@markkaplan20 Thank you for building this. Do you have women doctors on your team? I didn’t see any on your website. If not, please consider adding women’s health experts. Women’s cardiovascular issues are different than men’s.
"Heart disease runs in my family."
Four words I heard my whole life. Four words millions of people say.
They're describing their genes without knowing it.
I ignored those words until they nearly killed me at 52.
Then I did what nobody had ever told me to do. I tested my genes.
What I found changed everything. For me and for my son David. 🧵
Why we STILL have no FDA-approved therapies for #POTS and #dysautonomia:
❓ Where did we go wrong???
Here is MY take on WHY:
🧠 Labeling it as "complex, multi-systemic, multi-factorial." All true, but in reality -- it creates ambiguity, lack of focus, broad range of phenotypes and etiologies ➡️ Mechanistically, where do you even begin to develop targeted therapies?!
🧠 Trying to add POTS to "autonomic disorders," most of which are RARE by definition -- it creates a huge shortage of physicians who specialize in autonomic disorders ➡️ You want many doctors to diagnose and treat it, not a few, to increase and diversify therapeutic options.
🧠 Excluding POTS from neurologic education: this is a major mistake because the autonomic NERVOUS system is involved ➡️ When most neurologists are not well-versed in diagnosing and treating POTS, patients lose: neurology is not only about migraine or neuropathy!
❓ How to fix this???
Here is MY take on HOW:
🧠 Refocus POTS and dysautonomia on one mechanism instead of "it's everything" ➡️ Consider "neuroimmune" angle and try existing therapies that we have for other neuroimmune conditions (neurologic Sjogren's, lupus, MS)
🧠 Make tilt table tests, QSARTs and skin biopsies accessible and affordable for every community practice/hospital/clinic ➡️ Better diagnostic capabilities and precision diagnosis
🧠 Embrace POTS/dysautonomia as part of neurology residency curriculum - not just autonomic fellowship! ➡️ All neurologists would be required to diagnose and treat POTS in the same way that all neurologists are required to be able to diagnose and treat Parkinson's, diabetic neuropathy, migraine, etc.
🧠 Fund POTS research led by researchers with diverse and multidisciplinary backgrounds ➡️ When research money is going only to the few scientists and academic centers, you lose diversity of ideas and experiences, resulting in "more of the same" research studies.
🧠 Engage with Pharma more and better! ➡️ Learn from our headache medicine colleagues and what they have achieved in partnership with Pharma. Migraine and other headaches have no biomarkers and negative MRI of the brain, but there are over 30 FDA-approved medications and devices for treatment of migraine!
@DrJesseMorse This is extremely helpful, I appreciate your sharing your expertise and breaking this down for us. How soon can we expect these treatments to be incorporated by main stream medicine and insurance? And in the meantime, what is a reasonable cost for them?
@DrJesseMorse Are there options for people who don’t have professional athlete level funds to get these treatments? I asked my orthopedic doctor about PRP and they offer it for just over $1K per injection and I’m told it usually takes more than 1. Insurance won’t cover it, of course.
🧠 Love that list by Dr. @adamcifu. Here is my "Please do not do that research" list related to #Dysautonomia: 🗒️
1. Please no studies on exercise and rehab programs in patients with #POTS, #MECFS or #LongCOVID. We get it... exercise is good for you and helps a good subset of patients, but self-selection and other biases in these studies preclude sweeping generalizations. Some patients cannot exercise, period.
2. Please no studies on psychological correlates, personality traits, anxiety, depression or childhood trauma in patients with #Dysautonomia, #MECFS and #LongCOVID. If you don't have at least one control group consisting of patients with MS or lupus, then your findings are useless.
3. Don't waste your time to study psychotherapy in patients with #POTS, #MECFS and #LongCOVID. It'll only work on patients with significant anxiety, poor coping mechanisms and inadequate social support. It won't work for the underlying pathophysiology of these disorders.
4. We get it: salt and compression are good for you if you have #Dysautonomia so we can stop doing these studies, except one.... is long-term increased salt intake associated with a higher risk of autoimmune disorders in patients with #Dysautonomia? We don't have this study and need one to estimate the risk in a population already prone to autoimmune disorders.
