🆘️💔🆘️ A handsome Golden Retriever should never be waiting in a high kill shelter. 6 yo MARBLES is at Deadly Devore in San Bernardino County #California. Please help him be seen for a #SoCal forever or foster home 🙏 info 🔽 #A846284
"Their owner passed away alone in his apartment. Nobody found him for three days. The dogs waited the whole time." When animal control finally arrived, Max and Buddy were sitting by the front door. Not destructive. Not panicked. Just sitting. Waiting. Doing what he had always taught them to do. They came to our shelter with nothing. No records. No vet history. No family contact. Just each other. And one old tennis ball that somebody thought to grab on the way out. That was eleven days ago. Every morning they sit at the kennel door and wait. Every time they hear footsteps they both stand up. Every time those footsteps pass — they go back and lie down together. They don't know he's not coming. They just know he always came back before. Max is 6. Buddy is 5. Both healthy. Both gentle. Both heartbreakingly good dogs. Neither one will do well separated. They have never spent a night apart. They were somebody's whole world. Now they need somebody to be theirs. If you are in the USA and you have room in your home and your heart — please share this until it reaches the right person. They've already waited long enough. Drop a ❤️ for Max and Buddy. And please — SHARE. One share could be everything.
It's impossible to describe how devastating it is to see more & more people being diagnosed with #ME year after year, knowing there's still no treatment & Drs are still so dangerously misinformed
When I 1st became ill 39 yrs ago, I could never have imagined it still be this way
Where does it go when you lose it? When you feel as if you’re in a dream watching your life unfold somewhere else? Where is that place? When you can sense yourself but you feel that it is not truly in you? Where has it gone? Where do we go when we are lost to the fog? #mecfs
A federal judge rejected the Justice Department's attempt to end a lawsuit challenging Trump's slush fund — saying she didn't trust assertions by administration officials that the fund would not move forward.
Trump has turned the White House into a 24/7 corruption operation. This is a national crisis.
Trump thinks the public will stop paying attention.
So I went to the Senate floor to call his bluff. I told the ENTIRE STORY of his 500 days of corruption.
1/ Here it is - in one🧵
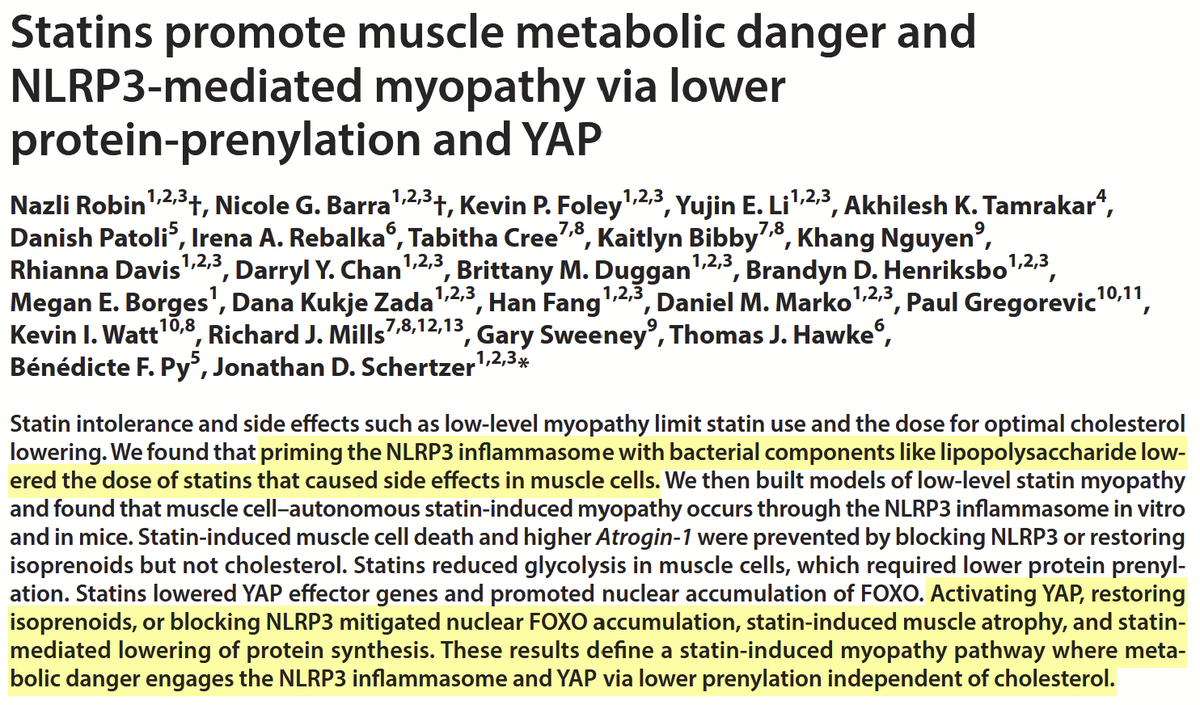
Statin's adverse effects on muscle may be driven by inflammation—not just cholesterol lowering.
