Culture-negative peritonitis? Don’t forget the spleen. 🩸
Case report & literature review by Raphaël Harrisson (2025).
🔗 Read here: https://t.co/ki6wWsM9C3
#PD#MedTwitter#HomeDialysis#Nephrology
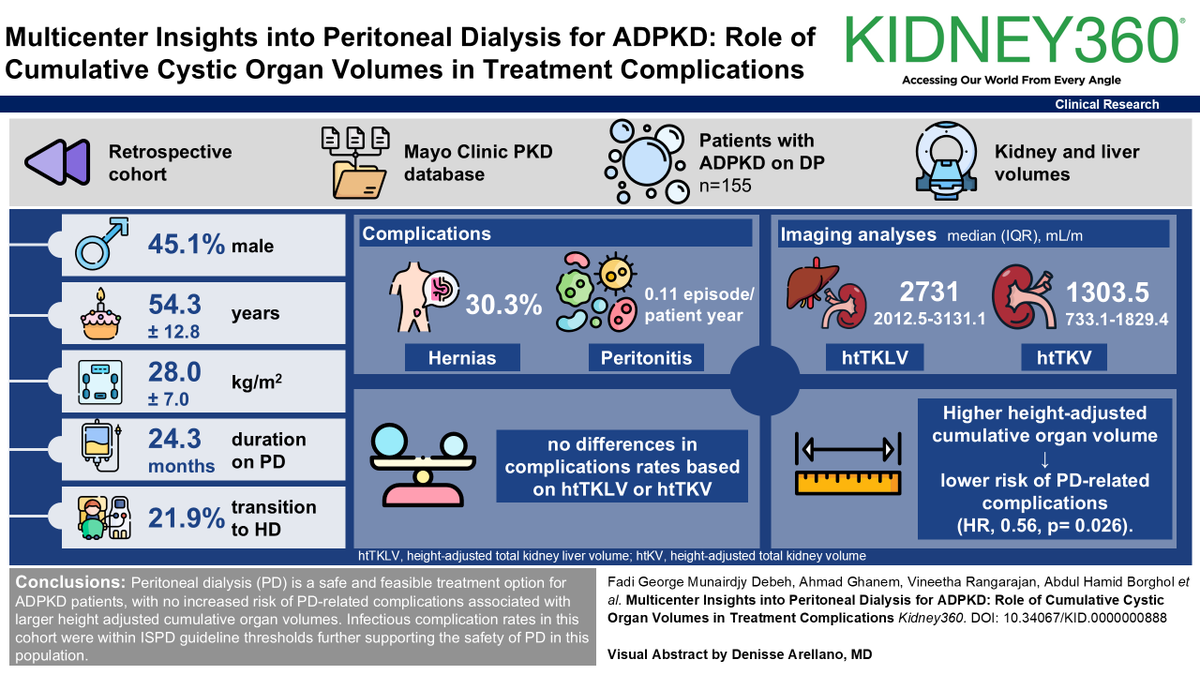
Peritoneal dialysis (PD) is not often used for patients with Autosomal dominant polycystic kidney disease (ADPKD). This #ASNKidney360 research demonstrates that PD is safe and effective for patients with ADPKD. Read more: https://t.co/g0lcCMKdEQ
▶️ APRIL is a key factor in pathogenesis of IgAN
▶️ Sibeprenlimab inhibits APRIL
▶️ Phase 2 trial of
Sibeprenlimab reduced proteinuria
▶️ Visionary trial is a large, international, RCT
▶️Primary endpoint: proteinuria
▶️ First 320 patients will be reported today ( proteinuria only)
💥💥💥 51.2% reduction in proteinuria at 40 weeks!
💥 💥💥Less SEs in the treatment group!
#ERA25
- Sarah Gleeson
Nursing care is the cornerstone of every successful peritoneal dialysis program—where expertise, compassion, and consistency truly make the difference. @Armelle_ISPD@ISPD1
@ISPDCongress@ISPD1 Learning alternative PD catheter insertion techniques from experts all around the world. Thanks to Dr Corbett for sharing his insight on troubleshooting during the procedure!
#ISPD PD as first line for AKI debate: @annieclairenf, Maher award recipient, clearly demonstrated that it is not ready for prime time in develop countries yet as more high quality data is required #ISPD24#ISPDCongress
The effect of implementing a dialysis start unit on modality decision among patients with unplanned start kidney replacement therapy
@ChrisChanUHN@JoanneBargman@PD_Perls@charmaine_lok
https://t.co/t63XgqN0to
Home hemodialysis is linked to several clinical advantages. However, it is perceived as a complex medical procedure that requires extensive training. This study demonstrates the feasibility of administering OSCEs during home HD training https://t.co/T86xFbwKgj
@ChrisChanUHN
@mustachemedical@askrenal I would add that in a clinical setting, urine Cl probably adds very little unless you’re dealing with metabolic alkalosis or need to calculate an urine anion gap for a RTA diagnosis.
@mustachemedical@askrenal It is rather complicated physiology but you’re right that the bulk of Cl is reabsorbed along with Na in the proximal tubule and then through NKCC2 (more Cl > Na). Distal Cl handling is more complex than just following Na, it depends on factors such as K and acid-base status.
@mustachemedical@askrenal You can also get high urine Na in metabolic alkalosis with volume contraction since the acid-base balance will see bicarbonate excreted as NaHCO3.
@mustachemedical@askrenal Mineralocorticoid excess states will be associated with relative hypervolemia, which will lower the stimulus to reabsorb Cl by type B intercalated cells in exchange for bicarbonate secretion through pendrin even though there is a high Cl delivery to the distal nephron.