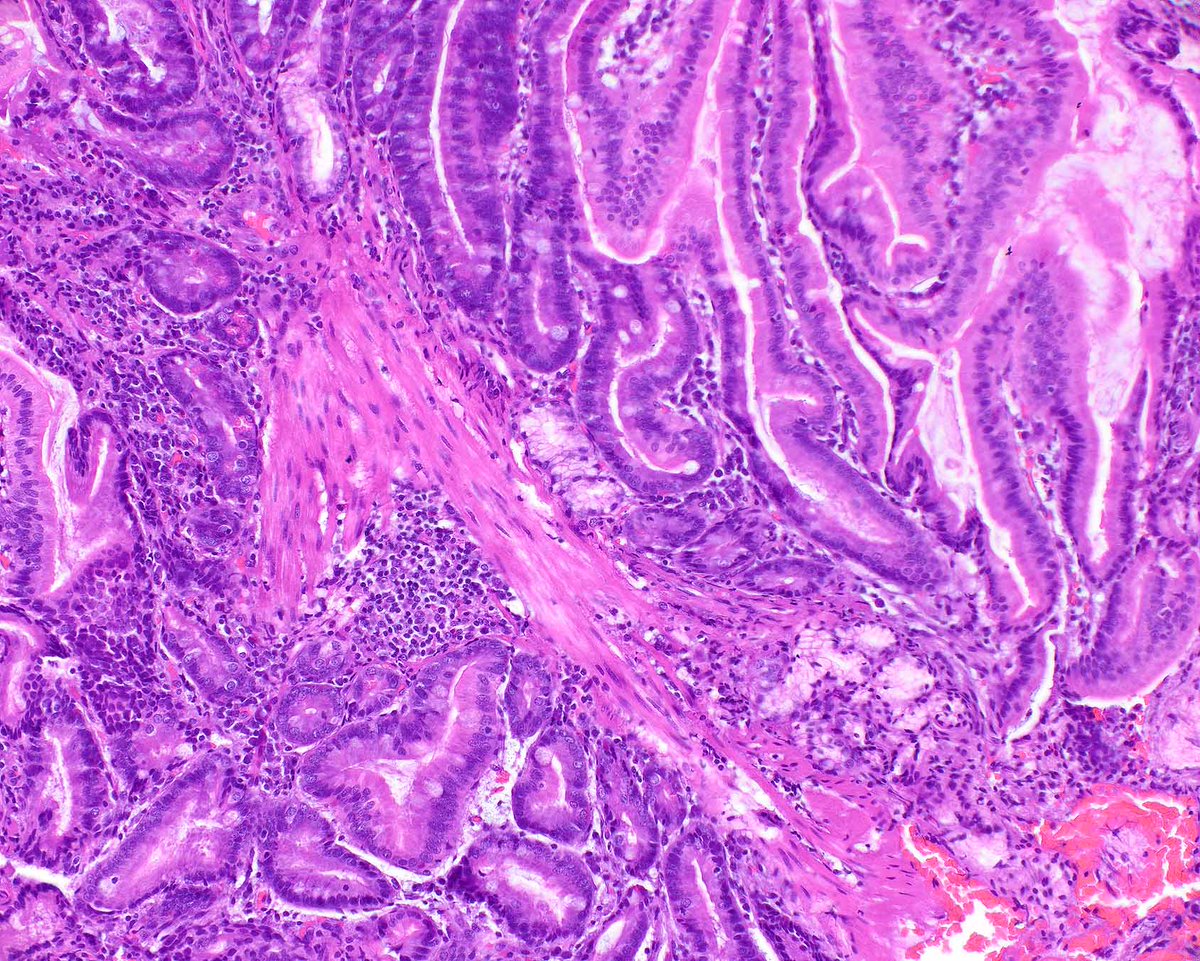
The diagnosis in this case is adenoid cystic carcinoma (ACC), tubular variant, which lacks the classic cribriform architecture of ACC and instead shows small ducts and anastomosing channels with peripheral staining for p63, mimicking a non-invasive process. Helpful features in such cases include absent staining for ER and, if performed, a MYB-NFIB t(6;9) translocation.
Let's address differential considerations:
1. Benign/radial scar/CSL
Radial scars/CSLs are fascinating and treacherous lesions for many reasons. What makes this less likely to be a CSL is the sheer size and anastomosing complexity of the epithelial proliferation, the presence of an infiltrative leading edge of neoplastic epithelium with a stromal reaction associated with it, the absence of a classic fibroelastotic center, and the complete absence of ER staining.
