🫀POCUS is no longer just a bedside imaging tool.
It is becoming real time physiological intelligence.
This excellent 2026 review highlights how modern POCUS is expanding into:
• ultrasound guided regional anesthesia
• shock and cardiac arrest management
• AI assisted imaging
• advanced diagnostics
• governance and medicolegal practice
Some of the most provocative concepts: • “Occult VF” detectable only on echocardiography during cardiac arrest
• Ultrasound guided CPR compression positioning
• AI assisted lung ultrasound acquisition by nonexperts
• Handheld devices approaching cart based diagnostic performance
One important medicolegal message: several lawsuits involved failure to perform POCUS when clinically indicated.
The future of emergency and critical care medicine will likely depend on clinicians capable of integrating: physiology + imaging + AI + rapid bedside decision making.
POCUS is not anymore an “optional skill” but “core clinical infrastructure.”
Mani N, Rao S, Kim DJ. Point-of-care ultrasound in the modern era of emergency medicine: a narrative review of the recent literature. Curr Opin Crit Care. 2026. doi:10.1097/MCC.0000000000001358
🫀🤓Pressure does not move blood. Energy does.
This outstanding review challenges one of the most deeply rooted concepts in haemodynamic management: the idea that pressure variables are the primary drivers of circulation. Instead, the authors propose a physiology framework where the heart supplies energy, the vasculature defines constraints, and pressures merely reflect system state.
Several concepts deserve special attention for critical care clinicians:
• Mean systemic pressure does not “drive” flow
• Right atrial pressure is a dependent variable, not a therapeutic target
• Venous return depends on inflow acceptance and inlet impedance
• Raising pressure without improving flow may worsen congestion
• Shock should be interpreted as either impaired venous delivery or impaired cardiac acceptance
Clinically, this framework helps explain why:
• CVP-guided fluid loading often fails
• Vasopressors may normalize MAP without restoring perfusion
• Congestion can coexist with preserved arterial pressure
• Flow responsiveness matters more than static pressure targets
One of the strongest messages of the paper is simple but powerful:
“Pressure is not perfusion.”
For intensivists, anesthesiologists, and cardiogenic shock teams, this review is worth reading in full. It reconnects bedside haemodynamics with first-principles physiology.
Miller A, Anaesthesia. 2026. https://t.co/ejjvREUe7c
🫀 Hemodynamics is not blood pressure... actually, It never was.
⚠️ The biggest mistake in perioperative & critical care:
👉 Treating numbers instead of physiology
📊 What we were taught
✔️ BP
✔️ HR
✔️ SpO₂
🔥 What actually matters
👉 Flow + oxygen delivery + tissue perfusion
🧠 Core concept
👉 Blood pressure ≠ perfusion
You can have:
▪️ Normal BP → low cardiac output
▪️ High BP → poor microcirculation
▪️ Stable vitals → ongoing hypoxia
💡 Why?
Because:
👉 BP = CO × SVR
Same pressure
→ completely different physiology
🧬 The real pillars of hemodynamics
✔️ Cardiac output
✔️ Stroke volume
✔️ Preload / afterload / contractility
✔️ Oxygen delivery (DO₂)
⚠️ Critical insight
👉 Oxygen delivery = CO × arterial O₂ content
Not:
❌ BP
❌ SpO₂ alone
🔥 This is where advanced monitoring changes everything
👉 From static → dynamic
👉 From guess → prediction
🧠 Dynamic parameters outperform static ones
✔️ SVV
✔️ PPV
✔️ PVI
👉 Predict fluid responsiveness
👉 Avoid fluid overload
💥 Reality check
Only ~50% of unstable patients respond to fluids
👉 The rest get harm
🫀 Next level thinking
👉 Ventriculo-arterial coupling
👉 Cardiac power output
👉 Tissue perfusion markers
🚨 Final message
Stop asking:
❌ “What is the blood pressure?”
Start asking:
👉 “Is the patient perfusing?”
🧠 Because in critical care:
👉 Flow saves organs
Pressure just looks good on the monitor
📚 Demir et al., Aydın et al.
