Husband. Dad. EP. Extractor. Implanter. Ass Prof 😯 49 post-nominals: anyone have a spare one to even it up? Royal Melbourne Hospital. 🇬🇧 in 🇦🇺. Quite ranty
Need to help #Epeeps patients understand their condition?
Over 1000 copies given out so far, now available for Kindle (tried to make it completely free but Amazon wouldn't let me 😞). Hard copy available soon. @drjohnm@narrowQRS
https://t.co/rUSzOZ2cgV
@DavidLBrownMD There may be issues with today's approach but this is still a really bad thing that happened. I agree with much of your approach and qualified 23 years ago but any Doc should be able to understand the need to recover properly from critical illness, irrespective of profession.
@tylerblack32 There use to be though, before gell came in pads and then we switched to stick-on patches rather than paddles.
You also don't need to stand clear. Ad a cardiac EP, I am usually holding my patients tightly when they get cardioverted
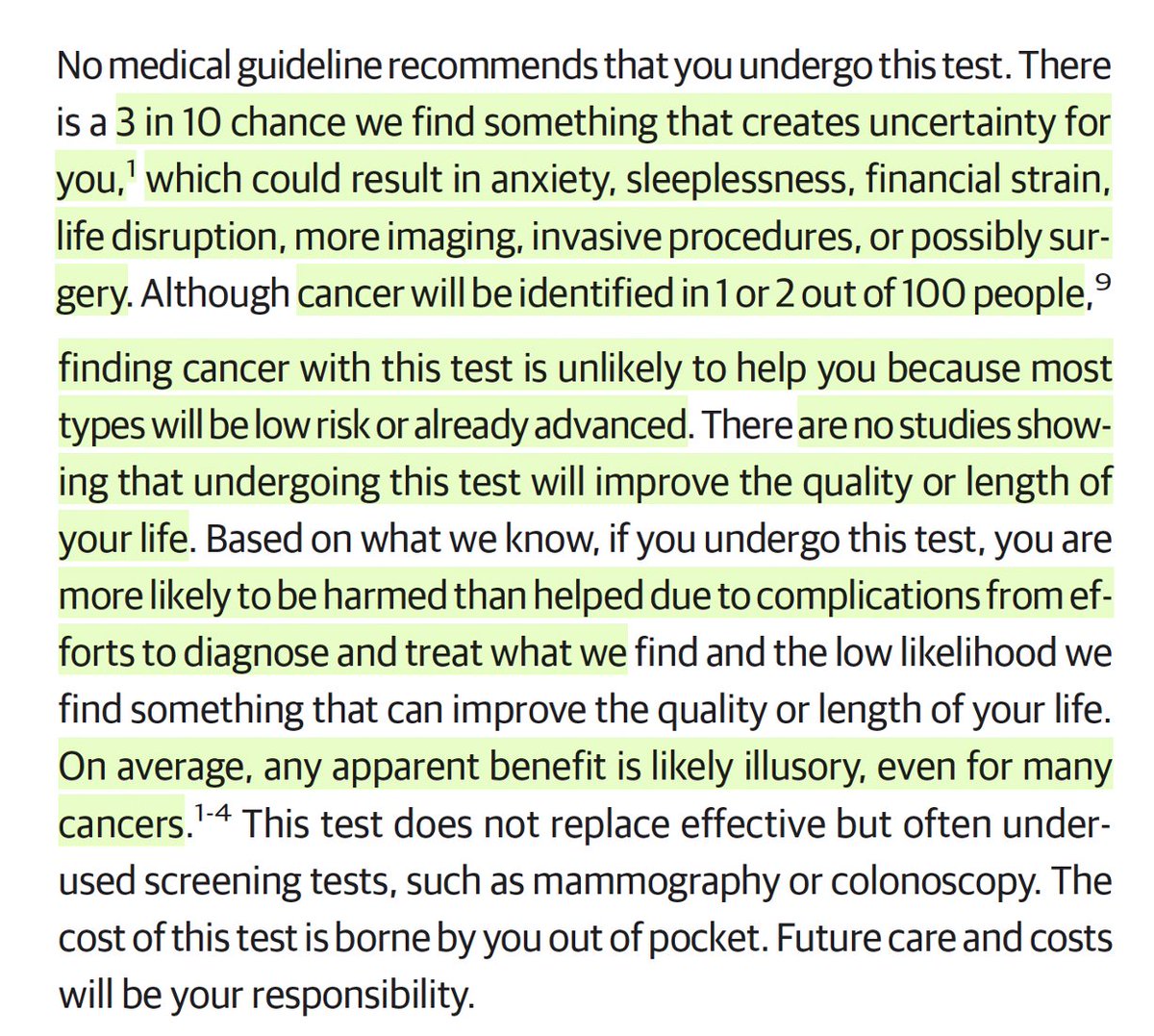
At @JAMA_current today, 2 radiologists publish what should be the consent form for a total body MRI in healthy people
Note: "no major medical society recommends whole-body MRI screening in the general population because it is unproven, and the harms likely outweigh the benefits."
https://t.co/TRSkxDwb6K
Zero Fluoro-guided ablation for AF substantially reduces radiation exposure without evidence of higher procedural complication, 12-month freedom from atrial arrhythmia recurrence or procedure duration #OpenAccess
https://t.co/oskh8VrxaQ
For the love of God #EPeeps journals - please can PFA catheters be described by their trade names rather than theses stupid circular array / penta-spline / lattice tip / variable loop descriptions that are no less bloody specific!!!!!
More than 10 years ago Oussama and I started our journey of investigation, trying to the define the optimal first treatment for patients with atrial fibrillation.
