There was a recent suicide of a US medical student after a professionalism violation. Many students feel they have to be perfect, that one blemish on their record will ruin their career. But if you could know the truth about your attendings, you’d know they’ve all made enormous mistakes. I’ve made hundreds over the years. Talk to someone if you’re in despair. And allow yourself to be flawed. Don’t try to be perfect. No one is.
I have deep respect for the Krebs cycle, the Golgi apparatus and the structure of tRNA but honestly these things belong more on a college biochem or cell bio test than on Step exams to determine whether to license a doctor to practice medicine in the US. I’d much rather have future physicians memorizing the five major social determinants of health or the nutrition content of common foods.
1/9
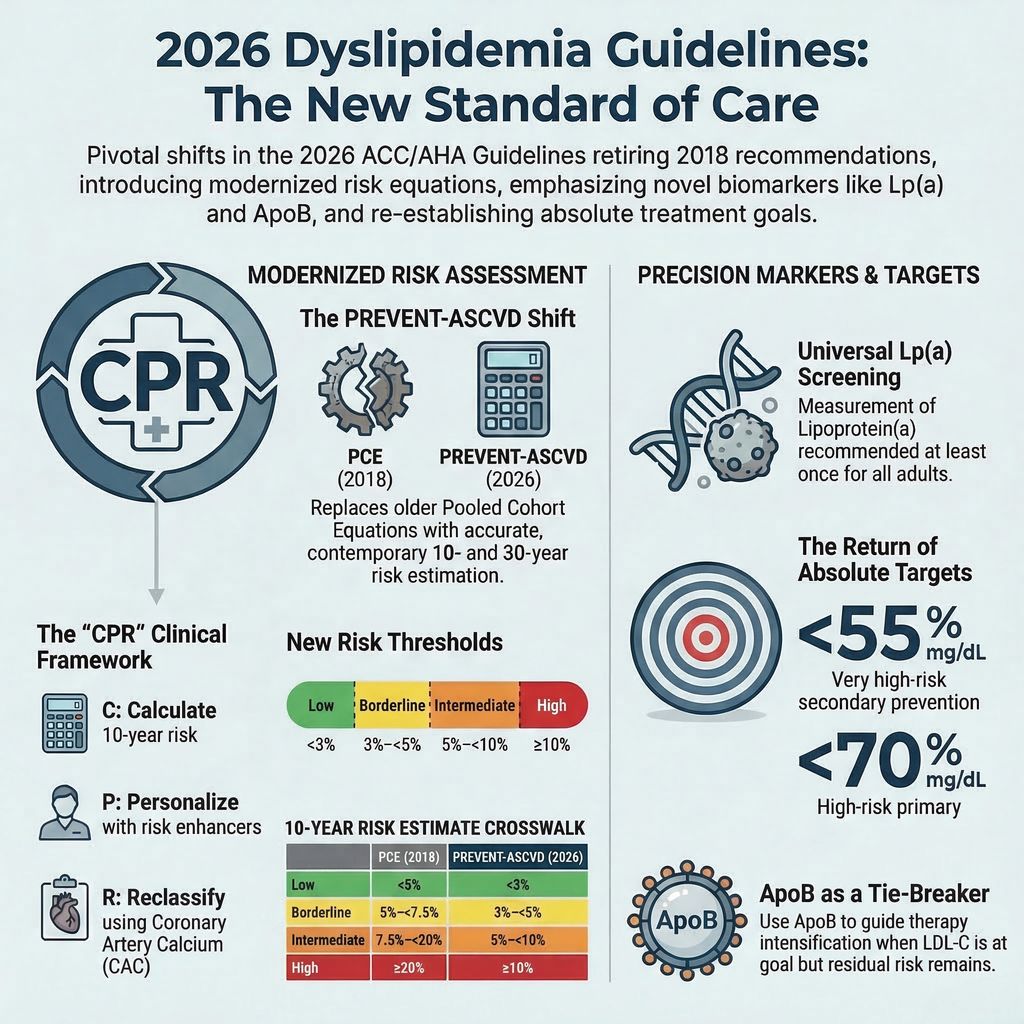
The 2026 ACC/AHA Dyslipidemia Guidelines are officially here!