Turkish Journal of Anaesthesiology & Reanimation, 2025
DOI: 10.4274/TJAR.2025.251926
DOI: 10.4274/TJAR.2025.251925
🫁 Why I always ask for paired blood gases! CO2 and hemodynamics 🧪
For years, we have relied on:
▪️ Lactate
▪️ ScvO₂ / SvO₂
▪️ Clinical perfusion
But all of them share a critical limitation:
👉 They do not reliably detect ongoing tissue hypoperfusion
⚠️ The problem
You can have:
✔️ Normal ScvO₂
✔️ Decreasing lactate
✔️ “Stable” hemodynamics
…and still have microcirculatory failure
👉 This is where CO₂ enters the game
🧠 The physiology in short
CO₂ behaves differently from oxygen:
➡️ ~20x more diffusible than O₂
➡️ Accumulates when flow is insufficient
➡️ Reflects flow adequacy, not just oxygenation
👉 Pv-aCO₂ ≈ inverse of cardiac output
🔥 What the CO₂ gap really tells you
🟢 Pv–aCO₂ < 6 mmHg → Likely adequate flow
🔴 Pv–aCO₂ ≥ 6 mmHg → Suggests low flow / impaired perfusion
BUT:
❗ It is NOT a marker of hypoxia alone
❗ It is a marker of flow–metabolism mismatch
⚡ The real upgrade: the CO₂/O₂ ratio
👉 Pv-aCO₂ / Ca-vO₂
This is the missing piece.
✔️ Approximates respiratory quotient
✔️ Detects anaerobic metabolism
✔️ Reacts faster than lactate
📈 >1 = ongoing anaerobic metabolism
🚨 Clinical implications
🩸 Septic shock
High CO₂ gap despite ScvO₂ >70% → hidden hypoperfusion
Persistent Pv–aCO₂ ≥6 mmHg → ↑ mortality