2. Adenomyoepithelioma
The differential here is trickier and the distinction controversial. Part of the difficulty is how diverse and poorly defined adenomyoepitheliomas are, from benign to atypical to malignant to carcinoma arising in adenomyoepithelioma.. a hot diagnostic mess if you ask me. Strictly speaking, I believe ACC is a subtype of the general category of adenomyoepithelioma in its current poorly defined state of affairs. However, there are hints that can help differentiate one from the other, at least in my opinion, and I'm certainly not the authority on the matter.
a. Adenomyoepitheliomas tend to have an atypical population of myoepithelial cells, even if mildly so, meaning that the myoepithelium is conspicuous, the cells are large and the nuclei tend to be hyperchromatic. Almost invariably, there are foci where the abnormal looking myoepithelium seems to pile up and proliferate.
b. Adenomyoepitheliomas are notoriously heterogeneous, often papillary, and both myoepithelium and epithelium show variable degrees of atypia and proliferation. The above ACC, though morphologically complex, tends to maintain a relatively consistent relationship of epithelium and myoepithelium.
c. Adenomyoepitheliomas often show aberrant staining patterns for myoepithelial markers, losing p63 while keeping SMM, partially losing both while keeping CK5/6, etc. This is particularly useful when you know that a cell is myoepithelial by morphology.
d. Adenomyoepitheliomas do not have the recurrent MYB-NFIB translocation. Instead they show mutually exclusive PIK3CA and AKT1 mutations.
e. Finally, in my experience, adenomyoepitheliomas show variable ER positivity. ER-negative adenomyoepitheliomas have been described but they show specific molecular abnormalities and may belong to a separate diagnostic category that requires further elucidation.
