Linda Liau fanatic, engaged Biotech Investor, GLove spreader, Big Time Cheerleader. I am not an investment advisor or attorney my opinions are just that
@PK_Fund 1 CHM recommendation isnt approval, that would come a few to several weeks after the vote if it was needed which isnt certain $NWBO
2 Industry has long held a need to w/hold public notification until a reasonable opportunity to also alert the HCP community
3 RAs work time w/them
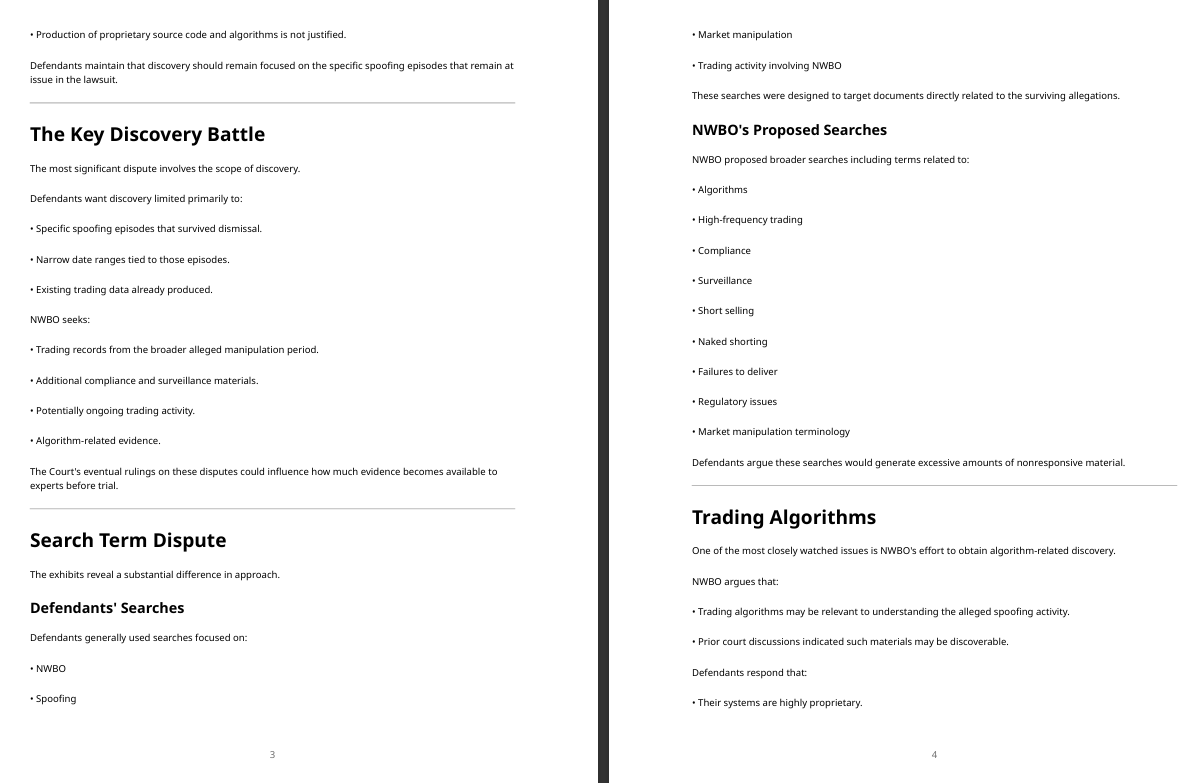
✅️Algorithms Discoverable?
The federal magistrate judge in $NWBO's spoofing lawsuit against six of the largest market makers in the world, including Citadel and Vitru, believes that the Defendant market makers' trading algorithms are discoverable
The Magistrate Judge stated, in relevant part:
"I'm not sure how that gets limited, frankly." [1]
See attached Image.
[1] Docket #286, https://t.co/2vLwDOXAki
@hoffmann6383@Cleves_trades We have a front row seat to THE GREATEST ROPE-A-DOPE BATTLE SINCE MUHAMMAD ALI vs FRAZIER, present military actions excluded $NWBO
Linda Powers is the Ali in this fight in case you re wondering and her 7 rounds of body blows are just about over
Linda Bomaye! Linda Bomaye!
