We're excited to welcome @cliffreid as one of our keynote speakers at #SASNoosa2026. Join us at the Elysium Noosa Resort Fri 28th Aug (& don't forget the Airway SIG meeting on Thu 27th).
Workshops, panel discussions, guideline launches & more.
Details: https://t.co/0fYRRnFaT6
Haemodynamic equations are useful. But they also mislead.
Take:
CO = HR × SV
CO ≈ (MAP − RAP) / SVR
Both are mathematically true. But they can make the variables they contain look like the controllers of output.
Often they are not.
In the intact circulation, these equations describe the resolved state of the system. They do not, by themselves, tell you what is supplying energy, what is constraining flow, or what is actually limiting output.
That is one of the central themes of our review:
Energy, flow and pressure in the cardiovascular system: a narrative review of how the circulation works.
https://t.co/L19bsDCzr6
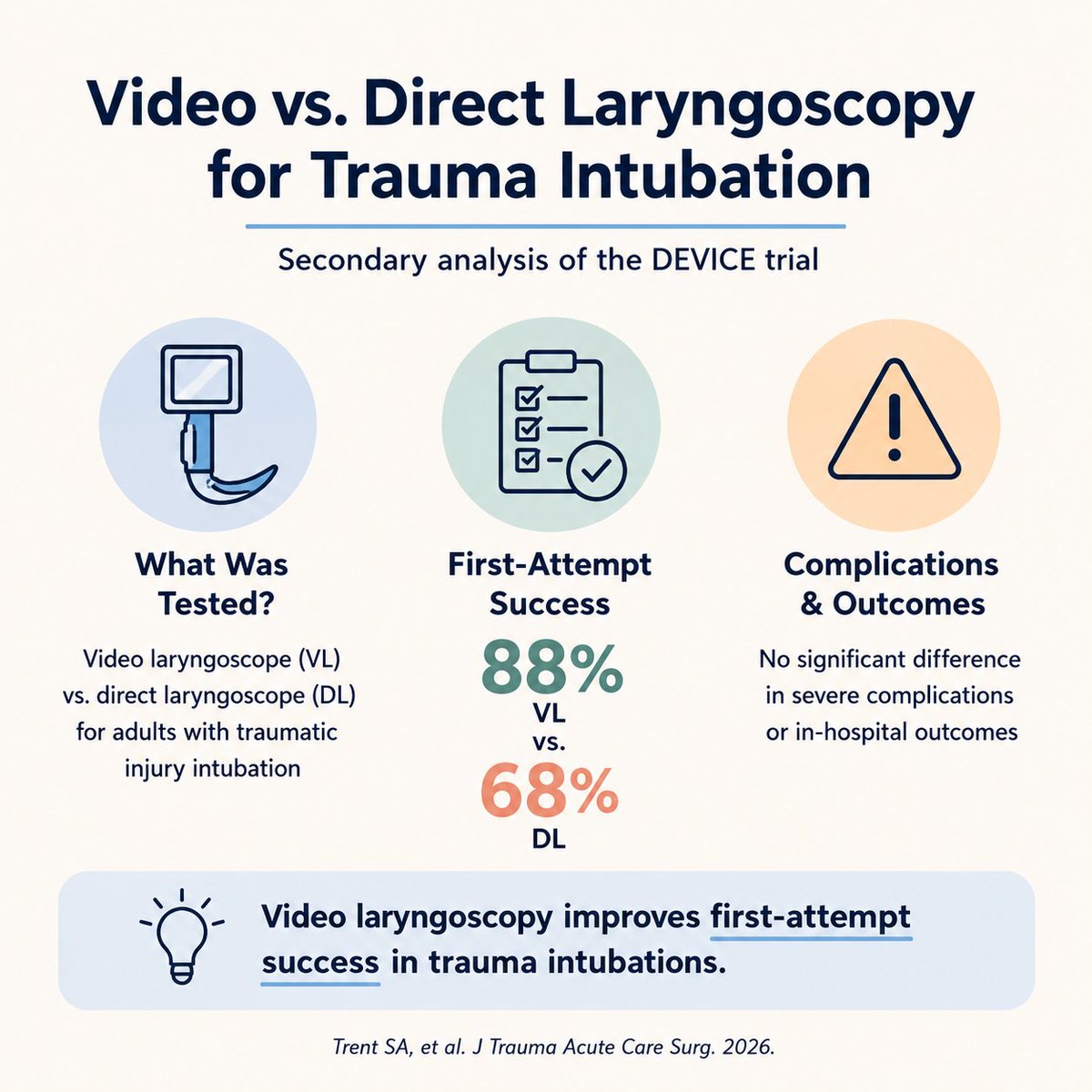
Our secondary analysis of patients intubated for traumatic indications from the DEVICE study is out now. Unsurprisingly, VL out performed DL with an NNT of 5.
https://t.co/aeuE3I2njH
DM me for the full paper.