Replacing the 2018 guidelines, these new updates bring major shifts in risk assessment, novel lipid markers, and cholesterol targets.
Here are the most salient features you need to know. 🧵👇
#Cardiology #MedTwitter
One of the most meaningful evolutions in the 2026 ACC/AHA dyslipidemia guideline is the continued elevation of CAC as a central tool in preventive decision-making.
We have come a long way.
1. In the 2013 guidelines, CAC was effectively sidelined.
2. By 2019, it re-emerged as a decision aid.
3. In 2026, it is now clearly embedded in the framework of risk assessment, treatment initiation, and treatment intensity.
Two messages stand out.
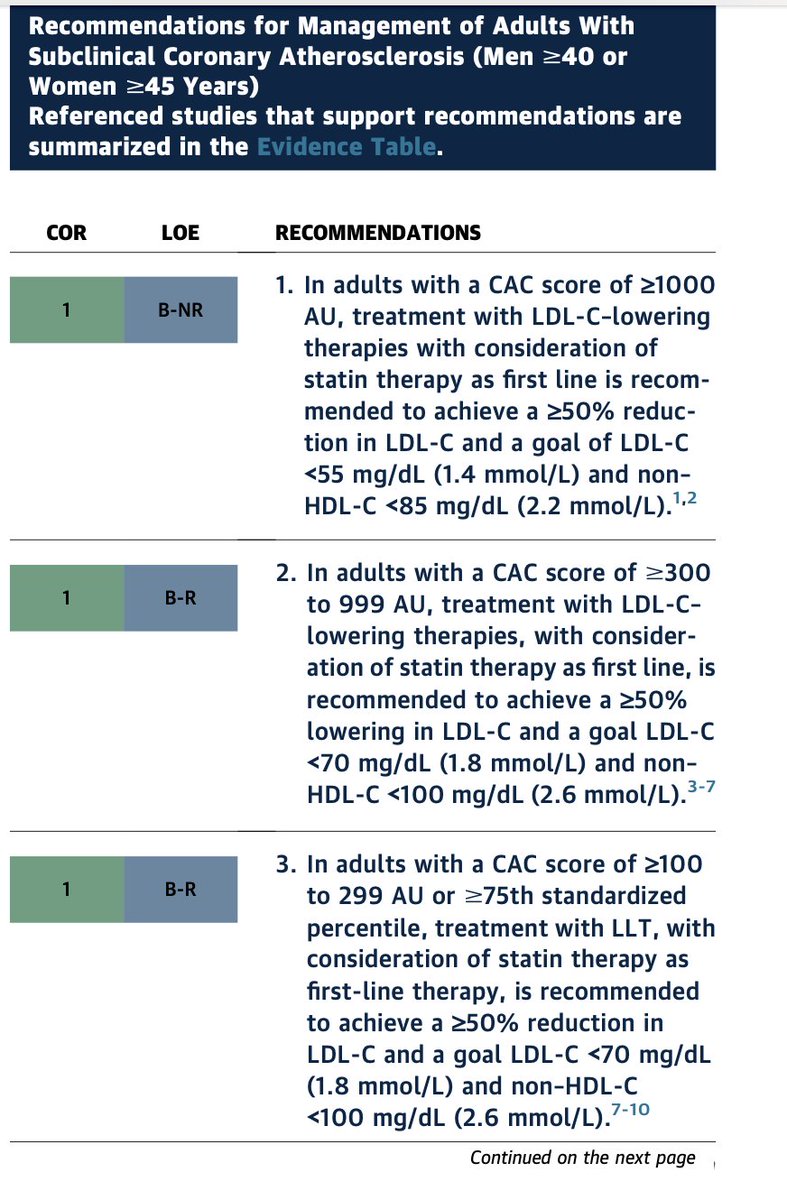
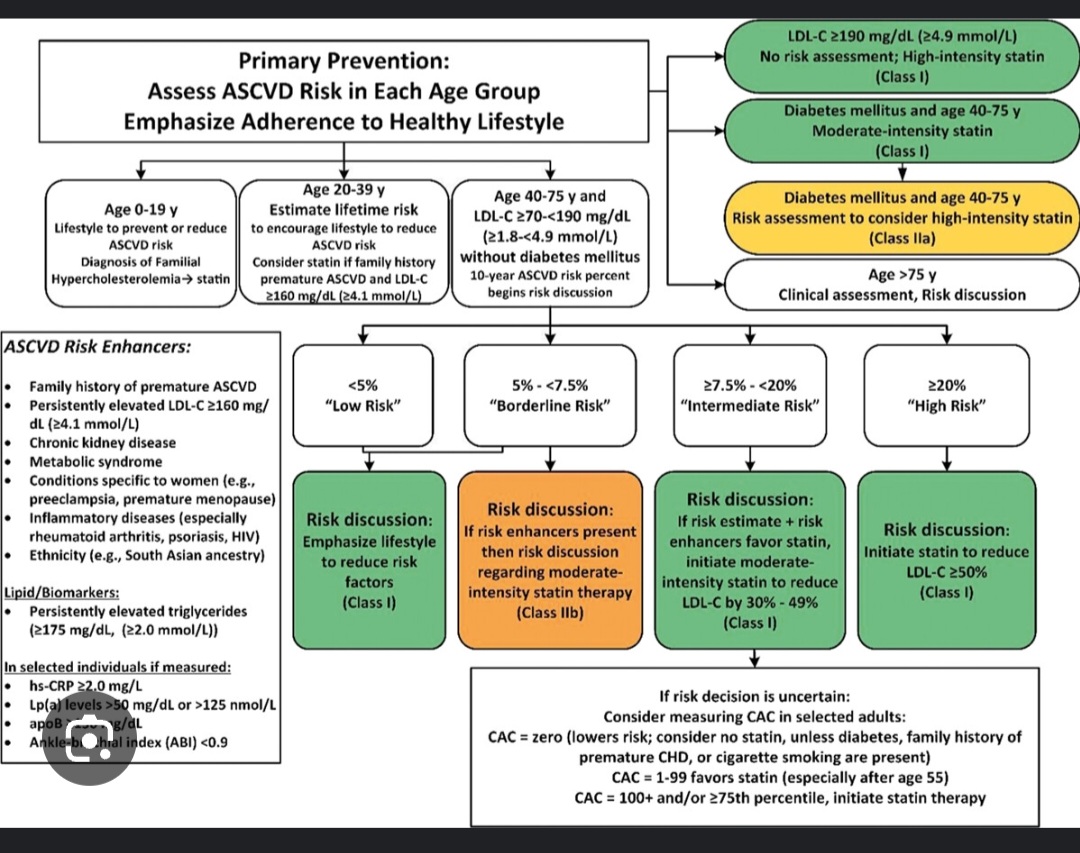
1. First, CAC has become the preferred decision aid when treatment decisions are uncertain. This is not an uncommon situation. In real-world practice, uncertainty is the rule rather than the exception, especially in borderline or intermediate-risk individuals. #PowerOfZero provides a clear distinction who is and not at risk that for the decision whether lipid-lowering therapy should be initiated.