@hoffmann6383@Cleves_trades The answer is pretty clear right upfront in the response as well. “We respectfully, request clarification that Mr. Mitts need not log PRIVILEGED DOCUMENTS that are technically
responsive to the subpoena but are UNRELATED TO THIS ACTION.” $NWBO
This clearly states other action
@David_J_Bier@BaddCompani 668000 people who spent nearly all of their income created a large economy. Look at what the population Grand Rapids, MI produces. Those dollars are no longer spent on rent, at grocery stores, on clothing, on mobile phones
That is the true Trickle Economy. It has always been UP
@SouthernDrive21@TimThomas0007@neilmck37597308@Investors_Hub Some over to C for storage before heading back to A1. Long term stability at C must also be guaranteed before putting back into A1’s body or severe safety issues may arrive secondary to errors
Problems with solutions
https://t.co/cPnFDvjJl0
@SouthernDrive21@TimThomas0007@neilmck37597308@Investors_Hub Look up Graft vs Host disease for explanation $NWBO has been solving for this for years. That is what Max’s ASCO presentations were about Quality Assurance. It is also what lymphopherisis clinics solve for. Quality from point A1 to B back to A1
Open your eyes to see the truth
Andrew Left Found Guilty of Securities Fraud
“Andrew Left, one of the world’s most prominent short sellers, was found guilty of securities fraud by a federal jury after a landmark trial that scrutinized his use of social media to move the price of stocks.
The verdict was handed down Monday in Los Angeles following a three-week trial and two full days of jury deliberations. Left was accused of using explosive tweets about dozens of companies to illegally influence their shares and make a quick profit.
Prosecutors said he earned about $20 million from such trades from 2018 to 2023….”
@SouthernDrive21 Well ya see, its like this ya see, yea
We got these blueprints & plans, ya see, yea
They’re secret & for our eyes only yea?
It shows how we’re gonna protect you ya see
You need protection from market preditors see
So its our proprietary business, ya see
Its none of yours $NWBO
@DrBala24943950 Sadly all I can confirm that Bright Boy passed yesterday morning. I have texted with Rosie and the family put up an informal obituary
He was a trrrific guy and this a loss for us all.
@DrBala24943950 Sadly all I can confirm that Bright Boy passed yesterday morning. I have texted with Rosie and the family put up an informal obituary
He was a trrrific guy and this a loss for us all.
$nwbo @alphavestcap
https://t.co/ydtylEtrSh
DCVax-L's MHRA Timeline: What the Evidence Shows Is Gating It, and What Is Not
Two explanations circulate for why DCVax-L's MHRA marketing authorization has not yet landed: that MimiVax's SURVIVE trial is secretly coordinating with or feeding the application, or that the review is waiting on the MHRA's external-control guidance to be finalized. The evidence rejects both. What governs the timeline is ordinary and substantive: a trial whose evidentiary framework was restructured after its original design, an external-control comparison built from reconstructed data, a population defined under a now-superseded tumor classification, first-in-class manufacturing qualification, and routine review mechanics. A recent validation of external-control methodology in glioblastoma strengthens the case that the method itself is sound, while leaving the trial-specific scrutiny intact. Every claim below is anchored to a primary or verified source. The pivotal trial figures have been checked against the full text of the primary article, not a summary of it.
The External-Control Guidance Is Not the Gate
1. DCVax-L did not use a real-world-data external control. The pivotal analysis compared treated patients against external control patients drawn from the control arms of prior randomized trials, reconstructed as individual patient data: 1,366 controls from five comparator trials for the newly diagnosed comparison and 640 from ten comparator trials for the recurrent comparison [8]. These are prior-trial controls, not registry or electronic-health-record data.
2. The MHRA guideline addresses real-world-data external controls specifically, drafted with the Commission on Human Medicines real-world-data ad hoc group [2][4]. For controls drawn from previously completed trials it states that only general principles apply, and it does not cover synthetic or virtual control arms at all [3][5]. DCVax-L's reconstructed prior-trial controls fall, at most, under general principles.
