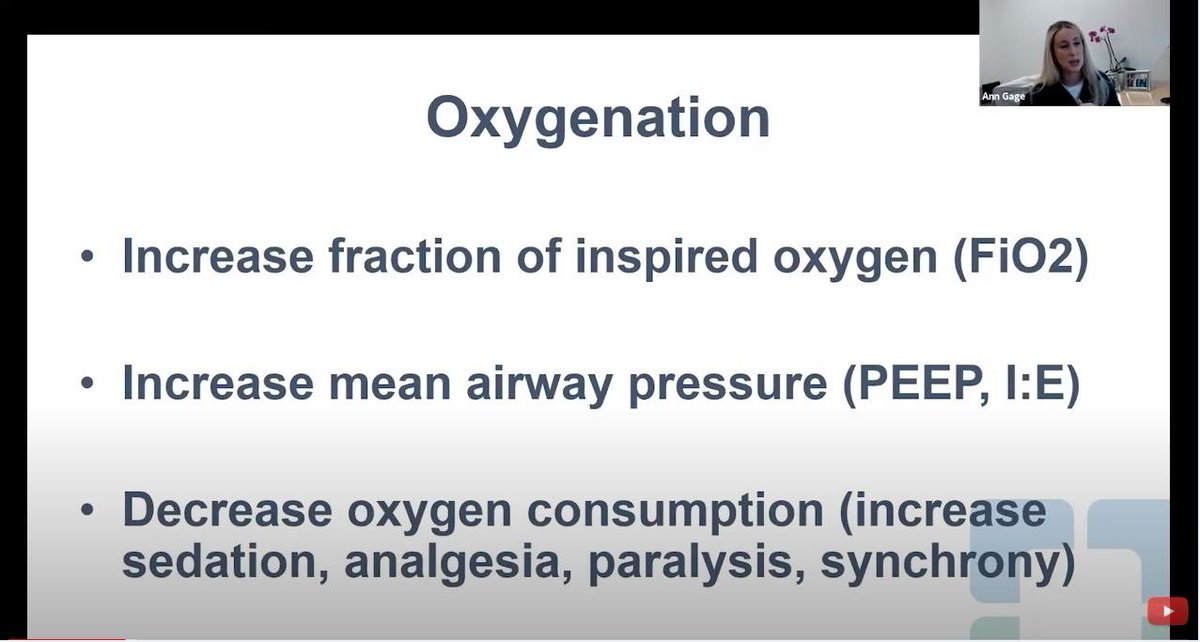
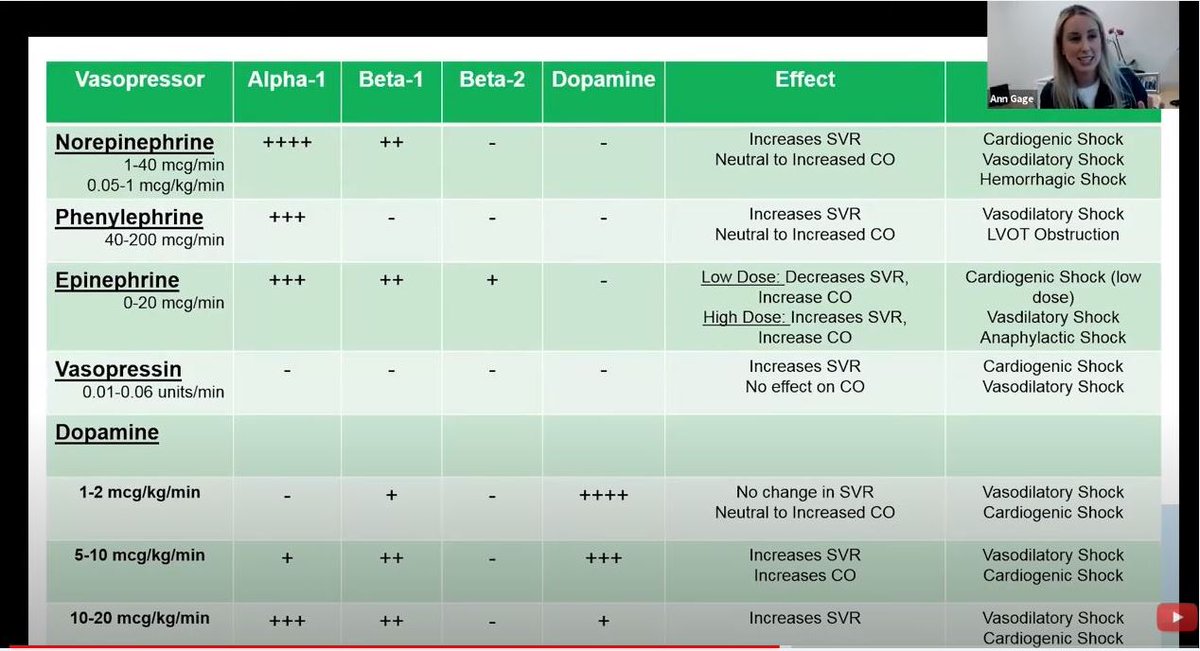
Thank you @AnnGageMD, Cleveland Clinic's interventional intensivit cardiologist, for masterful delivery of a special talk on "Reacquainting Cardiology with Critical Care: Mechanical Ventilation & Pressors"
Must watch for #ACCFIT & #Cardiotwitter 👉https://t.co/LrfovmGmge
#MedEd
Breathing New Life into an Old Skillset: Reacquainting Cardiology with Mechanical Ventilation in Response to the COVID-19 Pandemic. Thank you @JACCJournals@JGrapsa@AnkurKalraMD@RanLeeMD for helping ease some anxiety re: caring for our ICU patients. https://t.co/uA2EiCx9b1
COVID-19 Prep Update- March 14:
Last night I was on with state & local officials around the US well into the night. By March 23 many of our largest cities & hospitals are on course to be overrun with cases.
I am going to prepare a memo for them. I will share highlights here.1/
@bmorecardiology@drjohnm@jaymontgomery44 Have seen incessant bundle branch reentry post valve surgery - possibility based on typical LBBB morphology here, and rapid rate.
@JAMACardio, reassuring data regarding high amounts of physical activity/exercise and coronary calcification. Growing evidence of benign association, at least from a population standpoint. https://t.co/A8fzsS8Ee7
@bmorecardiology@keaglemd@drjohnm@johnmcph@DLBHATTMD Thompson recommends two years of high intensity statin before resumption of competition, based on plaque remodeling studies/hypothesis. ACC/AHA advise DQ for 3mo lost AMI/PCI, then OK if normal EF and stress. These are all separate from DAPT concerns.
@bmorecardiology@keaglemd@drjohnm@johnmcph@DLBHATTMD Question isn’t simply “triggering” another MI, or chronically increasing risk. But triggering fatal VT/VF via border-zone ischemia when acidotic, hypokalemic, and experiencing profound myocardial stress during critical portion of competition or training.
