@megothelioma @VUMCPathology Thanks for a lovely example of a benign curiosity lesion.
Here is the rare massive version on CT imaging from a middle aged patient. The entire abdomen is myelipoma!
Now this is a cool diagnosis - myelolipoma. A thin rim of adrenal cortex lines an area of mature fat and hematopoietic elements. This case even had some osseous metaplasia. #PathTwitter#MSGPath
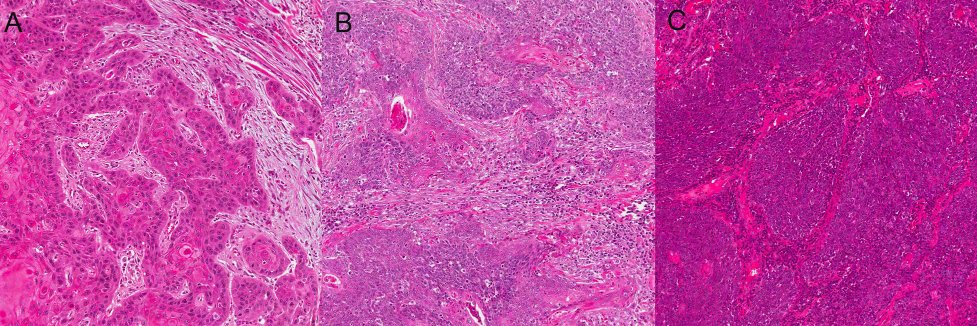
Tricky tumors when they arise in the thyroid gland because they can resemble papillary carcinoma, showing papillae, abortive nuclear irregularities like PTC, and PAX8 expression. Must look for the secretory material!
@Pathologists@bfaquin Thanks all for attention. The most important thing we can do as pathologists is to be consistent in what tests we do for pts with head and neck SCC. The guidelines are a start for this - and can shift in time as the field shifts. #capchat@Pathologists@bfaquin@LewisPath
Nuclear only or cytoplasmic staining only does not count, no matter the intensity or distribution - must be nuclear and cytoplasmic. For any equivocal p16 stains (borderline), your can do HPV-specific testing to resolve (RNA ISH best). #capchat@LewisPath@bfaquin@Pathologists
@Pathologists@bfaquin p16 should be positive in >70% of tumor cells, in both nucleii AND cytoplasm, and with at least moderate intensity in order to use as prognostic marker and surrogate if high risk HPV. #capchat@bfaquin@Pathologists@LewisPath
@Pathologists@bfaquin p16 should be positive in >70% of tumor cells, in both nucleii AND cytoplasm, and with at least moderate intensity in order to use as prognostic marker and surrogate if high risk HPV. #capchat@bfaquin@Pathologists@LewisPath