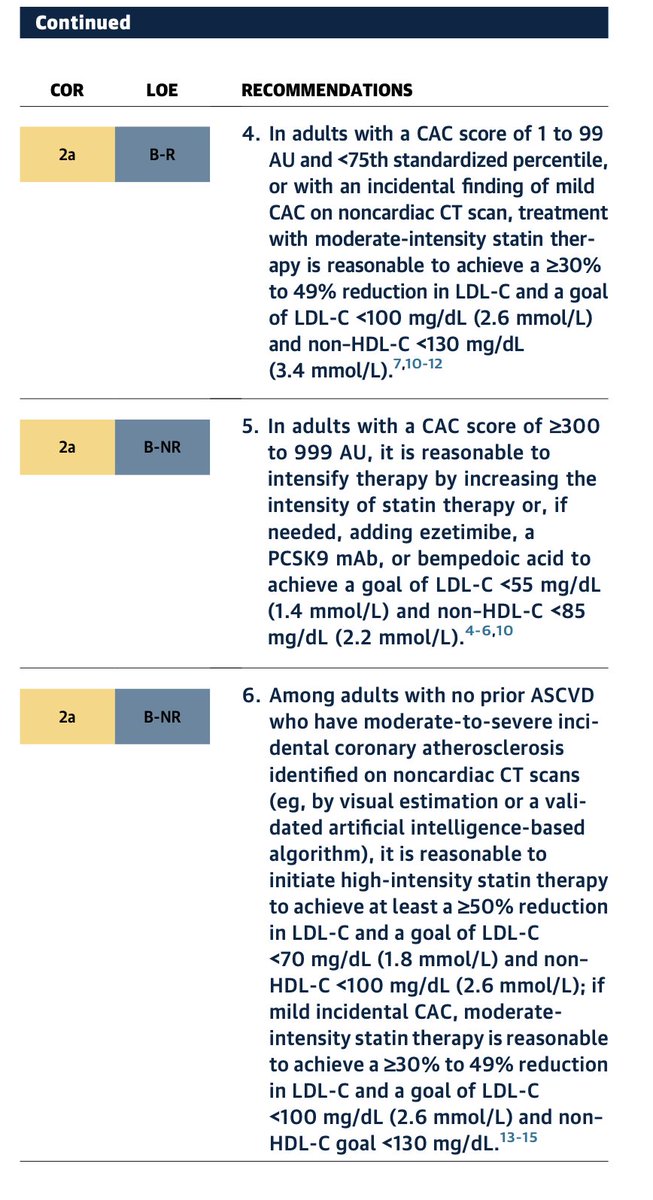
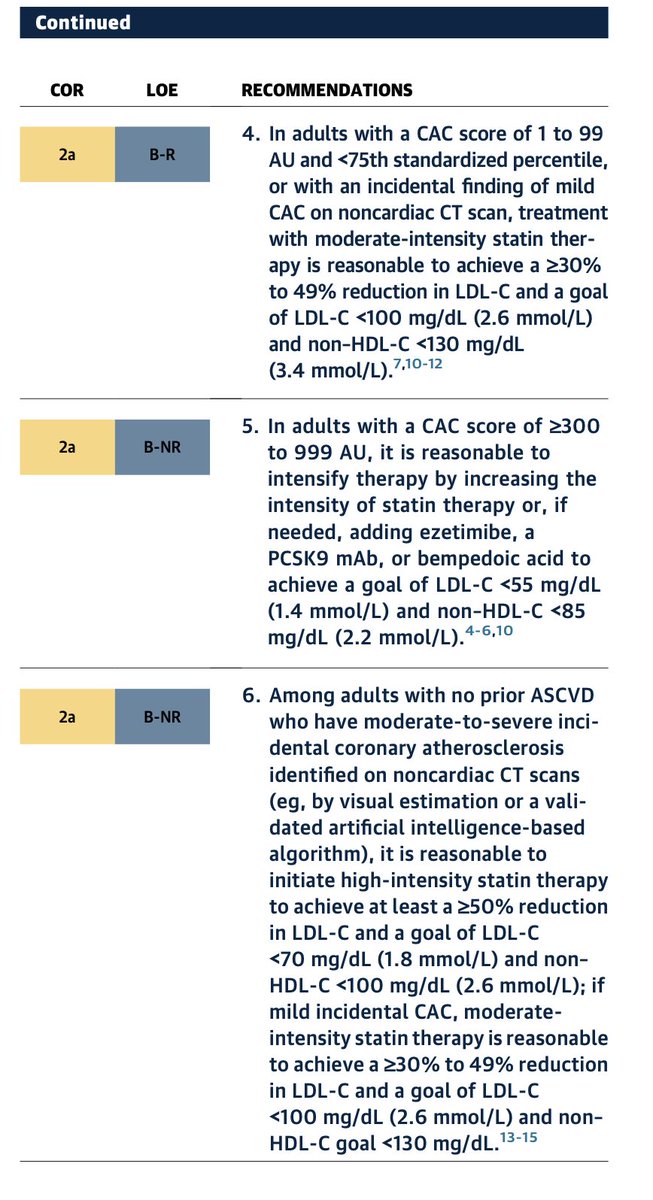
2. Second, the guideline goes beyond initiation. CAC is increasingly used to guide the intensity of therapy. Increasing plaque burden corresponds to progressively more aggressive LDL targets and therapeutic strategies. For example, individuals with CAC ≥300–1000 are recommended to pursue LDL reduction strategies approaching secondary prevention intensity, reflecting event rates comparable to treated ASCVD populations.