🫀 Fluid responsiveness
↓ Pv–aCO₂ after fluids → likely responder
🫁 Weaning failure
↑ CO₂ gap during SBT → inadequate DO₂ vs VO₂
🏥 Post-op patients
Elevated CO₂ gap predicts complications better than lactate
❌ Common mistakes
❌ Using lactate alone
❌ Ignoring normal ScvO₂ “false reassurance”
❌ Interpreting CO₂ gap without context (pH, Hb, ventilation)
❌ Treating numbers instead of physiology
🚀 Modern hemodynamic approach
We should integrate:
1. Macrocirculation → MAP, CO
2. Oxygen markers → ScvO₂
3. Metabolic markers → Lactate
4. Flow markers → Pv–aCO₂
5. Anaerobic markers → Pv–aCO₂ / Ca–vO₂
👉 Not one variable
👉 A physiology-driven bundle
🎯 Take-home
CO₂ is not a waste product.
👉 It is a real-time marker of perfusion adequacy
👉 It detects what oxygen variables miss
👉 It bridges macro and microcirculation
📚 Mallat J et al. (2025)
Annals of Intensive Care
DOI: 10.1186/s13613-025-01569-2
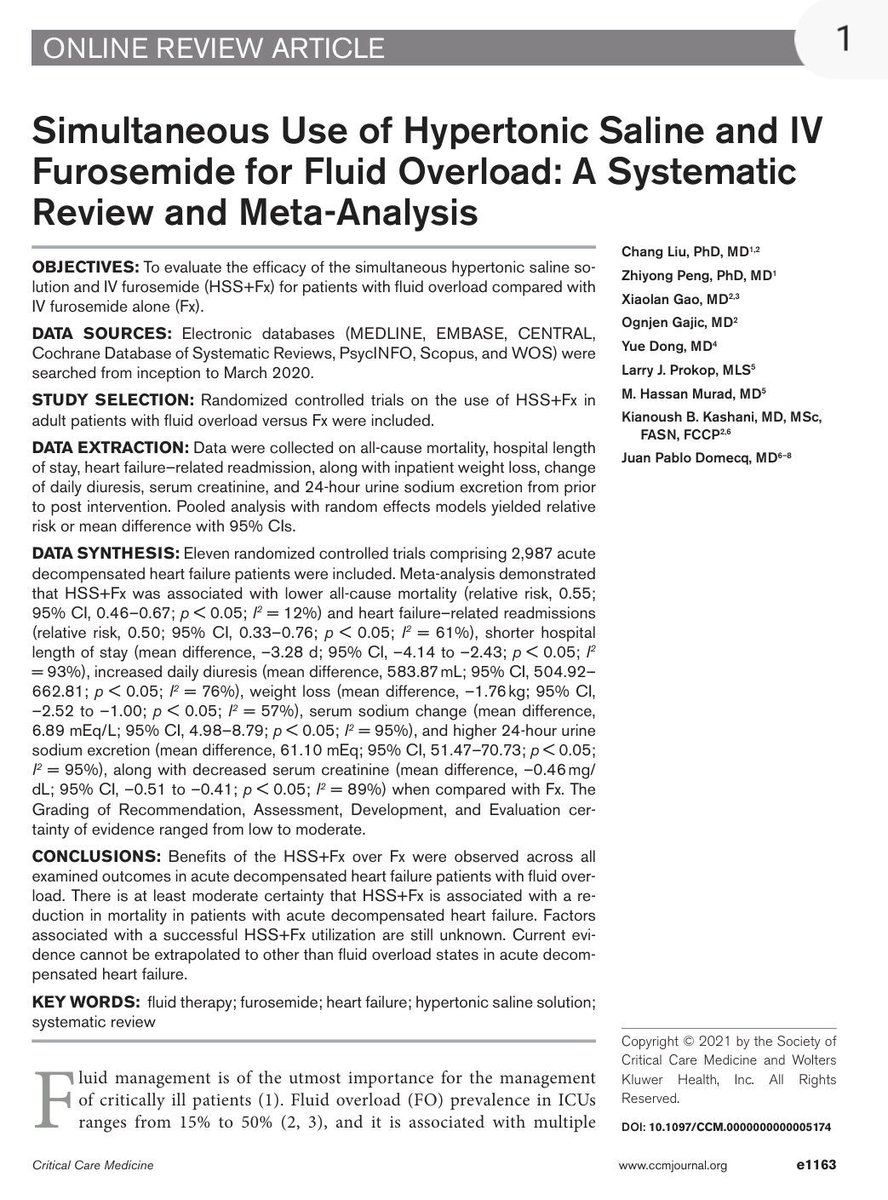
💧 Hypertonic saline + furosemide in fluid overload.
Fluid overload remains a major driver of morbidity and mortality in critically ill patients and acute decompensated heart failure.
A systematic review and meta analysis evaluating the combination of hypertonic saline solution with intravenous furosemide provides important insights into a potential strategy to enhance decongestion.