3. Epithelial-myoepithelial carcinoma
These classic salivary gland tumors are rarely seen in the breast, and in my experience, are usually admixed with different patterns of biphasic neoplasia. The classic pattern of epithelial-myoepithelial carcinoma consisting of layers of myoepithelial cells with clear cytoplasm surrounding a minor epithelial tubular structure is unmistakable.
4. Low-grade adenosquamous carcinoma
These low-grade triple-negative tumors are also a favorite of mine. They tend to be morphologically diverse as well and can be very difficult to differentiate from benign proliferations. The classic pattern of p63 is usually not just single-layered but often involves the entirety of the gland, together with the characteristic squamoid morphology which gave the tumor its name. No squamous morphology was seen in this case.
Ok. I think I overstayed my welcome and my fingers and pending cases are giving me the evil eye :)
I won't have that much to say about tomorrow's case, but it is nevertheless quite interesting and memorable, in my humble opinion.
See you tomorrow!
@washu_pathology@washupathedu #breastpath #PathTwitter
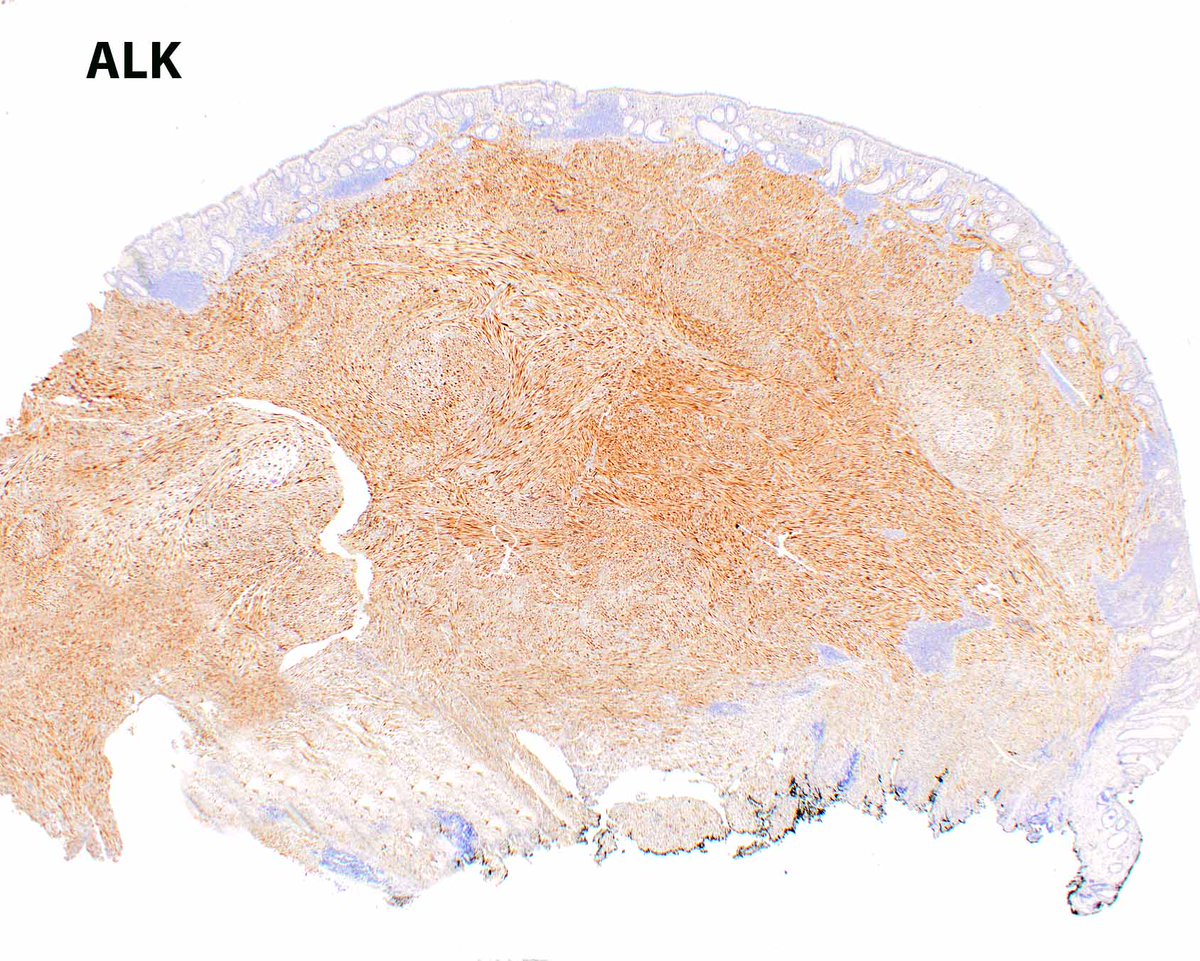
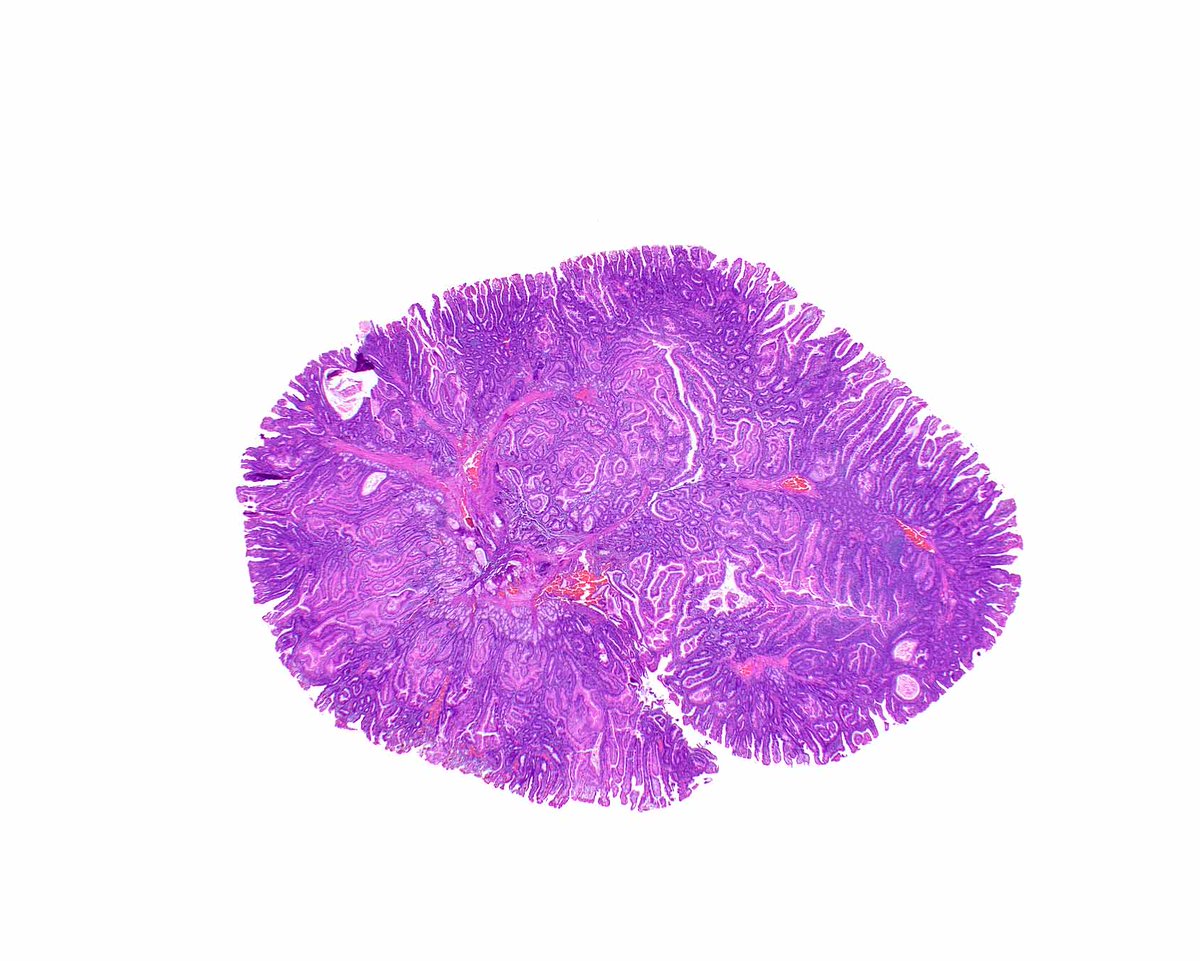
When inflammatory myofibroblastic tumor (IMT) extends into the submucosa and mucosa, it can mimic a gastrointestinal tract schwannoma because of its cuff of lymphoid aggregates. Generally, IMTs are located in the mesentery and schwannomas in the muscularis propria. #UMiamiPath
This classic Peutz-Jeghers polyp of the duodenum shows cords of smooth muscle that partition off zones of site specific mucosa. Detecting even a single such polyp can indicate that a patient has this cancer syndrome.
PMID: 17667545.