3. It is prospective design guidance, not an approval precondition. It is written for sponsors planning future trials and directs them to engage the MHRA on specific proposals [2][3]. Applications are assessed on their own merits, not held pending a guideline.
4. The timeline runs backwards for this theory. The MAA was submitted on 20 December 2023 and entered the 150-day pathway then [6]. The consultation did not open until 20 May 2025, seventeen months later, and it has since closed, with the MHRA now analysing feedback [2]. A multi-year review cannot be gated by a six-week consultation that opened in its second year.
5. A 2025 guideline cannot retroactively bind a trial designed over a decade earlier [9]. A regulator assesses a completed dataset against the standards applicable when it was designed and submitted, informed by current judgment.
6. MHRA's posture on external controls is permissive, framing real-world-data ECAs as a way to accelerate decisions where randomization is not feasible [2]. The belief that unfinalized guidance is the gate rests on a category error: it conflates prospective methodology guidance for future trials with the assessment of a specific submitted application whose controls were reconstructed prior-trial arms.
The Actual Gating Items Are Documented, Mundane, and Substantive
7. The company named the procedural gating items at submission: intensive responses to requests for further information, plus inspections of the CROs, the sponsor, the Trial Master File, regulator-selected sites among the 94 that participated, and the GMP facility [6]. The 150-day pathway is a working-day clock that stops whenever the sponsor is answering questions, so two-plus years of calendar time reflects repeated clock-stops, which is ordinary for a first-in-class submission [6][22].
8. Manufacturing qualification is a documented, multi-year, MHRA-engaged workstream. The MHRA granted NWBO and Advent a Manufacturing and Importation Authorisation for commercial cell-therapy manufacturing at Sawston in March 2023, among the first such UK licenses [7], and the 2025 to 2026 buildout scales that base through the Advent acquisition, a Grade C suite, and a dedicated leukapheresis clinic [22].
9. The trial's evidentiary framework was substantially restructured after its original design, which is itself a primary reason the review is rigorous and slow. The trial's own published report describes it as originally a randomized, double-blind, 2:1 study of DCVax-L versus placebo, with progression-free survival the primary endpoint in the 2007 protocol and a crossover design [8][9]. While the study was underway, pseudo-progression made PFS infeasible to adjudicate, so the analysis plan refocused on overall survival; the crossover then depleted the placebo arm, which necessitated comparison against external control populations, and a recurrent-GBM secondary endpoint was assessed [8][10]. Measured PFS in fact numerically favored placebo and was not significant [8]. A regulator assessing a trial that changed its primary endpoint and adopted reconstructed external controls after the design was set applies heightened scrutiny by design. That scrutiny is a legitimate, substantive gating item.
10. The WHO 2021 reclassification is a concrete population-definition issue the MHRA must address.The 2021 classification restricts glioblastoma to IDH-wildtype tumors and moves IDH-mutant grade 4 tumors into a separate, better-prognosis category [15]. The trial enrolled WHO grade 4 patients from 2007 to 2015 with central histological confirmation, and it did determine IDH R132 mutation status centrally for its treated patients, but it neither reported the resulting IDH distribution nor restricted the population to IDH-wildtype, and the reconstructed external controls predate routine IDH testing entirely [8]. Mapping the comparison onto the modern definition is therefore a real assessment task: the treated arm holds IDH data that was never reported, and the control populations lack it altogether.
11. Label scope and NICE timing have ordinary explanations. The MAA seeks both newly diagnosed and recurrent GBM [6], widening the label discussion. The NICE appraisal (ID836) is scoped to newly diagnosed disease only, requires a finalized SmPC before the dossier is appraised, and remains in progress with publication date to be confirmed [1][23].
12. External-control evidence faces extraordinary scrutiny across the whole system. A 2025 British Journal of Cancer review of 175 oncology external-control-arm submissions to HTA agencies in four countries from 2021 to 2023 found that none were accepted without restrictions and only 17% escaped outright rejection, with England the most permissive at 41% (accepted with restrictions), France at 14%, and Germany and Norway rejecting all [16]. This bears most directly on the NICE stage, but it demonstrates that ECA-based evidence is slow and contested everywhere, the opposite of a process gated by a phantom variable.