Separately we pursed randomised studies in populations with treatment-naive paroxysmal AF.
Five years ago we presented our RCTs in the paroxysmal AF population, which ended up sitting side by side in the same issue of the New England Journal of Medicine.
https://t.co/DWgHQ2VhiJ
https://t.co/z346xqq0jg
Since then we have been working together to examine the same question of optimal initial therapy, but instead looking at patients with more advanced forms of atrial fibrillation.
Today Oussama presented the results of the AVANT-GUARD study, which definitively demonstrated the value of initial catheter ablation in the treatment naive persistent AF population.
Like EARLY-AF, AVAT GUARD used implantable cardiac monitors to evaluate arrhythmia endpoints
Like EARLY-AF - initial catheter ablation reduced recurrences in AVANT GUARD by about 50%, which was about 25% in absolute terms. To put this another way, only 4 patients need to be treated with ablation to prevent a recurrence of arrhythmia.
However, binary recurrence doesn’t tell the whole story. Because we had loop recorders we were able to assess the time spent in AF (or AF burden). In this regard significantly more patients had none or negligible burden after ablation (<0.1%), with significantly more AAD treated patients having a very high burden (>5%). This is important as AF burden is associated with clinical outcomes such as hospitalisation.
In terms of risk - the rates of any adverse event or serious adverse event were comparable between randomised arms. Highlighting that persistent AF patients with high CHADS-VASc score are high risk irrespective of treatment provided. This is important as we reflect on treatment options as part of shared decision-making.
Congratulations to Oussama for the presentation and leadership, to the co-investigators and study sites for their participation and dedication, and a huge thank you to the Boston Scientific team for their support and commitment to advancing science.
To end, I want to acknowledge and thank Oussama for this shared journey, I’m grateful for our collaboration and friendship, and look forward to what we will do next.
Hot off the press
2026 @HRSonline#CIED management guidelines just dropped - and these ones have a real pulse!
Honored to contribute and represent @IDSAInfo@bcmhouston@BCMCME
https://t.co/7K1W3JxwVC
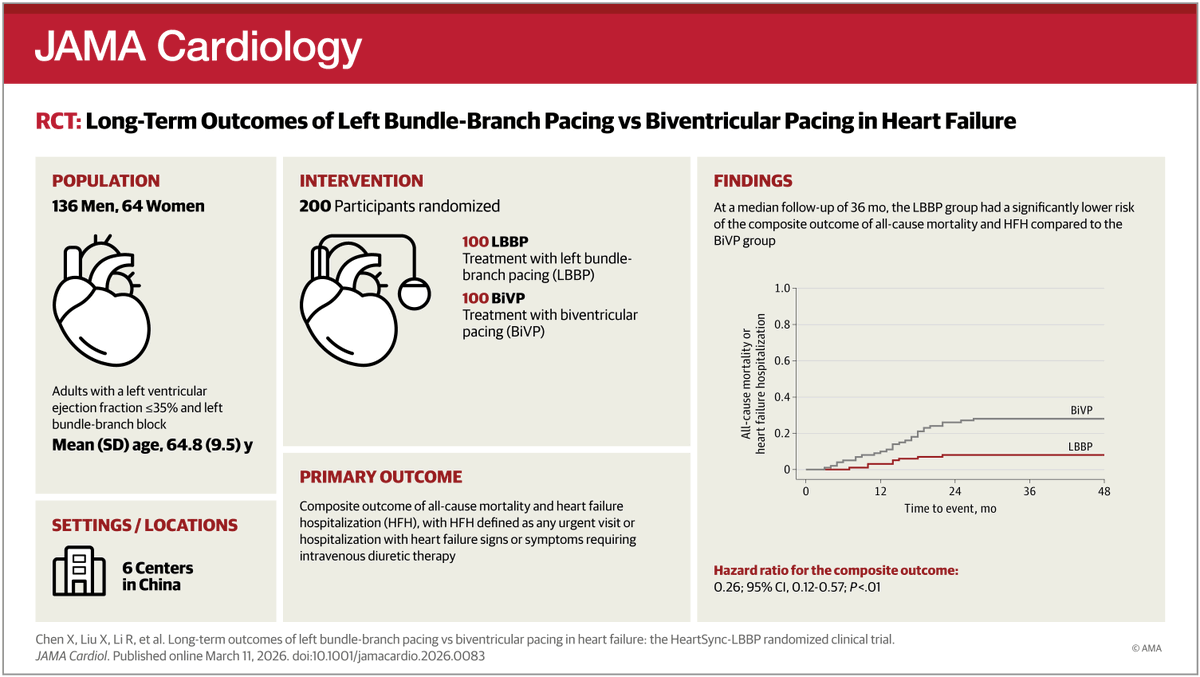
Errr @JAMACardio... publishing PhysioSync-HF (LBBAP inferior) and HeartSync-LBBB (CSP superior) simultaneously is certainly confusing but I think you are supposed to know the difference between the two studies 😬
In patients with #HeartFailure and #LBBB, conduction system pacing (#CSP) was inferior to biventricular pacing (#BiVP) for a composite of death, heart failure events, and LVEF change at 12 months.
https://t.co/a3Tlkre65B
Open access... @drjohnm@DrJasonAndrade@epfellow@karan_chauhan3
Safety of catheter ablation compared with antiarrhythmic drugs for atrial fibrillation: A systematic review and meta-analysis of randomized trials - Heart Rhythm https://t.co/0xEhPE2Myj
@BElbarouni@Hragy Errr because of the protocol....
(Or if you mean: why did they do this? I presume it was because ORBITA was negative but ORBITA 2 was positive)