🔑 Key findings:
• 11 randomized controlled trials
• 2987 patients with acute decompensated heart failure
• Compared with furosemide alone, the combination therapy was associated with:
Reduced all cause mortality
Reduced heart failure related readmissions
Shorter hospital length of stay
• Improved decongestion profile:
Higher daily diuresis
Greater weight loss
Increased natriuresis
Reduction in serum creatinine
• Physiological interpretation:
Hypertonic saline may improve intravascular refill and renal perfusion
Enhances diuretic response and sodium excretion
Potentially overcomes diuretic resistance
👉 Clinical perspective:
This strategy may be particularly useful in patients with diuretic resistance and severe congestion
However, evidence remains moderate and should be individualized
👉 Bottom line:
Not just removing fluid
Optimizing the intravascular compartment is key
📖 Reference
Liu C, Peng Z, Gao X, et al. Simultaneous use of hypertonic saline and IV furosemide for fluid overload. Critical Care Medicine. 2021. doi:10.1097/CCM.0000000000005174
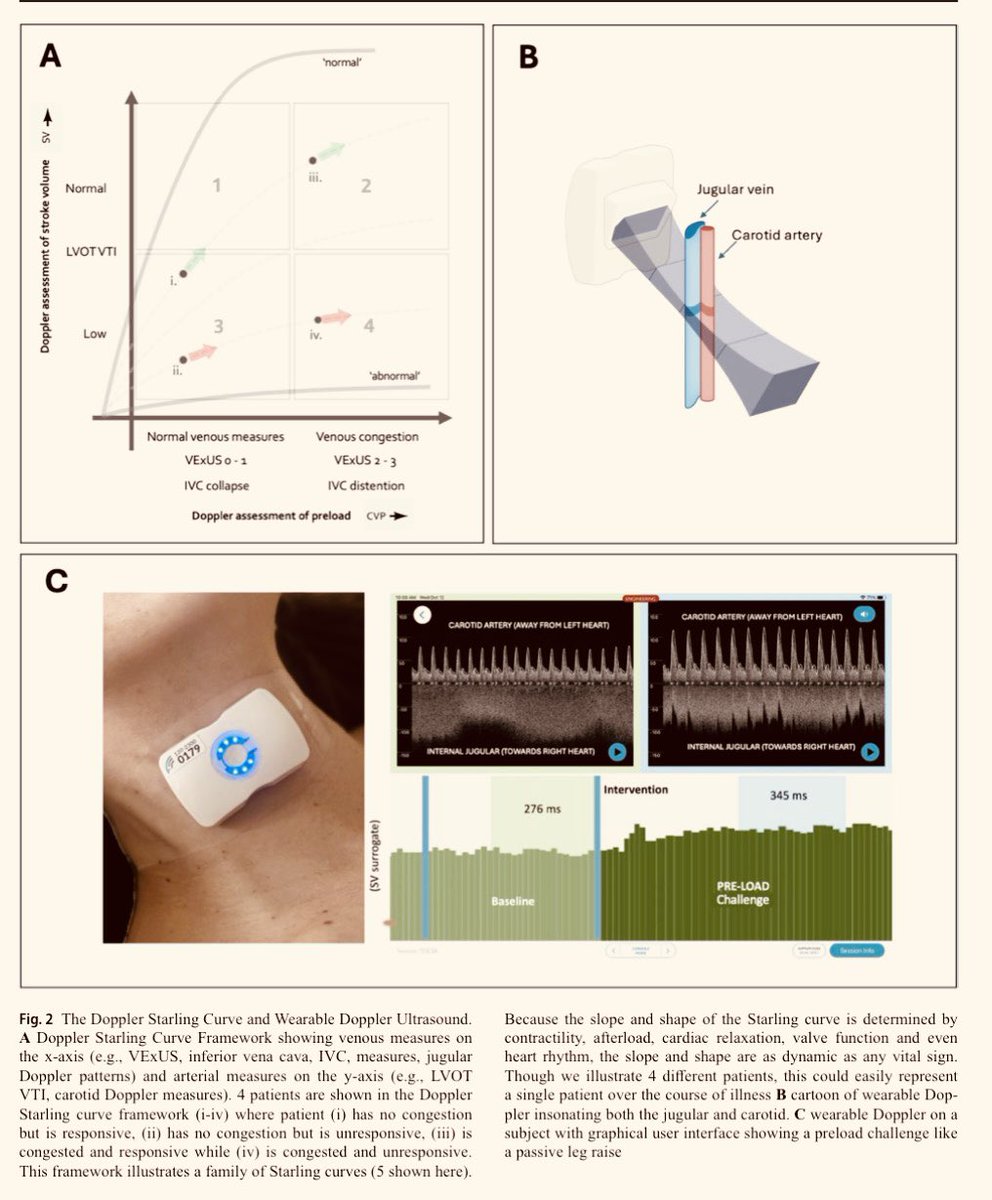
🚨 Just published! We validated an ultrasound-based score combining VExUS + LUS to guide decongestion in acute heart failure. A step forward toward more precise, ultrasound-driven management. Proud of our team! Congrats Henrique!