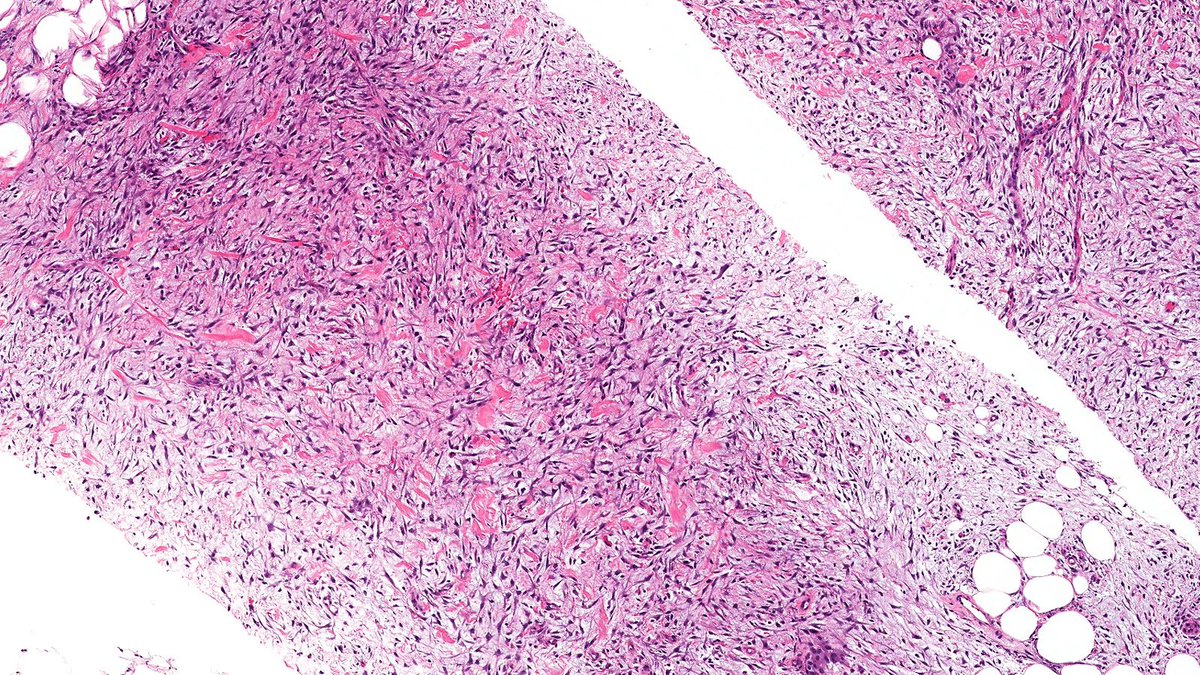
Let’s review some spindle cell breast lesions this week
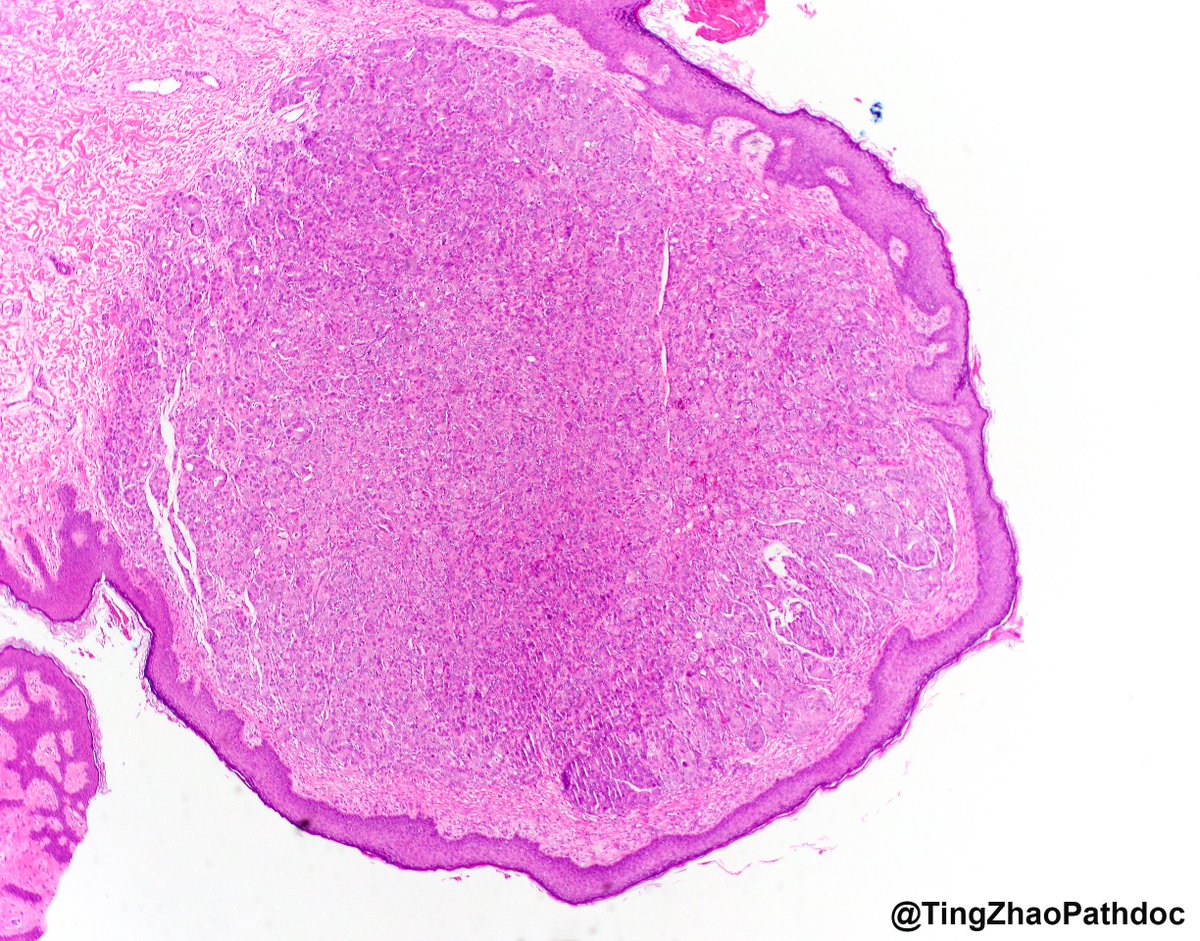
Case of Nodular Fasciitis (NF) 🔬
NF is a self-limited pseudosarcomatous benign neoplasm mimics malignant spindle cell lesions and harbors USP6 gene fusion. NF rarely involves the breast.