The Framework Was Restructured Once, Which Forecloses a Second Graft
13. The submitted external-control framework is the locked basis of this review. Its matching, covariate selection, alpha-spending, and pre-specified sensitivity analyses define the application the MHRA is assessing [8]. The trial's analysis was already restructured once, before database lock and unblinding. Grafting in a second, outside dataset now, from a competitor's blinded trial, would not be another permissible amendment; it would invalidate the submitted framework and force a fresh cycle.
14. Distinguish a formal SAP amendment from routine supplementary analysis. Formally amending the locked SAP would be destructive, but the MHRA can and routinely does request supplementary contextual analyses using contemporary published data as part of the review. That is already captured by the requests-for-information in point 7, and it is the realistic version of “contemporary data matters,” not evidence of a hidden control-arm transfer.
15. The controls were reconstructed by an accepted method, with a known limitation. The external control populations were selected by an independent firm, the York Health Economics Consortium, from the control groups of contemporaneous randomized trials and matched on fourteen criteria prespecified in the Statistical Analysis Plan [8]. Individual patient data for those controls were not available, as is common, so their survival curves were reconstructed from the published Kaplan-Meier plots by digitization, and a matching-adjusted indirect comparison was applied to adjust for residual imbalances [8][11]. Curve reconstruction is an established technique with validated low bias [11], not an invented shortcut, but it carries more uncertainty than true patient-level data, which is one more reason the assessment is careful. As internal support for the method, the investigators re-derived each of the fifteen comparator trials' original results after substituting their reconstructed controls and reproduced whether each trial's primary endpoint had been met [8].
The External-Control Method Now Has Empirical Validation in Glioblastoma
16. A May 2026 reanalysis tested the method against randomized data and it held. The INSIGhT investigators re-analyzed the three experimental arms of their randomized platform trial by replacing the internal control arm with matched external control data, and after propensity-score matching found no survival benefit for abemaciclib (HR 1.00; 95% CI 0.75 to 1.34), neratinib (HR 0.93; 0.70 to 1.24), or CC-115 (HR 0.88; 0.41 to 1.88), estimates similar to the original randomized analyses [12]. The three arms had shown no overall-survival benefit against the internal randomized control [13], and the external-control method reproduced that null rather than manufacturing a spurious positive. This is evidence the method does not systematically invent signal in this disease, and the investigators note its validity depends on comprehensive data capturing all relevant confounders [12].
17. What this does and does not establish. It validates external-control methodology in newly diagnosed glioblastoma generally. It does so using propensity-score matching on patient-level external data, a related but not identical technique to DCVax-L's reconstruction of control data from published survival curves with matching-adjusted indirect comparison, so the support runs to the family of external-control methods rather than to DCVax-L's exact implementation. It does not, by itself, validate DCVax-L's specific result, and it does not remove the trial-specific scrutiny in Section 3, namely the post-hoc restructuring, the reconstructed controls, and the pre-2021 population. The honest reading is that the method DCVax-L used is now better supported than it was when the 2023 critiques were written, while the implementation-specific questions remain part of the assessment. Claims that this “validates DCVax-L” or that the trial “satisfies every regulatory criterion” are interpretations a sponsor would make, not settled facts, and a regulator could read them differently.
SURVIVE Cannot Be Feeding DCVax-L
18. SURVIVE is a randomized, placebo-controlled trial, not a free-standing control set, randomizing roughly 228 to 247 newly diagnosed patients 1:1 with overall survival as the primary endpoint [17]. Its data are blinded and barred from disclosure while the study is ongoing [18], and MimiVax stated it was only beginning the final analysis in May 2026 [19]. Data only now entering analysis cannot have informed a DCVax-L review running since December 2023. The interim that occurred was a futility analysis the trial passed, a continuation decision, not a release of comparative results [18].
Coordination Would Leave a Trail, and the Incentives Run the Wrong Way
19. A formal patient-level data transfer would be visible. NWBO is a public, SEC-reporting company, so a material data or licensing agreement would trigger disclosure; MimiVax is privately held [20], but a transfer would still surface through NWBO's filings, the MHRA inspections and correspondence, and trial-site IRB amendments. As a likelihood ratio, the probability of seeing no trace across all of those channels if a transfer had occurred is very low, while the probability of seeing none if no transfer occurred is essentially one, so the silence weighs heavily toward no transfer.