@bmorecardiology@keaglemd@drjohnm@johnmcph@DLBHATTMD Recommend reading papers on the topic of competitive athletics and CAD by Paul Thompson. ACC/AHA guidelines from 2015 are open access (I just pulled up on my phone in Anguilla ;).
Left Atrial Electromechanical Remodeling Following 2 Years of High-Intensity Exercise Training in Sedentary Middle-Aged Adults | Circulation #AHA2018 https://t.co/oG6VkIBgDj
New study finds pro football retirees at least 5 times more likely to have atrial fibrillation than matched nonathlete controls: https://t.co/352jGMMu6n
Another look at CRF and mortality, here in a presumed “healthy” population. Using CPX for VO2max measurement, and less stringent cutoffs for high fitness. But message remains: fitter is better. https://t.co/e951ZIY6vo
@TheEliMarcus May be benign adaptation (increased bone/Ca turnover?) - evidence that these are more stable plaques. May partly explain our/other findings that athletes live longer, lower rates of CAD events. That said, CAD is #1 cause of sudden death in athletes >35 years old.
Excited to see our work finally published! Many to thank for helping bring all this together.
Association of Cardiorespiratory Fitness and Mortality Among Adults Undergoing Exercise Treadmill Testing https://t.co/QVkht9Gf8X
ICYMI: Individuals with 'elite' cardiorespiratory fitness for their age maintained a survival advantage over high performers (75th-97.6th percentile), suggesting there's no upper limit for the benefits of #fitness. @KyleMandsager@ClevelandClinic https://t.co/skn1x9PJ7U
@TheEliMarcus Can’t comment on individual case/give med advice. Studies have shown more coronary Ca2+ in endurance athletes, others suggest these are more stable plaques. Unclear true clinical significance. We found the most fit patients lived longest. Should discuss w your MD.