https://t.co/tFNWHvc56S
Protocolo SaFER: Combinación de Vexus /ITV en resucitación:
a) Sin congestión, sensible, b) Sin congestión, sin respuesta, c) Congestión, sensible, d) congestión, sin respuesta…
https://t.co/VcVetclWq1
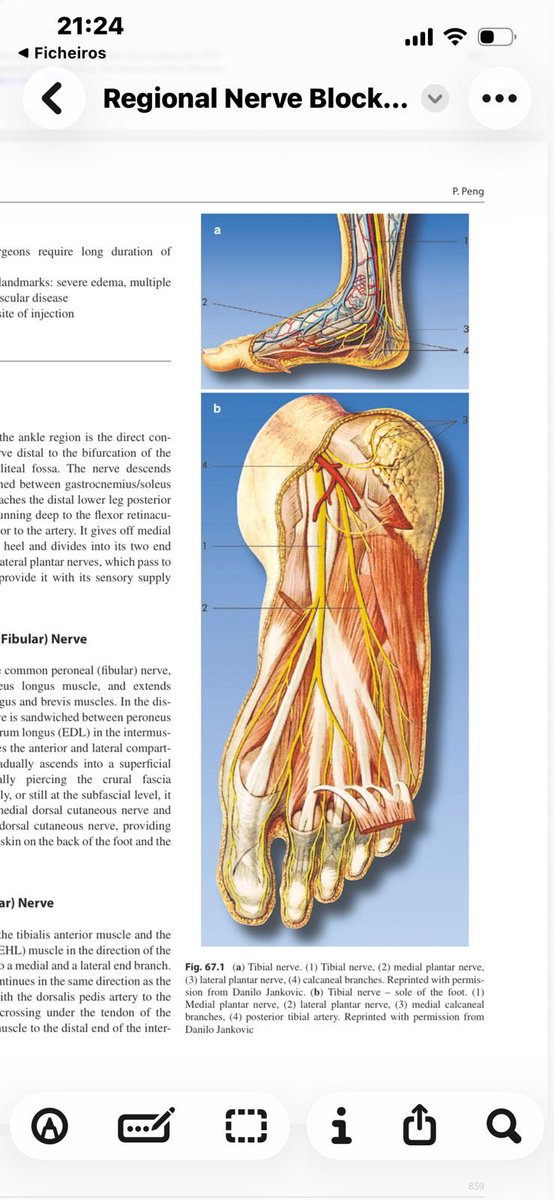
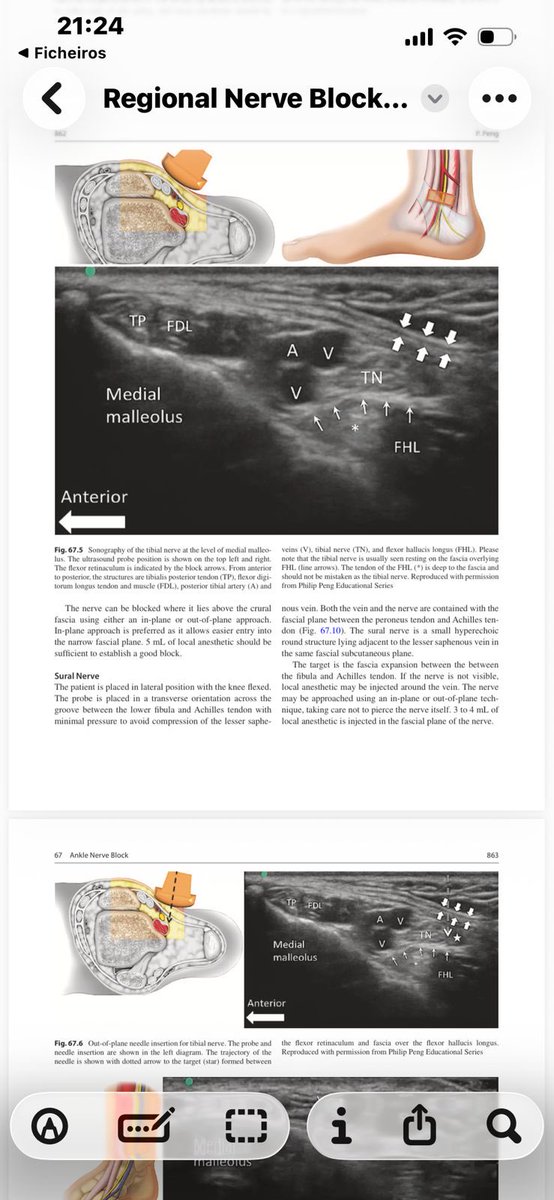
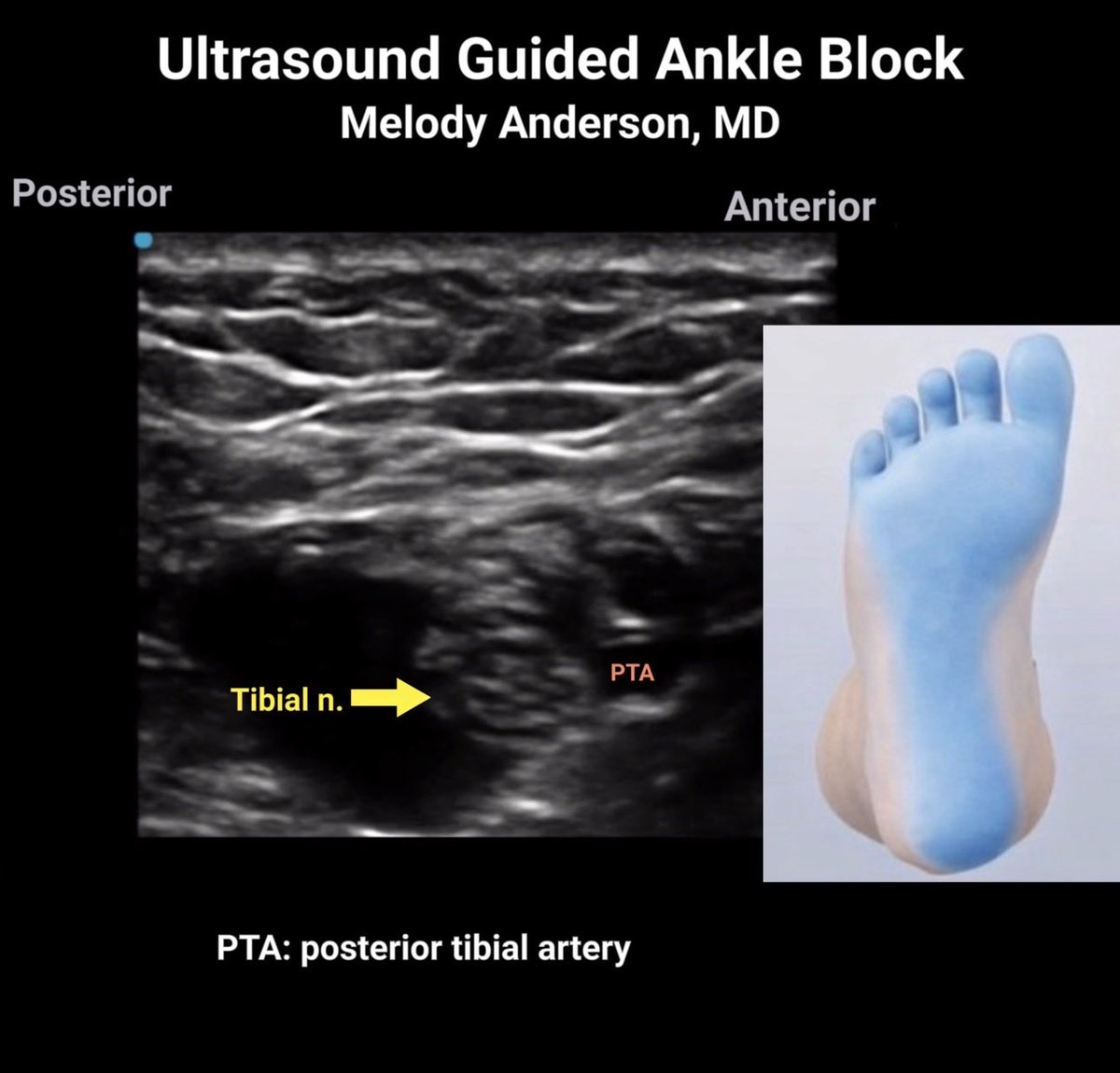