#emergency#icu#airway#trauma#science#medx#medtwitter
Delighted to see this editorial published in Resuscitation
Described as hard hitting it addresses
- the ongoing and unacceptable high rates of unrecognised oesophageal intubation in some out of hospital settings
- current methods to reduce this
- future opportunities to make this even more failsafe
https://t.co/IgnYxHvPqE
20 years ago today, 3 years before he was slain by depression, David Foster Wallace delivered his unforgettable meditation on the meaning of life – perhaps the greatest commencement address of all time https://t.co/SqaJx9Covr
Does it really matter which IO site you choose?
Well, it depends on how important flow rates are for what you are looking to infuse.
Here's some IV flow rates for comparison:
14g = 330 ml/min
16g = 193 ml/min
18g = 95 ml/min
20g = 61 ml/min
With a pressure bag, here's what you can expect from IO by type and site:
EZ-IO in tibia = 69-165 ml/min
EZ=IO in humerus = 60-153 ml/min
FAST1 in sternum = 112 ml/min (does anyone actually use these now?)
So, back to the original question... for the vast majority of indications, it does not matter which site you choose. We frequently do not resuscitate through 14g IV's, thus, both commonly used IO sites will provide you nearly similar flow rates on pressure bag to the usual IV access catheters.
Clip from The Pitt on @streamonmax
https://t.co/RJuX9wDa6O
PMID: 27075364
#emergency #emergencymedicine #criticalcare #icu #airway #medic #science #data #research #army #armymedicine #armyemdoc #medic #prehospital #medx #medtwitter
Revisit a February 2024 review article on the concept of consciousness, how it is altered by anesthetics, the challenges for assessing consciousness, currently used technologies for assessing anesthesia levels, and future research directions: https://t.co/BZnAMHCZ9a
Exposure to nature doesn’t only make us happier. It makes us kinder too.
Data: Just recalling or seeing photos of forests, oceans, landscapes, or the stars is enough to evoke awe and motivate helping.
The outdoors strengthens our connection to something larger than ourselves.
Female physicians still face systemic barriers and internalised biases, limiting professional opportunities, undermining success and taking significant emotional and psychological tolls. #SexismInMedicine
https://t.co/JWGVsDqh09
Does digital intubation work?
There is no good data on this technique in adults.
There is decent data with efficacy in neonates, but their anatomy is different than adults, and more importantly, unlike adults, you can attempt this in neonates without paralysis. In adults, without paralysis, you risk losing your digits.
One mannequin study compared digital intubation with an ET tube alone, ET + stylet, and ET + bougie. The ET + stylet had the best success rate and fastest times.
A systematic review in neonates found a 94% first-pass success rate.
Anecdotally, when I've tried this in an elective setting, my fingers were almost never long enough. So maybe my colleagues who wear size 8+ gloves may have better success at reaching the landmarks.
In an era of VL and other reliable backup devices, such as SGAs, I'm not sure what role this has, if any. Maybe someone out there can tell me what role this should have, if any.
https://t.co/WKNenvaLOz
https://t.co/KWufY07V5O
PMID 30711420, 34265176
Clip from The Pitt at @StreamOnMax
#emergency #emergencymedicine #criticalcare #icu #airway #medic #science #data #research #army #armymedicine #armyemdoc #airway #medx #medtwitter
Great news
WAMM2025 registration now open
www. https://t.co/CqnmdFrelP
Have you booked yet?
@dasairway@dasresidents@WAMM2025
Did someone mention abstracts....
Amiodarone isn’t the answer just because it’s listed first.
Let’s give lidocaine some love!!
Our @AnnalsofEM commentary lays out the argument for lidocaine in VT/VF arrest. Time to rethink your ACLS autopilot. #TwitteRx#EMRx
Free access link: https://t.co/spkTpck1YI
The decision as to whether we should provide bicarb to our critically ill patient takes places every single day. This paper breaks things down amazingly well. Don’t forget to pay attention to the serum CO2. 🎩 tip to the authors.
https://t.co/wtiQFg1wGN
The "J-Curve" of change is a helpful concept when thinking about the trajectory of a change initiative. Leaders assume that they will see early results from the implementation of change but performance often gets worse before it gets better.
There are many reasons for it; disruption to existing systems, people fearful of & getting used to new ways of working; it's a learning curve for the system.
One of the worst things that happens as a result of the J-Curve is "leadership tampering": leaders impatient for results who start to fiddle with the new system before new arrangements get a chance to work through.
There are many things we can do to reduce the impact of the J-Curve:
1) Stay focused on shared purpose & values, giving people the confidence to move towards a different future that is more compelling than the status quo
2) Anticipate that an "implementation lag" may happen and set expectations based on that
3) Provide support - technical, emotional, learning
4) Involve everyone in the change process, so it is done "with" people, not "to" them
5) Adjust, based on learning & feedback, through small test of change
This article is from @dviney who developed the concept of the J-Curve: https://t.co/vu4gwzD0NG.
We’re proud to share that AV’s Dr Ziad Nehme has been recognised on the national stage, receiving the prestigious Peter Doherty Investigator Grant Award at the 2025 NHMRC Research Excellence Awards.
More: https://t.co/uu0woWwzur
📸 credit Hilary Wardhaugh Photography