20. The honest limit, linked to proximity. Absence of a trail rules out a formal data transfer; it does not rule out informal awareness of timelines or general trends through the shared Roswell Park nexus. That informal awareness falls far short of the thesis and would not gate an authorization, but it is the boundary the argument actually establishes.
21. The incentives are backwards. MimiVax and NWBO target the same newly diagnosed GBM indication [17]. MimiVax's duty runs to its own shareholders, and supplying data that helps a rival secure the first approved GBM immunotherapy would help foreclose its own commercial path. Its neuroendocrine pivot is fully explained by its own rationale, that survivin is a target across multiple cancers [19], with no coordination story required.
The Direction-of-Effect Concern Is Narrowed but Contested
22. Whether a contemporary control arm would change DCVax-L's measured benefit is genuinely disputed, and a regulator would see both sides. Population data show glioblastoma survival rising over calendar time: a National Cancer Database analysis of 127,737 patients found 3-year overall survival rose from 10.0% to 15.5% and 2-year from 17.6% to 24.6% between 2004 to 2007 and 2016 to 2019, attributed largely to increased uptake of trimodal therapy [24]. A SEER analysis of 46,106 cases went further, reporting that the downward trend in hazard over calendar time persisted even after adjusting for age, sex, resection extent, and treatment type, and concluding that matching contemporary patients to noncontemporary controls on those factors may be insufficient [25]. On its face, this supports the concern that older reconstructed controls could flatter a treatment effect.
23. The countervailing evidence is that the gains were concentrated in the post-Stupp ramp and appear to plateau in the window most relevant to this trial. A 2025 Neuro-Oncology analysis of 3,061 patients across eight datasets and nineteen randomized trials found no detectable temporal drift in standard-of-care survival from 2012 to 2022 after covariate adjustment [14]. DCVax-L enrolled from 2007 to 2015, with most patients accrued from 2012 onward, and drew its controls from contemporaneous trials, so the 2012-onward plateau is the directly relevant period, where the drift signal is weakest. The same analysis also found trial-enrolled patients had inferior survival to non-trial patients after adjustment (HR 1.30) [14]; because DCVax-L drew its controls from trial control arms, its comparator may be a conservative benchmark rather than an inflated one. The honest synthesis is bounded and symmetric: the concern is live, not defused, because the adjusted analyses themselves disagree on whether residual drift remains; but the period most relevant to DCVax-L is the one where drift is least apparent, and the trial-versus-non-trial gap cuts against the assumption of a weak comparator. This unresolved methodological question is itself one more substantive reason a first-in-class externally controlled file draws a long, careful review.
Both Gating Theories Fail as Inferences
24. The coordination thesis is a conjunction of conditions that must all hold at once: an agreement exists, it stayed undisclosed, the submitted framework could absorb outside data, MimiVax would cooperate against its own interest, the borrowed data moves the effect favorably, and this explains the timing. A conjunction can only get less probable with each added condition, so a story needing six things simultaneously true is far less likely than any one of them. Specificity is not evidence.
25. Neither theory has a null hypothesis. Each reads every outcome as confirmation, which makes it unfalsifiable and useless as a decision tool. A good ultimate outcome would not vindicate the reasoning either; treating outcome as proof of thesis is outcome bias. Both theories also convert ordinary bad news into reassuring hidden narratives, which is a pattern that deserves more scrutiny, not less, when it supports a position.
26. Calibration cuts both ways. Rejecting the exotic theories does not license an equally unfalsifiable dismissal, and it equally does not license adopting the opposite advocacy framing that “three independent vectors converge to prove the result.” The evidence points to specific, nameable gating items, and those are independently checkable.
The Strongest Version of Each Theory, and Why It Still Fails
The guidance theory, steelmanned. The strongest form is that DCVax-L is the first major externally controlled oncology MAA the MHRA has assessed, that the agency was visibly building its external-control position during the same window [2][4], and that a regulator still forming its stance moves cautiously on the first such file, so the guidance and the slow review share a common cause. That is coherent. But a common cause that slows assessment is not the application being gated by a document. The effect is captured by first-in-class methodology assessment, a named gating item, and the recent validation of the method [12] makes the literal “waiting on guidance” mechanism even less necessary as an explanation. The defensible core collapses into “novel, restructured methodology takes longer to assess.”