Updated ankle block video 🔗 with Anatomy pearl 🦵 :
There are two tibial arteries (anterior & posterior)…
but only one tibial nerve
https://t.co/AlhNLvcwl0
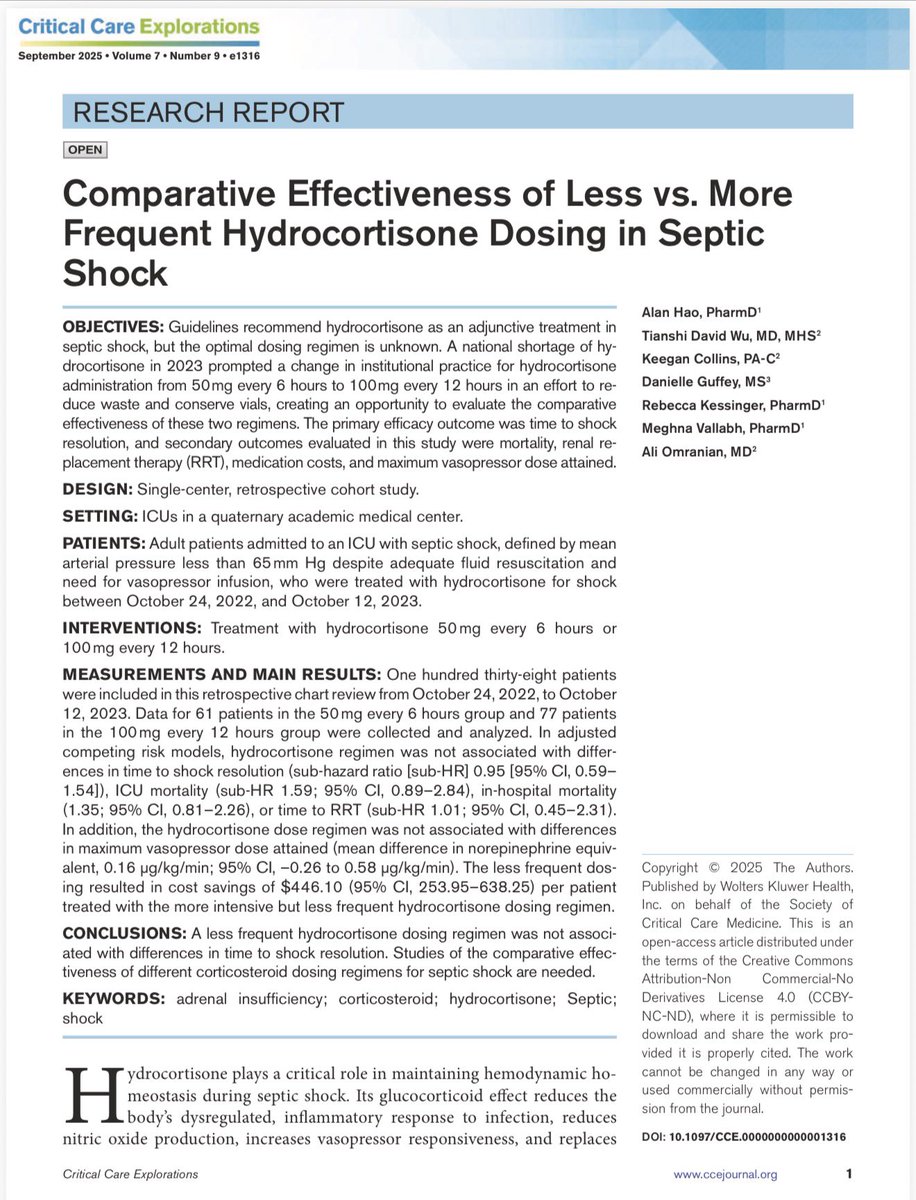
¿Importa cada cuánto das hidrocortisona en el choque séptico?
Estudio retrospectivo (n=138) comparó:
50 mg c/6 h vs 100 mg c/12 h (200 mg/día en ambos).
1️⃣Resultado primario Tiempo a resolución del choque: sin diferencia
Sub-HR 0.95 (IC 95% 0.59–1.54)
💀Mortalidad UCI: HR 1.59 (IC 95% 0.89–2.84) Hospitalaria: HR 1.35 (IC 95% 0.81–2.26) sin diferencia
💵 100 mg c/12 h ahorra aproximadamente 446 USD por paciente.
Menor frecuencia de dosificación logra los mismos desenlaces clínicos, con menor costo y menos desperdicio.