#PathTwitter#PathX#breastpath
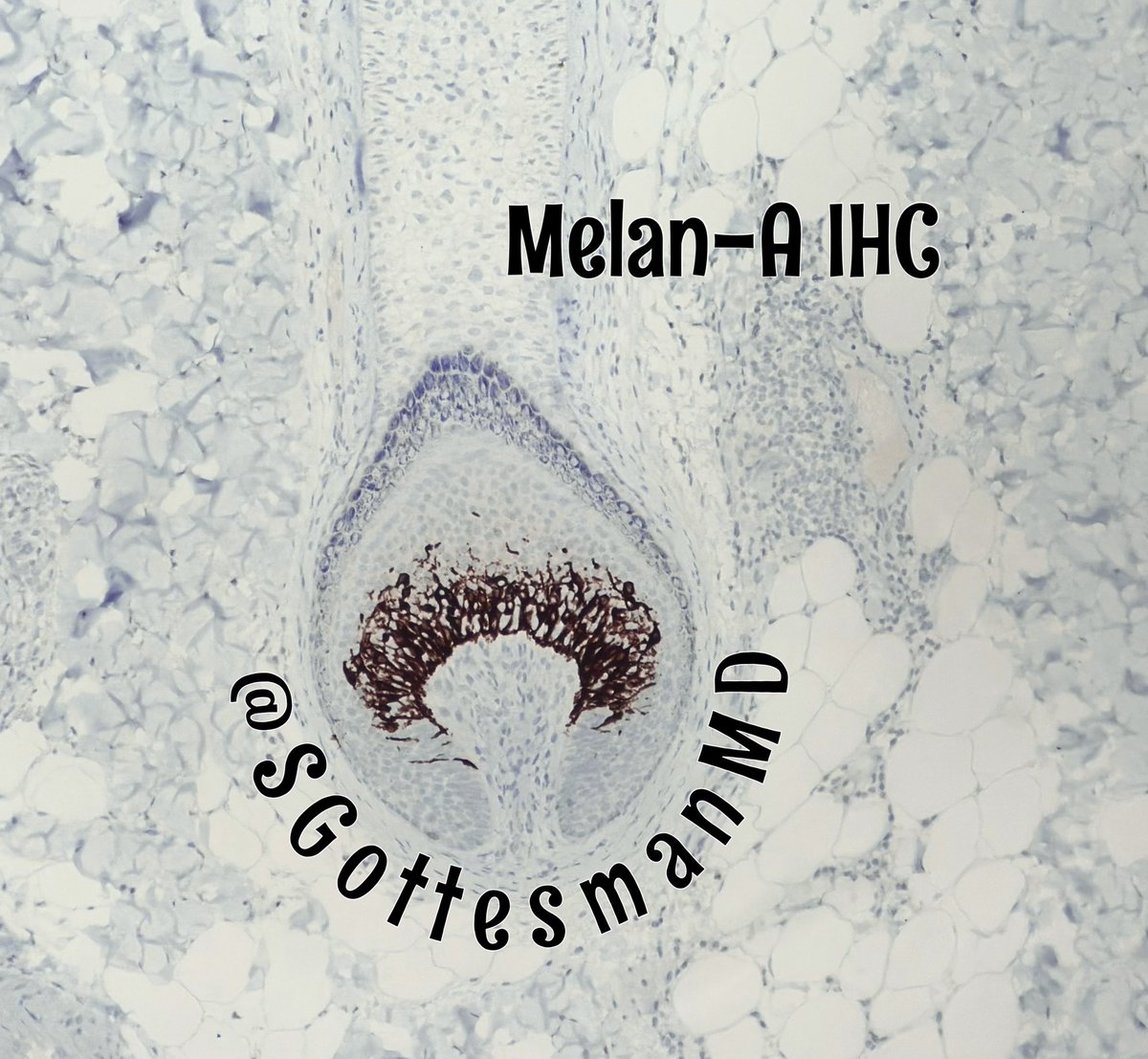
🔹Melan-A immuno stain of a normal hair follicle highlighting melanocytes that are responsible for color of hair shafts
🔹In #AlopeciaAreata, melanocytes get destroyed by the lymphocytic infiltrate, resulting in hair growing in white (colorless) after treatment