5. I really could care less if breathwork, meditation, music therapy or acupuncture are beneficial in patients with #POTS, #MECFS or #LongCOVID. Those things are beneficial for many stressed and overworked individuals, regardless of health or disease. Waste of time and money....
6. Demographics, phenotypes, loss of smell and taste and other such things that have been studied ad nauseam in #LongCOVID do not need to be repeated in any cohorts from any country. Enough is enough.
7. As an editor and reviewer of many studies on POTS, some comparisons among groups are unnecessary and useless: I don't want to see outcome comparisons between POTS and VVS vs. POTS alone or POTS and EDS vs. POTS alone groups. The more disorders one has, the worse. We know!
8. No offense to my basic science colleagues: love and appreciate your work, but honestly, if you find that muscle sympathetic nerve activity in patients with POTS is higher than in healthy controls, thank you, but it helps nothing and no one.
9. Subjective vs. objective mismatch in patients with POTS/dysautonomia or Long COVID: don't want to hear about it. The autonomic function tests were not designed to assess patients with common autonomic disorders so yes, they will look amazing on the autonomic function tests, scoring 0-1 on CASS score, but they will be very sick and debilitated regardless, and no, it's not because they have anxiety, depression or deconditioning.
10. Finally... when you talk about VO2max as a marker of deconditioning, you're talking about research from decades ago. Reduced VO2max is not caused only by deconditioning: in our patients, it's most likely from mitochondrial and endothelial dysfunction, decreased organ perfusion and cellular metabolism problems.
Thank you for reading my list! Please do sensible, logical and clinically relevant research! 👩🔬🔬🧬
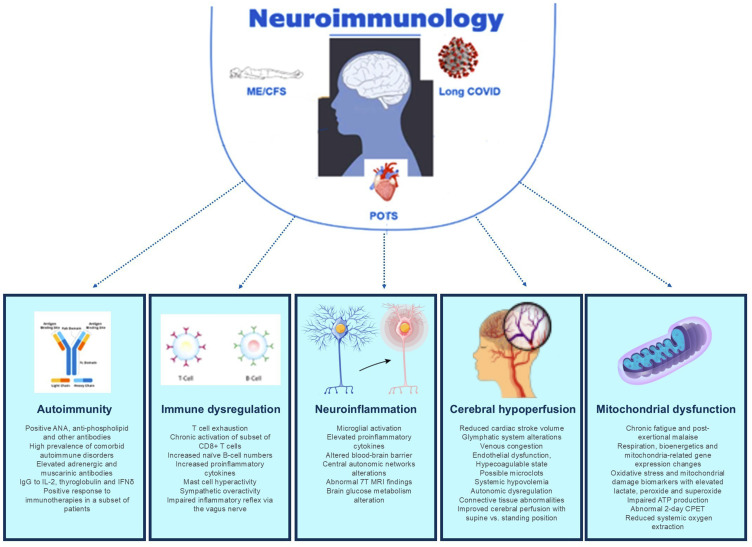
🚨 Hot off the press: my new paper that moves this field forward 🚀 and changes the narrative on what #POTS, #MECFS and #LongCOVID are... Neuroimmune Disorders!
🧠 The brain and the autonomic nervous system are involved in the immune system regulation.
🧠 There is evidence of autoimmunity, immune dysregulation, cerebral hypoperfusion, neuroinflammation and other mechanisms in all three disorders.
🧠 #Neuroimmunology is a field that should embrace these disorders: #MultipleSclerosis, the staple of neuroimmunology, used to be called hysterical paralysis before CT and MRI were invented. We're at the same crossroads with these disorders.
❌ These disorders are not "mysterious", "anxiety", "deconditioning," "functional neurologic" etc. etc.
‼️ Classifying these disorders as neuroimmune and including them as part of neuroimmunology training is critical.
🛌 #PatientCare and lives of millions of people living with these disabling conditions are at stake!
Thanks to my esteemed colleagues and co-authors, Dr. @TaylorDoherty8, immunologist from UC San Diego and Dr. Lawrence Steinman, neuroimmunologist from @StanfordMed, for their support!
Read open-access paper here: 👇
https://t.co/wr7kMNKj3c
@NeurologistMom Thank you for this. I have two chronically ill daughters and relate deeply. I have followed you for a long time, you are an inspiration for me! I think of you and your daughter often and send prayers and positive thoughts for her recovery.