La tradición no supera a la farmacocinética
🔗 https://t.co/WpwmQMzueO
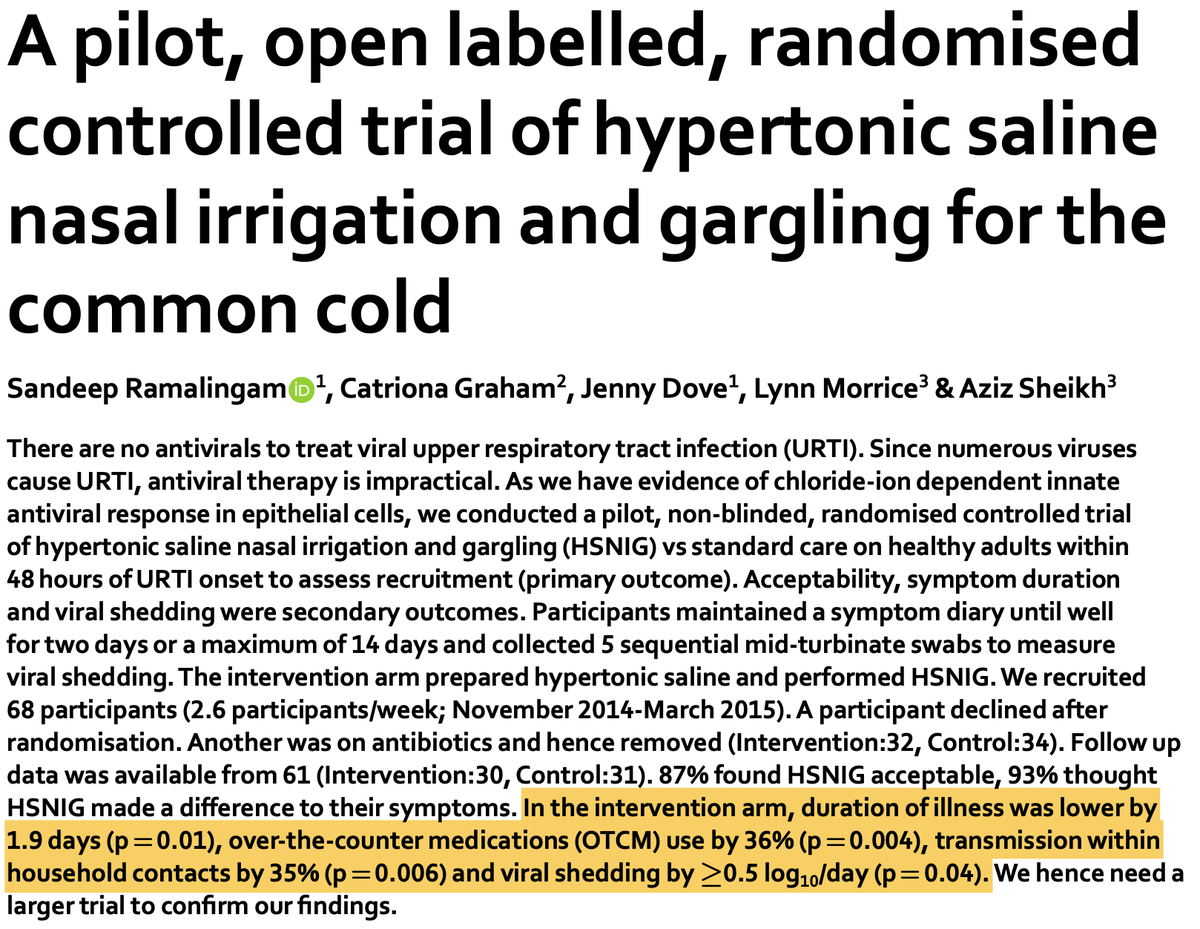
Washing viruses out of your nose and throat can help you get better faster
In an RCT of 66 adults, hypertonic saline nasal irrigation and gargling:
1) Cut cold duration by 22% (1.9 days shorter)
2) Reduced household transmission by 35%
Right ventricular dilation can easily be screened for in multiple cardiac views. This can be done both qualitatively, by visually inspecting the relative size of the right ventricle compared to the left, and quantitatively, by measuring it.
#medtwitter#cardiotwitter#foamed
For all the new medical students starting this fall there are 10 lessons they don’t teach in medical school (but should) @ross_prager
https://t.co/tZ5GmLeKtf
@SchulichMedDent@WesternU
Redo🧵regarding 'straightening the wire' during central line placement.
There are a few of my 🧵worth repeating for each group of new interns; IMO this is definitely one of them.
If you do a lot of central lines, this technique will come in handy over and over again.
(1/ )
Transcranial #Doppler in the Emergency Department: A Clinical Application and Quick Reference
(I like this orientation pic 👇compared to the traditional skull-based illustration)
🔗 https://t.co/P36YmA3Hpt
#POCUS#FOAMed#TCD
🩺 Auscultar no es tan fácil como parece.
Muchos médicos solo reconocen el soplo sistólico... y poco más.
Hoy te explico con sonidos reales cómo hacer una buena auscultación cardíaca ✅
Prepara los auriculares 🧵👇