#dermpath #alopecia #dermtwitter #pathology #IHCpath
This might LOOK like a metastatic mucinous adenocarcinoma, but it's actually a #glioblastoma. These tumors can be very tricky under the microscope. #pathology#neuropath#PathTwitter
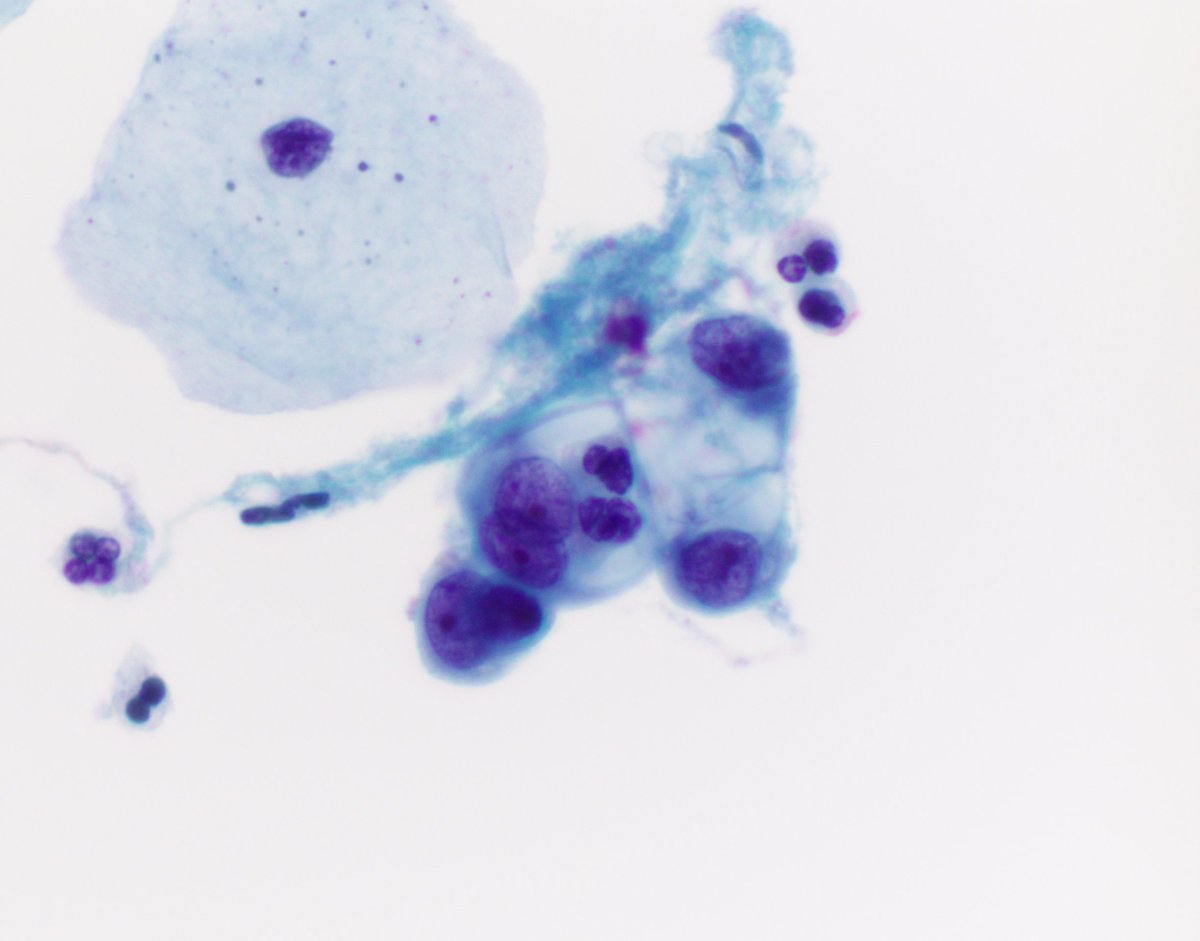
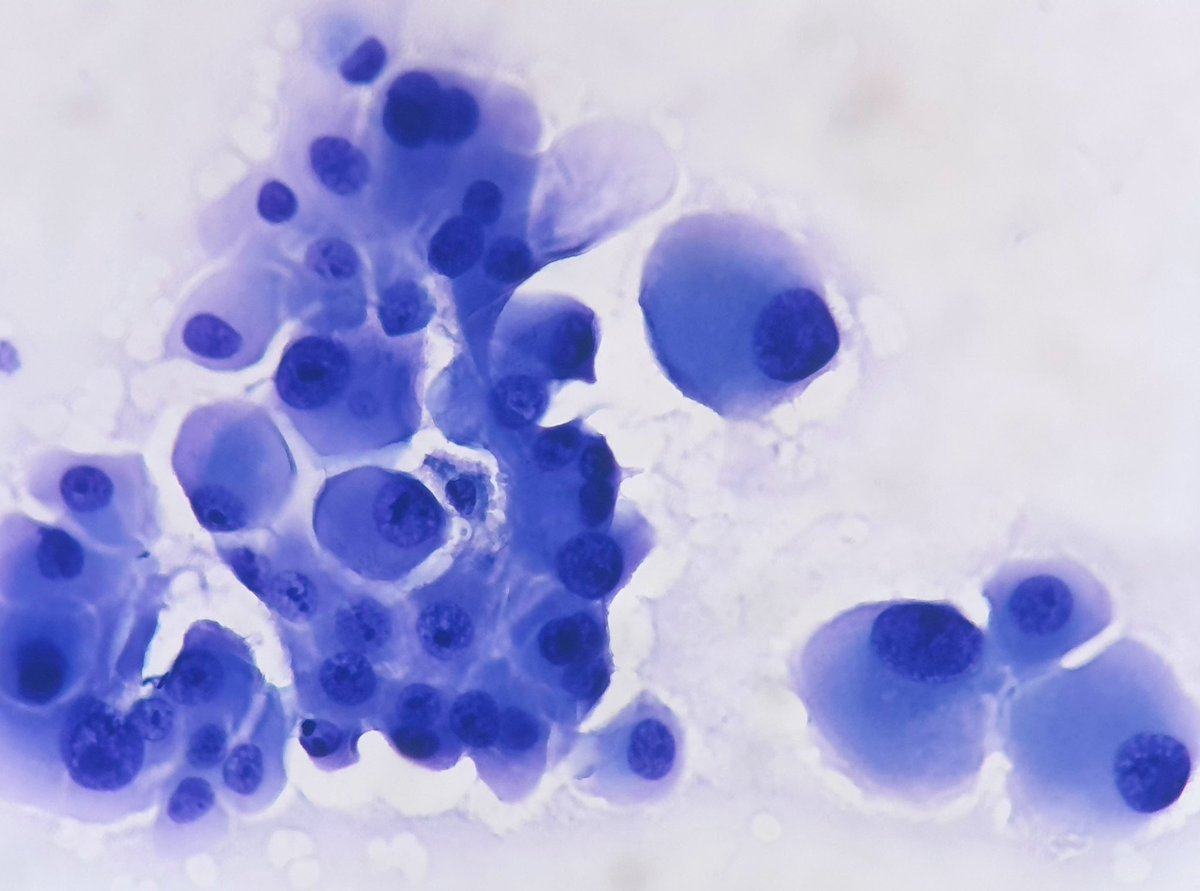
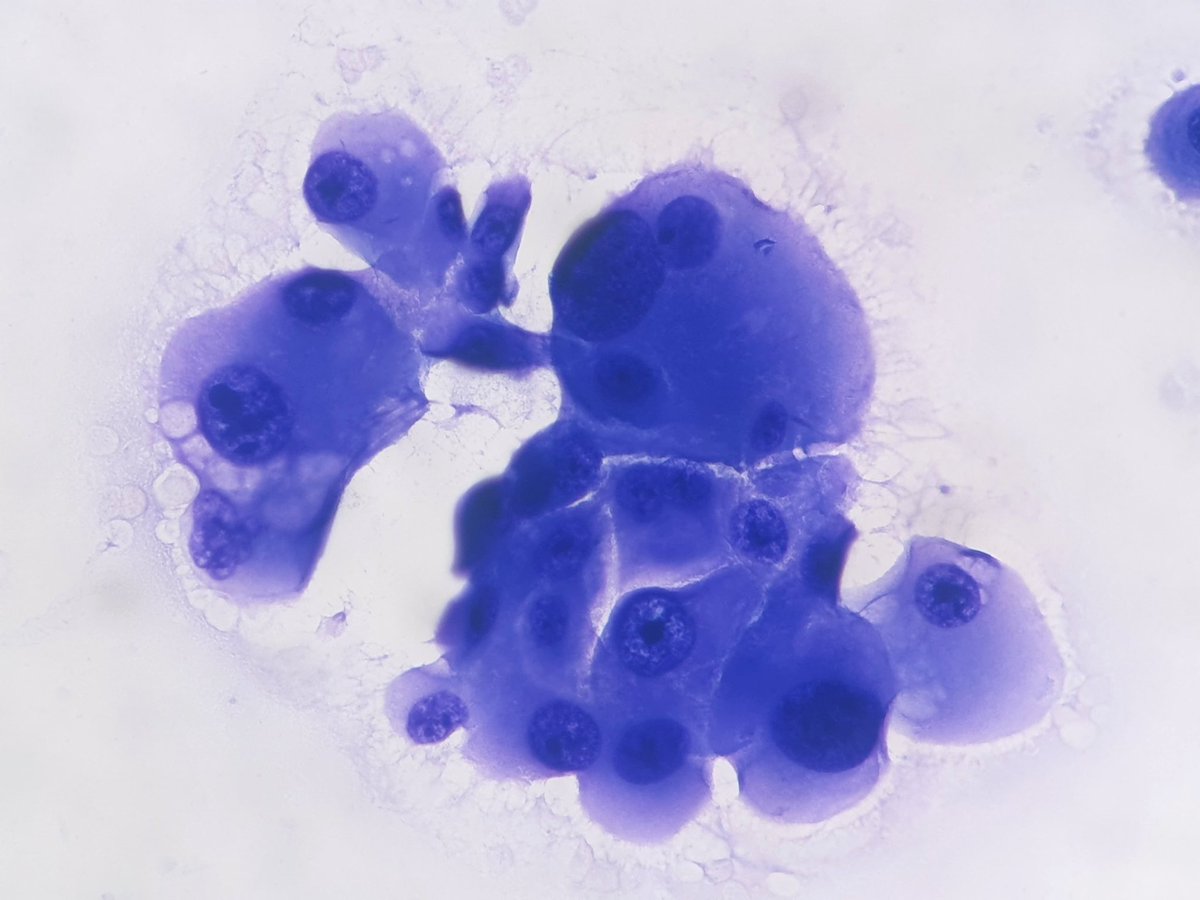