This research shows statins can trigger the NLRP3 inflammasome in muscle cells, leading to atrophy, reduced protein synthesis, and cell death via disrupted isoprenoid/prenylation pathways. Blocking NLRP3 or restoring isoprenoids prevented these effects, identifying a potential target to reduce statin-associated myopathy. #Statins #MuscleHealth #Inflammation #AgingResearch
https://t.co/J480WYiq9E
I'm a cardiologist. I prescribe cholesterol-lowering drugs every single day. They save lives. That science is settled and I will never tell you otherwise.
But I'm going to say something that will make a lot of my colleagues uncomfortable — because someone needs to say it, and your doctor probably won't.
Too many physicians make you feel crazy when you bring up statin side effects.
You walk into your appointment and say "my muscles ache constantly" — and you're told it's in your head. You say "I'm exhausted all the time" — and you're told it's your age. You say "my sex drive disappeared" — and you get an awkward silence followed by a subject change. You say "I don't feel like myself anymore" — and you're told the benefits outweigh the risks, take the pill, stop reading the internet.
I've watched it happen in my own field for twenty years. The conversation gets shut down. The patient gets dismissed. And then they do the one thing we should be most afraid of — they stop the medication entirely, without telling us, and lose the cardiovascular protection that's keeping them alive.
That is the real cost of not being honest. Not the side effects themselves — the silence that drives patients away from treatment.
In my practice, I see statin-related complications in at least 25% of my patients. Muscle pain. Fatigue that doesn't resolve with sleep. Reduced sexual drive. Brain fog. Cramping. Joint stiffness. Weakness that makes exercise — the very thing we tell them to do — feel impossible.
Some of these improve with CoQ10 supplementation and optimizing vitamin D. Many do not.
I wrote about the diabetes risk of statins in a New York Times op-ed in 2012. The backlash from the cardiology establishment was immediate. I was told I was undermining trust in a life-saving drug class. Fourteen years later, every major guideline acknowledges the risk I warned about. It's in the prescribing information. The physicians who attacked me for saying it now teach it to their residents.
The truth doesn't care about professional comfort. It never has.
Now a paper published this week in Science Advances has finally explained the mechanism behind statin myopathy — and the finding validates what millions of patients have been telling their doctors for years.
Researchers discovered that statins activate the NLRP3 inflammasome in muscle cells — triggering an inflammatory cascade that causes muscle cell death, activates atrophy pathways, and disrupts muscle metabolism. This is entirely independent of the drug's cholesterol-lowering effect.
The muscle damage isn't caused by lowering cholesterol. It's caused by a completely separate pharmacological action through a different pathway.
The critical implication: the side effect can potentially be separated from the benefit.
Blocking NLRP3 or restoring isoprenoids prevented muscle cell death without interfering with cholesterol reduction. Future therapies could preserve the cardiovascular protection while eliminating the muscle toxicity.
Even more striking — the researchers found that background systemic inflammation significantly lowered the statin dose needed to trigger muscle damage. Patients with chronic inflammation, gut dysbiosis, or metabolic syndrome may be experiencing myopathy at doses their doctors consider "too low to cause problems." They're not imagining it. Their inflammatory state is priming the pathway.
The muscle pain was never in their heads. It was in their NLRP3 inflammasome. And we finally have the molecular proof.
Here's what I actually do in my practice — because I refuse to choose between protecting the heart and respecting the patient.
Whenever possible, I avoid statins as my first-line approach for eligible patients by using alternatives that lower LDL through entirely different mechanisms with no muscle toxicity:
PCSK9 inhibitors — Repatha and Praluent. Injections every 2-4 weeks that dramatically lower LDL without touching muscle tissue. No myopathy. No fatigue. No brain fog. For patients who can access them, these are transformative.
Inclisiran — Leqvio. An siRNA injection I administer twice a year in my office. It silences the PCSK9 gene in the liver. Two shots a year. LDL drops roughly 50%. No muscle side effects. No daily pills. Now approved as first-line monotherapy. This is the future of lipid management and I use it aggressively.