This is a MAJOR shift.
CAC is no longer simply a tie-breaker for statin decisions. It is evolving into a disease-guided framework for preventive intensity.
From a practical standpoint, this matters.Risk equations estimate probability. CAC visualizes disease.
1. When uncertainty exists, seeing the burden of atherosclerosis often changes the conversation for both clinician and patient.
2. It also aligns therapy more closely with biology (GREATER DISEASE, MORE INTENSE THE TREATMENT) rather than risk-factor projections alone.
IN 2026. CAC has moved from the margins of guidelines to the center of preventive cardiology.
For clinicians, that represents one of the most practical advances in translating risk assessment into actionable care.
Congrats @rblument1@RonBlankstein@DrMichaelShapir & rest of the guideline authors
@AJPCardio@ASPCardio@MichaelJBlaha@Sadeer_AlKindi@HMethodistCV
lipidology has moved far beyond statin monotherapy. The discussion highlights a central tension: we have more effective drugs than ever, yet treatment inertia remains profound, with many high-risk patients still undertreated.
💊🫀 Lipidology in 2025: from “lower LDL” to precision prevention
This expert discussion in the Journal of Clinical Lipidology (2025) offers a rare, insider view on how lipid-lowering drugs are actually conceived, developed, and translated into practice—and where the field is heading next .
🧠 A mature field facing new challenges
LDL-C remains a causal driver of ASCVD, but lipidology has moved far beyond statin monotherapy. The discussion highlights a central tension: we have more effective drugs than ever, yet treatment inertia remains profound, with many high-risk patients still undertreated.
🔬 How new lipid drugs are born
Successful development now hinges on:
Genetic validation (Mendelian randomization) to de-risk targets
Surrogate endpoints with regulatory credibility (LDL-C remains king)
Cost-effectiveness, safety, and tolerability, often more important for uptake than maximal efficacy
PCSK9 inhibitors are used as a cautionary tale: biologically sound, outcome-proven—but initially underutilized due to pricing, complexity, and unrealistic expectations.
💊 What’s coming next?
The future is multi-target:
Lp(a) therapies are poised to reshape prevention 🧬
CETP inhibition (e.g. obicetrapib) aims for “LDL-lowering plus” effects, including Lp(a) reduction and metabolic benefits
Remnant cholesterol, ApoC3, and inflammation (IL-6, NLRP3) emerge as key residual-risk targets
Imaging endpoints (non-calcified plaque volume) may help de-risk and accelerate drug development
⏳ The most important message
Prevention must start earlier and longer. Modest LDL reductions in low-risk individuals may yield greater lifetime benefit than aggressive treatment late in disease.
🔮 Bottom line
We already have the tools to prevent ASCVD. The real challenge is using them earlier, smarter, and together—moving lipidology from reactive treatment to precision cardiovascular prevention 🚀
@Vcassano11 Debate with any hardcore religious guy is pointless. He won't accept anything beyond his holy book even though it might be full of misogyny and superstitions. They'll try to justify every dumb shit in the name of God. An intellectual convo is simply not possible.
"आजको सन्दर्भमा पनि उत्तिकै प्रासंगिक आवाज. आजको पुस्ताले सुन्नै पर्ने कथा.
उज्वल थापाको जीवनयात्रामा आधारित दिमाग घोच्ने मान्छे देशभर जनवरी ९ / पौष २५ गते रिलिज हुँदैछ।
हेर्न नछुटाउनुहोला।"
#UTF#DimagGhochneManche
CAC = 0 ≠ zero risk = no free pass
i.e CAC 0 means no calcified plaque but NOT no atherosclerosis.
Higher LDL-C is linked with more non-calcified plaque and higher CHD risk despite 0 calcium. (esp in the young )
"My calcium score is zero, so my LDL doesn't matter."
