Love is in the air—and so is our commitment to healthy lungs. 🫁🫶
Happy Valentine’s Day from CHEST!💘💗
Share the love and tag someone who inspires you.
#LoveYourLungs#HappyValentinesDay#ACCPCHEST
Hospital corridor care is not something we should be writing into guidelines
Its not an escalation plan
Its the sole product of a system thats been neglected
I DETEST corridor care. We’ve been doing it since August.
Confirming asthma diagnosis once inhaled corticosteroids (ICS) are started can be difficult. If asthma is well-controlled, stepping down ICS may help with diagnosis. Start with assessment – see highlighted section GINA 2024 Box 1-5. Full explanation at https://t.co/Cm9ADXmsOb
@GeriSoc The North-West meets begins
Thank you for giving me the opportunity to present the pilot project. Also giving an opportunity to get up to date with best practise for the care of elderly
#BGSconf.
The X-ray results indicate that AE has referred the patient due to an unclear cause of infection. Looks like we need to put on our X-ray glasses to get to the bottom of this! 👓
🌏Respirology
Allergic broncho-pulmonary #aspergillosis: Old disease, new frontiers! Don't miss this expert view on the matter in #Respirology#OpenAccess
https://t.co/AloMK6hGZ5
I'm an A&E consultant and I'm tired after a weekend of nights.
But this am, I've handed over what I described as a "good department". This was said genuinely and with no hint of irony.
We provided great care and have very short waits to see an A&E doctor, but I'd forgotten how unacceptable it was to have 18 patients in the corridor, and elderly patients waiting over 2 days for a ward bed.
My lens of what is good and acceptable has been slowly warped by the slow & damaging effect of the working conditions of A&E departments up and down the country.
My biggest worry is that I'm starting to accept the unacceptable.
This is not about a lack of gp appointments, patients "abusing" the system or poor management - in fact we had excellent hospital management support, with patients boarding on each ward waiting there instead of A&E for a bed.
This is a simple case of patient demand being greater than what the overall health economy can cope with.
We have to either change the way we work, change demand via expectation management or increase resources.
If not, then the unacceptable becomes the norm and that's unacceptable.
Our patients and staff deserve better.
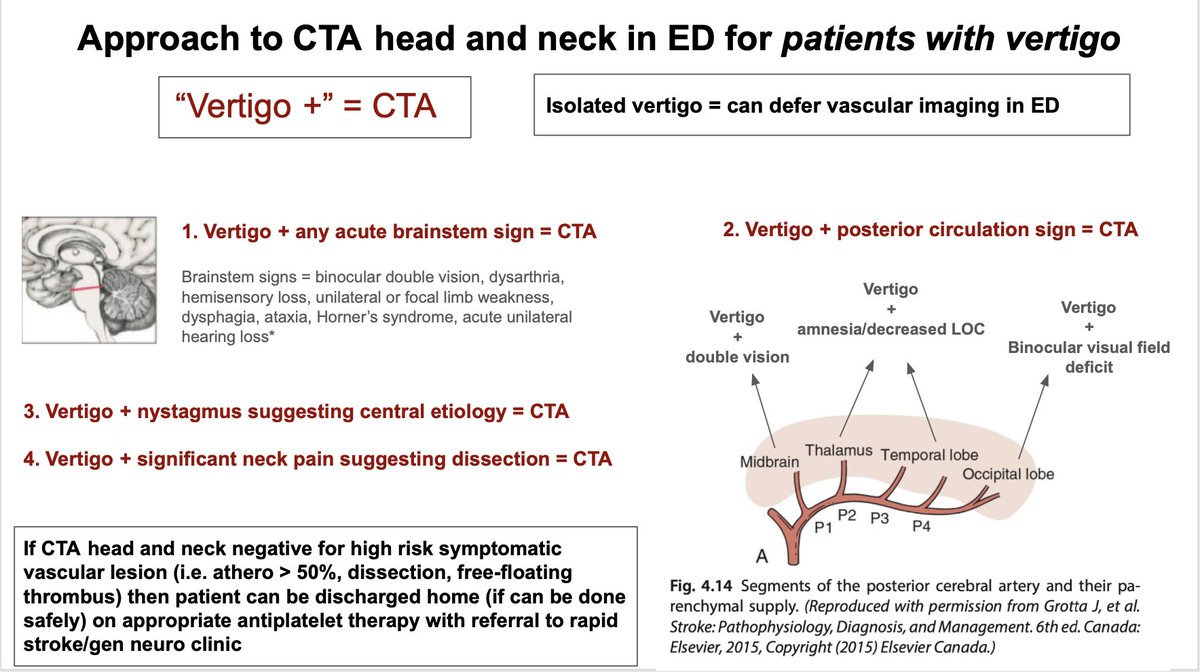
When should you do CTA head and neck in the ED for patients presenting with vertigo?
Below is a "vertigo +" approach to help risk-stratify who can be safely discharged to rapid clinic where further neuroimaging with MRI brain can be considered.
#neurotwitter#stroke#neurology