When statins ARE clinically necessary — and sometimes they are, especially post-heart attack or in combination therapy — I choose hydrophilic statins like rosuvastatin or pravastatin. These do not easily cross the blood-brain barrier. The cognitive complaints — the fog, the memory issues, the feeling of "not being yourself" — are substantially less common with these formulations because the drug stays out of the central nervous system.
I never prescribe a statin without CoQ10. 100-300mg daily. Statins deplete the cellular energy molecule your muscles and heart depend on. Replenishing it reduces muscle symptoms in many patients. It should be standard practice. The fact that it isn't is a failure of our field.
I check vitamin D and optimize it aggressively. Low vitamin D — which is epidemic — worsens muscle symptoms independently and compounds whatever the statin is doing. Target 50-80 ng/mL, not the bare minimum of 30.
Bempedoic acid — Nexletol — for patients who can't tolerate any statin. Works upstream in the cholesterol pathway and is not active in muscle tissue. Specifically designed to avoid myopathy.
Ezetimibe added to a lower statin dose. Cut the statin intensity, add ezetimibe to maintain the LDL reduction, and halve the muscle exposure.
There is no excuse in 2026 for telling a patient "just deal with the muscle pain." The toolbox is deep. The alternatives exist. The only barrier is a physician's willingness to listen and adapt.
I want to speak directly to every patient who has been dismissed.
Your muscle pain is real. Your fatigue is real. Your cognitive changes are real. Your loss of drive — in every sense of the word — is real. A paper in Science Advances just proved the mechanism. You were never crazy. You were experiencing a documented inflammatory response in your muscle tissue that your doctor didn't have the science to explain — until this week.
And I want to speak directly to my colleagues.
We have to be honest. Not just about the benefits — which are enormous and undeniable — but about the side effects, the mechanism, and the alternatives. Patients who feel heard stay on treatment. Patients who feel dismissed stop their medications in silence — and die from the heart attacks we could have prevented if we'd simply been willing to have an honest conversation and switch the approach.
The cardiologist who tells you statins are flawless is not protecting you. The wellness influencer who tells you statins are poison is not protecting you either. The truth lives in the middle — where it always has.
Statins save lives. The side effects are real. The mechanism is now proven. The alternatives exist. And you deserve a doctor who holds all four of those truths at the same time.
Both things can be true. They always could.
Now we have the science to prove it.
A video exploration of the impossible decisions ME/CFS patients have to make, constantly having to decide between two options that will both make our health worse. And how much more difficult these decisions get when they involve non ME/CFS medical needs. As well as thoughts on how to process these decisions…
A more comprehensive essay of these ideas in writing is in the works for a future text post… stay tuned! 😊💙
♿️ audio and text versions on my blog 👇
https://t.co/vejr6PX62D
———————
#mecfs #LongCovid #ChronicIllness #pwME #spoonie
This is a devastating interview.
Scott Pelley tells the NYT that Bari Weiss directly put a “thumb on the scale” for Trump over the killing of Renee Good.
Here’s his explanation of exactly what happened.
Imagine watching everything you care about in a house that starts to catch fire. And there’s a firehose one meter from you, but you're tied to a chair and can’t move. So you have to sit there and watch it all burn. That is everyday, over and over again, living with #MECFS 💙
“Having ME is not a choice.”
A 37-year-old woman with severe #MECFS says the disability assessment process in Switzerland is “simply dangerous and unsuitable for people like us”.
Clip from Swiss TV on severe #MECFS.
Dr Nigel Speight explains why the term ME carries more weight than “Chronic Fatigue Syndrome” and how it would be like renaming Alzheimer’s “Chronic Forgetfulness Syndrome”.
He also describes how a boy’s CFS diagnosis was weakened, leaving the family open to prosecution.
People don’t realise how much you can lose and still have to live every hour.
I’ve lost walking, my brain, normal vision, friends, food, music, love, career, hobbies, sunlight, sleep…
I can’t even grieve it without getting sicker.
Disease takes more than you realise you had.
George Monbiot describes the treatment of #MECFS as “The Greatest Medical Scandal of the 21st century”. Repost of the introduction to my 27-minute explainer video for #MEAwarenessMonth — now optimised for phones.
1 in 200 humans on earth are missing from their own lives due to ME. ME is a devastating physical illness that makes rubble of the lives of patients and families. Clinically, we’ve known it’s real for decades. Biologically, we had proof by the 1990s. But society still acts like it’s not real. This is a historic injustice. #MEAwarenessDay
On International ME/CFS Awareness Day, we stand with millions of people living with a disease that has too often been misunderstood, underestimated, and neglected. ME/CFS patients deserve visibility, dignity, and a scientific response equal to the severity of their illness.