I hear this constantly from the LDL skeptic crowd. Zero calcium = zero risk, they say.
Why bother lowering cholesterol if there's no plaque to see?
New data from 23,777 patients just dismantled this argument.
3 important takeaways from the study.
1. In symptomatic individuals with a CAC score of zero, 11% were found to have non-calcified plaque on CT angiography.
2. There is a strong, linear association between LDL-C levels and the presence of non-calcified plaque.
3. Elevated LDL-C was associated not just with minor plaque, but also with obstructive plaque (blockages) in patients with CAC = 0.
Here's the biology the skeptics ignore: atherosclerosis doesn't start calcified.
In young adults, the plaques we should fear most are soft, lipid-laden, and invisible to the calcium scan.
Meaning CAC=0 Does Not Mean "No Plaque"
And don't get me wrong.
I don't mean that it's a useless test. While CAC is a powerful tool, it is a "lagging indicator."
In younger patients, waiting for calcium to appear may delay necessary treatment.
Lipoprotein(a) and recurrent ASCVD: why it matters in secondary prevention
This large real-world analysis from the European Heart Journal examines the role of lipoprotein(a) [Lp(a)] in patients who already have established atherosclerotic cardiovascular disease (ASCVD). Using the US Family Heart Database, the authors analyzed 273,770 individuals with prior ASCVD and measured Lp(a) levels, with a median follow-up of 5.4 years .
Key findings
Lp(a) showed a continuous, dose-dependent association with recurrent ASCVD events. Compared with patients with Lp(a) <15 nmol/L, the adjusted risk of recurrent events increased progressively, reaching a ~45% higher risk in those with Lp(a) ≥300 nmol/L. Importantly, this relationship was consistent across sex and race/ethnicity, despite higher absolute Lp(a) levels being more common in women and Black individuals.
The increased risk applied to all major components of ASCVD recurrence, including myocardial infarction, revascularization (PCI/CABG), and ischemic stroke (with slightly lower effect sizes for stroke).
Therapeutic implications
Although no approved Lp(a)-lowering therapies currently exist, the study suggests that high-impact LDL-cholesterol–lowering therapy may partially mitigate Lp(a)-related risk, particularly at levels ≥180 nmol/L. The attenuation appeared strongest among patients treated with PCSK9 inhibitors, though this finding is observational and subject to confounding by indication.
Why this study matters
This is the largest and most racially diverse secondary-prevention cohort to date addressing Lp(a). It challenges the notion of a “risk plateau” at moderate Lp(a) levels and reinforces that Lp(a) remains a clinically relevant driver of residual risk even after an ASCVD event.
Bottom line
Lp(a) should be measured systematically in all ASCVD patients. The results highlight a major unmet need and strongly support ongoing outcome trials of dedicated Lp(a)-lowering therapies.
The natural history of patients with medically managed CCS is not as benign as we think. Our analysis of reconstructed individual patient's data from 29 trials and 53,000 pts shows AMI rates of 12.5% at 5 years and 8.6% mortality rate.
Outcomes will be much worse in non RCT real-world populations where risk factor control less optimal and multimorbidity more prevalent.
work led by @Nicholaswschew and team
➡️ https://t.co/m30sllCBz5
@SeeFisch Will the indications of PCI increase over time and prove to be better in many ways ? Especially after advanced stents /techniques. Regarding TVD and two vessels in a diabetic .
Wrt FREEDOM and excel trial.
