Can anyone solve this?
• 31-year-old woman
• 3 unexplained miscarriages in a row
• Sudden, massive blood clot in leg
• Suffers a mini-stroke out of nowhere
What is the probable diagnosis?
💔💔💔💔💔💔💔💔💔💔
My best friend called me this evening around 4 p.m. to say he was having chest pain and sweating profusely. I immediately told him to go straight to the hospital. Fortunately, his neighbour was around and rushed him to a nearby hospital.
Unfortunately, that hospital didn't have an ECG machine, so he had to be taken to another hospital. An ECG was done and, when I saw it, it showed a classic heart attack (Anterior MI).
I requested that they start him on Aspirin while transferring him to the teaching hospital, but sadly, they didn't even have Aspirin available. I then told them to rush him to the state teaching hospital. When he got there safely, they were finally able to start him on Aspirin.
However, they informed his friends and neighbours that they did not have a functioning cath lab that could have helped save his life. While I was trying to arrange for him to be moved to Lagos as quickly as possible, my friend died in the ambulance on the way there. It's about a five-hour trip. I was on the phone with them throughout, and this happened about three hours after they left the teaching hospital.
I was supposed to meet this guy next month in the Netherlands.
Nigeria really did me dirty today. How can an entire state not have a functioning cath lab? How? 😢😢😢😢😢😢😢
I'm so broken right now.
Someone is having an active SEIZURE right in front of you. What is the absolute WORST thing you can do that could actually kill them?
A) Pin them down to stop the shaking
B) Put a spoon in their mouth
C) Pour water into their mouth
D) Roll them onto their side
Bonus: Why?
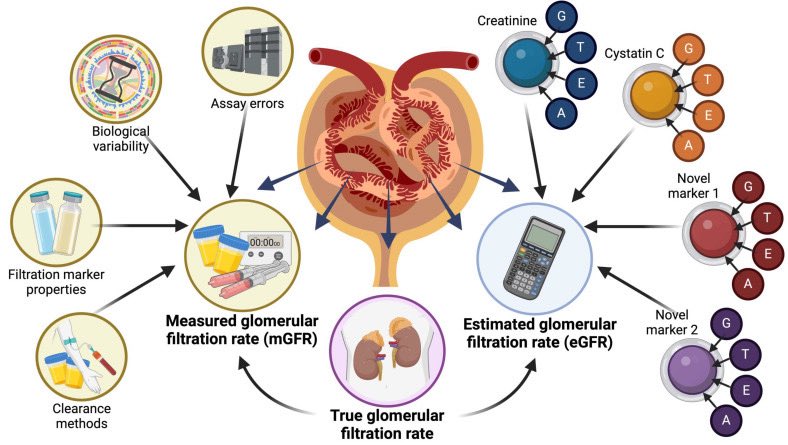
Answer: C) Cystatin C
Among the options, Cystatin C is the most accurate single marker of kidney filtration (glomerular filtration rate, or GFR). It is produced at a constant rate by all nucleated cells, freely filtered by the glomeruli, and almost completely reabsorbed and catabolized in the tubules with minimal tubular secretion or extra-renal clearance. This makes it far less influenced by muscle mass, diet, or other non-renal factors compared to the alternatives.
———————————————
• Serum urea (A) fluctuates wildly with protein intake, hydration, GI bleeding, and liver function.
• Serum creatinine (B) is the most common but imperfect.
• Urine output (D) reflects volume status and tubular function more than precise filtration rate and is unreliable as a standalone GFR marker.
——————————————
Bonus write-up:
Creatinine Lies: Why the Most Popular Kidney Test Misleads Millions
Serum creatinine is the world’s default kidney test, yet it’s a deeply flawed marker of actual filtration (GFR). Produced mainly from muscle breakdown, its blood level depends heavily on muscle mass — so muscular athletes or bodybuilders often register “high” creatinine with perfectly normal kidneys, while frail elderly people, malnourished patients, or amputees can have “normal” creatinine despite significantly reduced GFR.
As kidney function declines, the tubules secrete more creatinine into the urine, causing creatinine-based estimates to overestimate true GFR by 10–20% or more. Extra-renal clearance (mainly gut degradation) also increases in chronic kidney disease, further distorting results. Diet (red meat), certain medications, lab assay variations, and individual biology add even more noise.
The result? Poor sensitivity for early kidney disease, frequent misclassification of CKD stage, and unreliable medication dosing or risk assessment — especially in non-average body types. Equations try to patch this with age, sex, and race adjustments, but they can’t overcome the fundamental biological variability.
That’s why cystatin C — produced constantly regardless of muscle — often gives a clearer, more accurate picture of real filtration when creatinine is questionable. The popular test isn’t useless, but relying on it alone is like judging a car’s performance by its speedometer while ignoring the engine.
#MedTwitter #MedEd #MerX @IhabFathiSulima
Which of these is the strongest warning sign that a MOLE might actually be a deadly skin cancer?
A) It is raised like a bump
B) It has a hair growing out of it
C) It has multiple different colors
D) It hurts when you press it
Bonus: What are the other major warning signs?