The coordination theory, steelmanned. The strongest form is that contemporary control data genuinely matters for valuation, that assessors want a current benchmark, and that the two groups share a real institutional nexus at Roswell Park. But relevance to valuation is not gating of the authorization, and it runs to NICE's appraisal, not the MHRA decision. The SURVIVE data are blinded, undisclosed, and only now in analysis; the submitted framework cannot absorb a blinded outside arm; the trail is absent; and the incentives are backwards. The kernel is real but lands on a different decision than the one the thesis claims is gated, and it is satisfied by routine supplementary analysis, not a covert transfer.
The Checkable Test, Resolved as of Late May 2026
27. The proposed kill-condition was: if MHRA authorization lands before SurVaxM's final analysis publishes, the coordination thesis is dead. As of late May 2026 neither has occurred, so the race is undecided and the test has not yet falsified the thesis on its own terms. But the mechanism is already refuted independently: SURVIVE's data are randomized, blinded, barred from disclosure, and only now entering analysis [17][18][19], while DCVax-L's review has run since December 2023 [6]. Data that does not yet exist in analyzed, releasable form cannot feed a review that predates it by more than two years.
What Survives
The evidence supports a narrow, defensible conclusion. The delay is explained, more than adequately, by a restructured trial, reconstructed controls, a reclassified population, first-in-class manufacturing, and the extraordinary scrutiny external-control evidence draws everywhere. The external-control method DCVax-L used now has empirical support in glioblastoma [12], which removes one of the strongest 2023 objections, though the trial-specific questions remain. Whether a contemporary control arm would materially change the measured effect is contested rather than settled, and that uncertainty is itself a substantive review item. Contemporary control data matters for QALY valuation under NICE, and that stands on its own. The WHO 2021 reclassification remains a genuinely open interpretive question: the trial measured IDH status for its treated patients but never reported the distribution, and its external controls predate IDH testing, so it turns on data that exists for one arm and not the other.
None of this requires, implies, or supports the claim that an outside trial or an unfinalized guidance document is gating the authorization. Nor does the contrary advocacy claim, that academic and regulatory developments “converge to prove” the result, follow from the evidence: those developments support the method and the comparator landscape without establishing the marketing decision. Keep the verified facts, hold the interpretations of both sides at arm's length, and the gating question has a mundane answer.
A Note on Sourcing
The pivotal trial figures in this document, including the hazard ratios of 0.80 for newly diagnosed and 0.58 for recurrent disease, the MGMT-methylated subgroup hazard ratio of 0.74, the comparator sizes of 1,366 and 640, the restructuring history, the reconstruction method, and the central IDH measurement, have been verified against the full text of the primary article [8]. The INSIGhT reanalysis estimates (hazard ratios 1.00, 0.93, and 0.88, all consistent with no benefit) are verified against the primary publication [12]. The MHRA, NICE, HTA, and SURVIVE facts derive from primary regulatory pages, official company releases, or the cited peer-reviewed papers. The direction-of-effect question in Section 7 is presented as genuinely contested: population datasets show glioblastoma survival improving over calendar time and one adjusted analysis finds residual drift, while a second adjusted analysis covering the period most relevant to this trial finds none, and a regulator would weigh both.