#CABGvsPCI
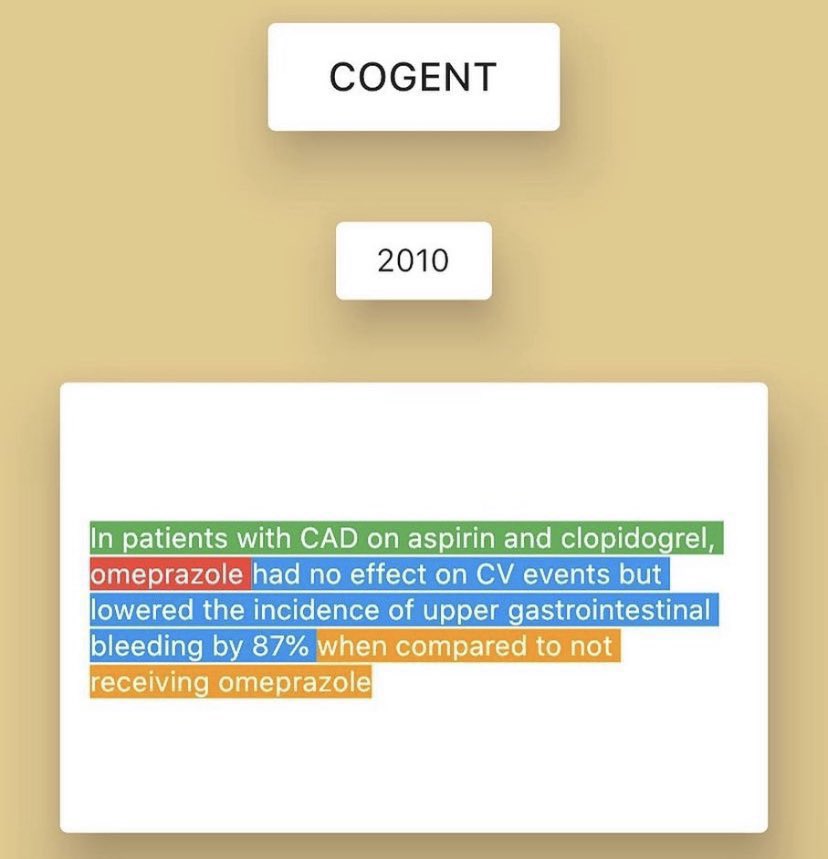
Prophylactic use of PPI among patients on dual antiplatelet therapy? Because yes we all have 🫀 , but we also have a GI tract as well. COGENT Trial, NEJM 2010 ♥️
PS: this 🔑 trial by @DLBHATTMD also showed the absence of interaction between clopidogrel and omeprazole, despite their both being metabolized by cyp2C19. As a prodrug, clopidogrel requires cyp2C19 for conversion to its active form – thought prior to be inhibited by omeprazole.




















![FCademartiri's tweet photo. Lipoprotein(a) and recurrent ASCVD: why it matters in secondary prevention
This large real-world analysis from the European Heart Journal examines the role of lipoprotein(a) [Lp(a)] in patients who already have established atherosclerotic cardiovascular disease (ASCVD). Using the US Family Heart Database, the authors analyzed 273,770 individuals with prior ASCVD and measured Lp(a) levels, with a median follow-up of 5.4 years .
Key findings
Lp(a) showed a continuous, dose-dependent association with recurrent ASCVD events. Compared with patients with Lp(a) <15 nmol/L, the adjusted risk of recurrent events increased progressively, reaching a ~45% higher risk in those with Lp(a) ≥300 nmol/L. Importantly, this relationship was consistent across sex and race/ethnicity, despite higher absolute Lp(a) levels being more common in women and Black individuals.
The increased risk applied to all major components of ASCVD recurrence, including myocardial infarction, revascularization (PCI/CABG), and ischemic stroke (with slightly lower effect sizes for stroke).
Therapeutic implications
Although no approved Lp(a)-lowering therapies currently exist, the study suggests that high-impact LDL-cholesterol–lowering therapy may partially mitigate Lp(a)-related risk, particularly at levels ≥180 nmol/L. The attenuation appeared strongest among patients treated with PCSK9 inhibitors, though this finding is observational and subject to confounding by indication.
Why this study matters
This is the largest and most racially diverse secondary-prevention cohort to date addressing Lp(a). It challenges the notion of a “risk plateau” at moderate Lp(a) levels and reinforces that Lp(a) remains a clinically relevant driver of residual risk even after an ASCVD event.
Bottom line
Lp(a) should be measured systematically in all ASCVD patients. The results highlight a major unmet need and strongly support ongoing outcome trials of dedicated Lp(a)-lowering therapies.](https://pbs.twimg.com/media/G8Oi1dZXwAQmD5H.jpg)