Approach to Hypocalcemia for HO/Medical officers/Residents:
A calcium report comes back low. Don’t jump straight to calcium replacement.
Use this approach:
A patient in the ER refused his Tetanus shot stating: "Doc, why do I need it? The nail I stepped on was shiny and wasn't even rusty!"
The biggest myth in medicine is that ONLY Rust = Tetanus.
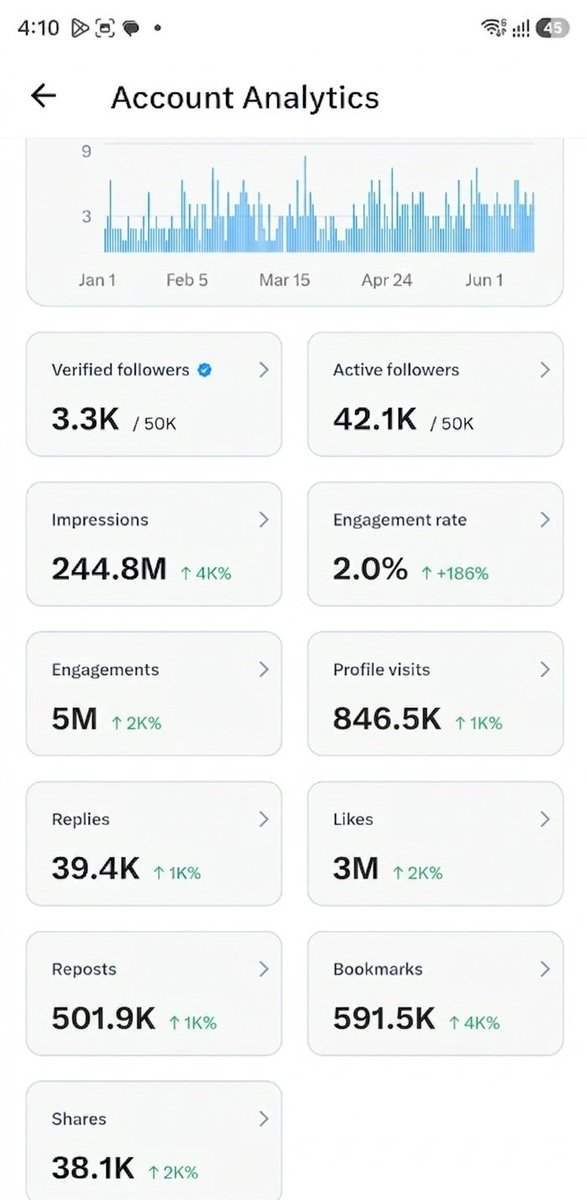
50,000 Followers! 🎉
On January 1st 2026, I started the year with just 1.5K followers. To see this community grow from 1.5K to 50k in less than six months is absolutely surreal. I am incredibly thankful for the support.
I am truly glad that my posts are helping Med Twitter break out of its niche. By reaching the non-medico zone, we are giving the whole Med Twitter community the much broader exposure it deserves.
The way we have all interacted over the new formats I have created namely
🔹 The "Patient Asks..." clinical scenarios
🔹 The classic MCQ with a Bonus format
🔹 The Clinical Mystery format and etc..
has been incredible. Seeing so many of you adopt these styles and build on them is what truly makes Med Twitter the absolute best place on this app to learn.
Knowing that these posts are reaching millions of non-medico people every single day and that they are genuinely learning from them is the greatest reward.
Last but certainly not least, I am also constantly learning from the other brilliant Med Twitter accounts I interact with every day. The knowledge sharing goes both ways, and I am grateful for those conversations.
Thank you all for being part of this journey. Let’s keep building and learning together!
My last 5.5 month Stats below 👇
The correct answer is C) HPV (Genital Warts)
We have had it drilled into our heads that condoms are a flawless shield. While they work incredibly well against infections spread through bodily fluids (like HIV or Chlamydia), they have a massive anatomical blindspot here.
Bonus Answer:
Why? Because HPV (and also Herpes) don't rely on fluids to travel, they spread via skin-to-skin contact.
A condom only covers the shaft of the penis. Any friction or contact with the surrounding uncovered skin like the scrotum, groin or vulva is more than enough to transmit the virus. They reduce the risk, but not at all fullproof. This is why tools like the HPV vaccine are so critical!
FOLLOW ME for more such posts!
A junior doctor in the casualty asked me: "Sir, two patients just arrived. One has a BP of 200/120, the other is at 80/50. Who do we prioritize first?"
My answer: Go look at their faces.
On Tuesday, 2nd June, 2026, I was finally inducted into the medical profession.
I emerged as the best graduating student and only 7-star general in the history of Obafemi Awolowo College of Health Sciences, Olabisi Onabanjo University @oou_agoiwoye.
Presenting:
Best Graduating Doctor, 32nd set of graduating doctors, OACHS, OOU
Best Academic Result in OACHS, OOU history at time of graduation
Distinction in Anatomy
Distinction in Physiology
Distinction in Biochemistry
Distinction in Pathology
Distinction in Pharmacology