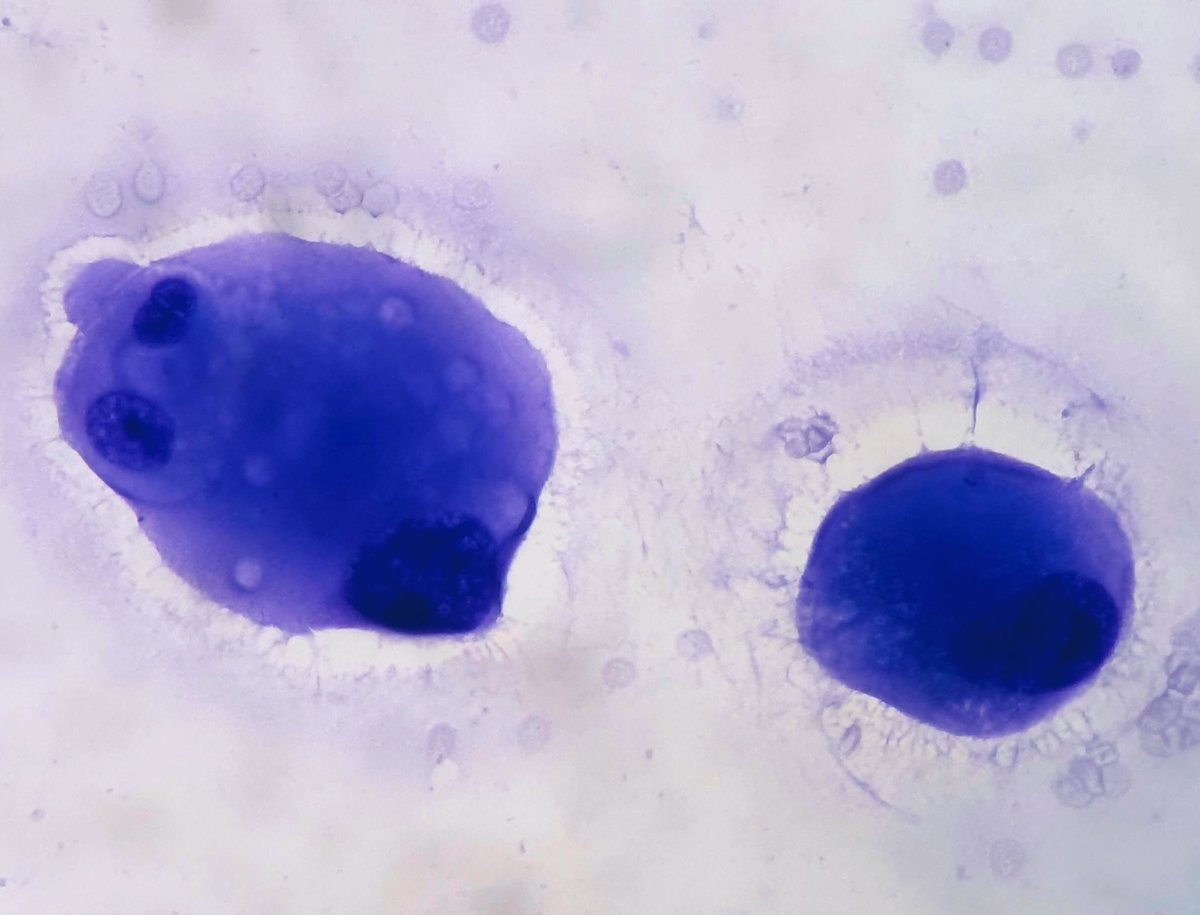
Cervical Pap w/ characteristic IUD effect
👉Glandular cells w/ vacuolated cytoplasm & w/ increased N:C (nucleoli a helpful benign feature)
👉Sometimes can see intracytoplasmic neuts so beware not to overinterpret as a glandular lesion in pts w/ IUDs
#CytoPath#PathTwitter
































![_Wondweson64's tweet photo. [Primary Biliary Cholangitis]
❶ Autoimmune, 85% 👩
❷ TRIADS: Cholestasis | Circulating Anitmitochondrial antibodies (+95%) | Nonsupurative destructive cholangitis
❸ 🩺: Fatigue, pruritis, jaundice
❹ 💊: Ursodeoxycholic acid
@Pathologists #Pathresidents #PathX #MedTwitter https://t.co/NoFk5wjWcQ](https://pbs.twimg.com/media/Gjav5YUWgAAKfbZ.jpg)