The DOJ’s cuts to Community Violence Intervention (CVI) programs are not just a policy shift—they’re a step backward at a time when we can least afford it. Let’s be clear about what this means: more shootings, more trauma, and more patients on our operating tables and in our trauma bays.
CVI isn’t abstract. It’s a public health approach to gun violence that centers on the individuals and communities most at risk. CVI teams—made up of trusted, trained community members, often with lived experience—work in neighborhoods, hospitals, and schools to interrupt cycles of violence, mediate conflicts, and connect people to jobs, education, housing, and mental health care. The data speaks volumes. In cities that have implemented CVI models with fidelity—like Oakland, New York, and Chicago—firearm homicides have dropped by 30 to 60%. Hospital-based violence intervention programs (HVIPs) have reduced reinjury rates by up to 50% and helped stabilize families during some of the most dangerous and traumatic moments in their lives.
This work is bipartisan. Governors and mayors across the political spectrum have embraced CVI because it delivers results. It’s grounded in science, driven by communities, and more cost-effective than downstream emergency and incarceration costs.
And yet, despite this evidence—and in the face of rising youth firearm deaths—federal CVI funding is on the chopping block. That’s not just fiscally short-sighted. It’s dangerous. As a trauma surgeon, I’ve seen what happens when we don’t intervene upstream. When a young person arrives in the trauma bay with a gunshot wound, it’s not just a clinical emergency—it’s a failure of systems. We should be doing everything we can to keep people out of harm’s way in the first place.
These cuts will ripple across the country, weakening the very networks that have been preventing violence every day—quietly, effectively, and without fanfare. We should be scaling CVI. Embedding it in Medicaid. Making it part of hospital accreditation and community benefit. Instead, we’re gutting its core support.
TEAL | For National Trauma Survivors Day.
“The MetroHealth System Trauma Recovery Center recognizes and celebrates National Trauma Survivors Day. This day honors survivors and caregivers and draws inspiration from their incredible triumphs, while also helping initiate healing from trauma.” @metrohealthCLE
This program is the latest step in our holistic approach toward enhancing public safety in Ohio by ensuring that our communities have the resources they need to protect and support the public. @Ohio_OCJS
More information: https://t.co/I4RoYAZDUE
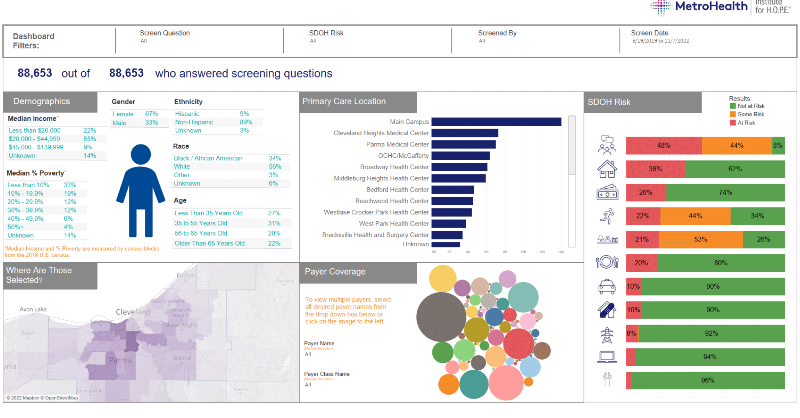
Health systems should systematically screen all patients for social drivers of health, partner with community organizations to provide assistance, develop their own programs, and conduct research for improvement: https://t.co/fGwHRVS9Bj @metrohealthCLE@SueFuehrer@MegenSimpson
"They (Cincinnati) are far ahead of the game - the first in the country to already be sending calls back and forth from 988 to 911." - Josiah Quarles @clevhomeless on #CityClub
"I think what's critical to think about in these is making sure that initiatives are properly supported and properly staffed and when we think about one of the major challenges in behavioral health world right now - it's staffing." - Joan Englund @MHAC_Ohio#CityClub
"The lingering effects of #trauma can grow in isolation, and this important funding ensures that survivors continue to have access to dedicated professionals and services on their journey of healing." https://t.co/FOSheVzlyg
My friend Heather Vallier, President of @otatrauma, watching Dr Patterson’s tribute prior to her speech. I have never met a more well-balanced, kind, and strong person in ortho. She mentored me of her own volition when I wasn’t her resident/fellow. The OTA is lucky to have her.🥰
Phenomenal opening symposium discussing the impact of trauma, moral injury and burnout among surgeons. Well done, @otatrauma thank you for bringing this up! We are here for it! #ota2021