Sources
[1] DCVax-L for treating glioblastoma [ID836], Project information | NICE (scope: newly diagnosed only; in progress). https://t.co/q0Y5Z6Q0yT
[2] MHRA draft guideline on external control arms based on real-world data, consultation page | https://t.co/umkhtzSywU (20 May to 14 July 2025; closed, under analysis; CHM RWD ad hoc group). https://t.co/i0AslAeoBx
[3] Draft MHRA Guideline on Studies with RWD ECA, May 2025 (general principles for prior-trial controls). https://t.co/IfJFLmSLHD
[4] MHRA guidance on the use of real-world data in clinical studies, series overview | https://t.co/umkhtzSywU. https://t.co/GwlqeuA2rX
[5] External Control Arms Based on Real World Data: MHRA Consultation Opens | Lexology (excludes synthetic/virtual arms; general principles for prior-trial controls). https://t.co/KhinB0pkmP
[6] NWBO Announces MAA Submitted to UK MHRA for DCVax-L | Northwest Biotherapeutics, 21 Dec 2023 (150-day pathway; gating items named). https://t.co/zOc82O4CVR
[7] NWBO and Advent receive MIA license for commercial cell-therapy manufacturing at Sawston, Mar 2023. https://t.co/gtyD6SV3W1
[8] Liau LM, Ashkan K, Brem S, et al. Association of autologous tumor lysate-loaded dendritic cell vaccination with extension of survival among patients with newly diagnosed and recurrent glioblastoma: a phase 3 prospective externally controlled cohort trial. JAMA Oncol. 2023;9(1):112-121. doi:10.1001/jamaoncol.2022.5370. https://t.co/0wES9PEMr2 (PMID 36394838; PMC9673026. Verified against the primary full text via PubMed/PMC: nGBM mOS 19.3 vs 16.5 months, HR 0.80, P=.002; rGBM mOS 13.2 vs 7.8 months, HR 0.58, P<.001; MGMT-methylated HR 0.74, P=.03; nGBM sensitivity-analysis HR range 0.77-0.82; external controls of 1,366 from five RCTs and 640 from ten RCTs, selected by York Health Economics Consortium and matched on 14 SAP-prespecified criteria; IPD unavailable so controls reconstructed by Guyot digitization with MAIC adjustment; originally randomized 2:1 double-blind with PFS primary, refocused on OS; IDH R132 status determined centrally for treated patients).
[9] Liau LM, Ashkan K, Tran DD, et al. First Results on Survival From a Large Phase 3 Trial of an Autologous Dendritic Cell Vaccine in Newly Diagnosed Glioblastoma. J Transl Med. 2018;16(1):142. doi:10.1186/s12967-018-1507-6 (original 2:1 randomization; PFS primary, OS secondary; crossover).
[10] Olivier T, Migliorini D. Autologous tumor lysate-loaded dendritic cell vaccination in glioblastoma: what happened to the evidence? Rev Neurol. 2023;179(5):502-505. doi:10.1016/j.neurol.2023.03.014 (endpoint modified to OS; external controls in an originally randomized trial; recurrent population added; unplanned analyses).
[11] Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced Secondary Analysis of Survival Data: Reconstructing the Data From Published Kaplan-Meier Survival Curves. BMC Med Res Methodol. 2012;12:9. doi:10.1186/1471-2288-12-9.
@EatYerShorts@bradsmithnz First one gets the sweetest deal, next one gets a break, after that…
Well, after that…
I mean after all of that…
Think about all of it. I mean think about that…
And then look at this judges actions thus far $NWBO
After the second deal, y’all can all go Frack yourselves
Brokers keep fighting it? NWBO files a motion to compel + sanctions.
Stein has already shown he’ll referee this thing aggressively.
August 28 fact discovery deadline is the backstop, but the real action is happening this summer. 👇
Once that data drops, depositions go nuclear.
Key broker traders, compliance people, and algo guys on the stand UNDER OATH.
That’s when the real manipulation story starts spilling out. 👇
If Stein backs NWBO's push, MMs get forced to cough up full productions, complete privilege logs, algos, comms, and proper trading data by June 26.
That would be a hard hammer coming down on their slow-walking asses. 👇



















![hoffmann6383's tweet photo. ✅️Algorithms Discoverable?
The federal magistrate judge in $NWBO's spoofing lawsuit against six of the largest market makers in the world, including Citadel and Vitru, believes that the Defendant market makers' trading algorithms are discoverable
The Magistrate Judge stated, in relevant part:
"I'm not sure how that gets limited, frankly." [1]
See attached Image.
[1] Docket #286, https://t.co/2vLwDOXAki](https://pbs.twimg.com/media/HJ77xJCWcAE5jwb.jpg)

























